
Ultrasound in the Differential Diagnosis of Medial Epicondylalgia and Medial Elbow Pain—Imaging Findings and Narrative Literature Review


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Epidemiology of Medial Epicondylalgia
3.2. Causes and Other Risk Factors
Symptoms of Medial Epicondylalgia
3.3. Pathophysiology of Medial Epicondylalgia
3.4. Diagnosis
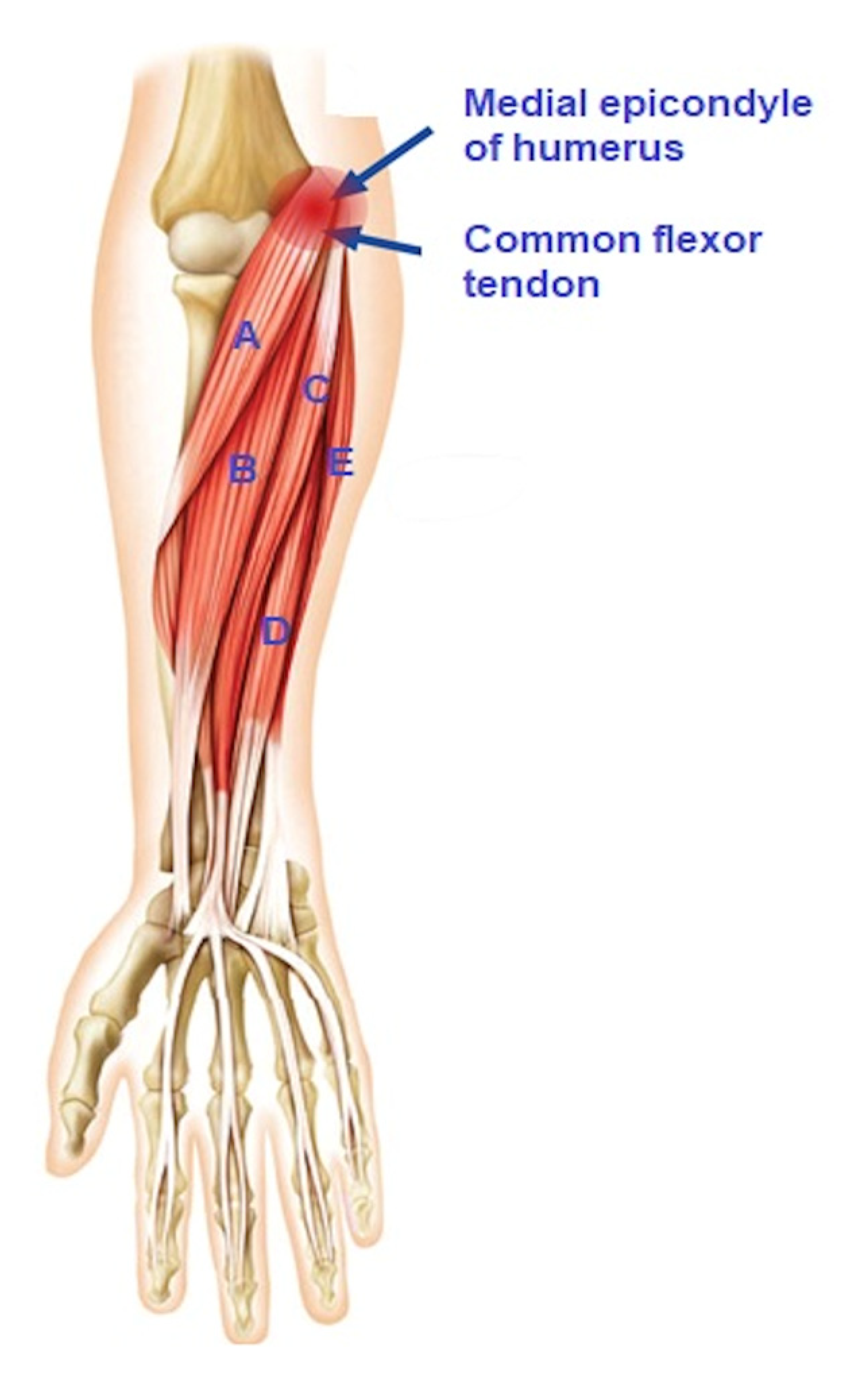
3.4.1. Normal Anatomy of the Medial Epicondyle Region
3.4.2. Clinical Diagnosis
3.4.3. Imaging of Medial Epicondylalgia
3.4.4. Radiography
3.4.5. Magnetic Resonance Imaging
3.4.6. Ultrasonography
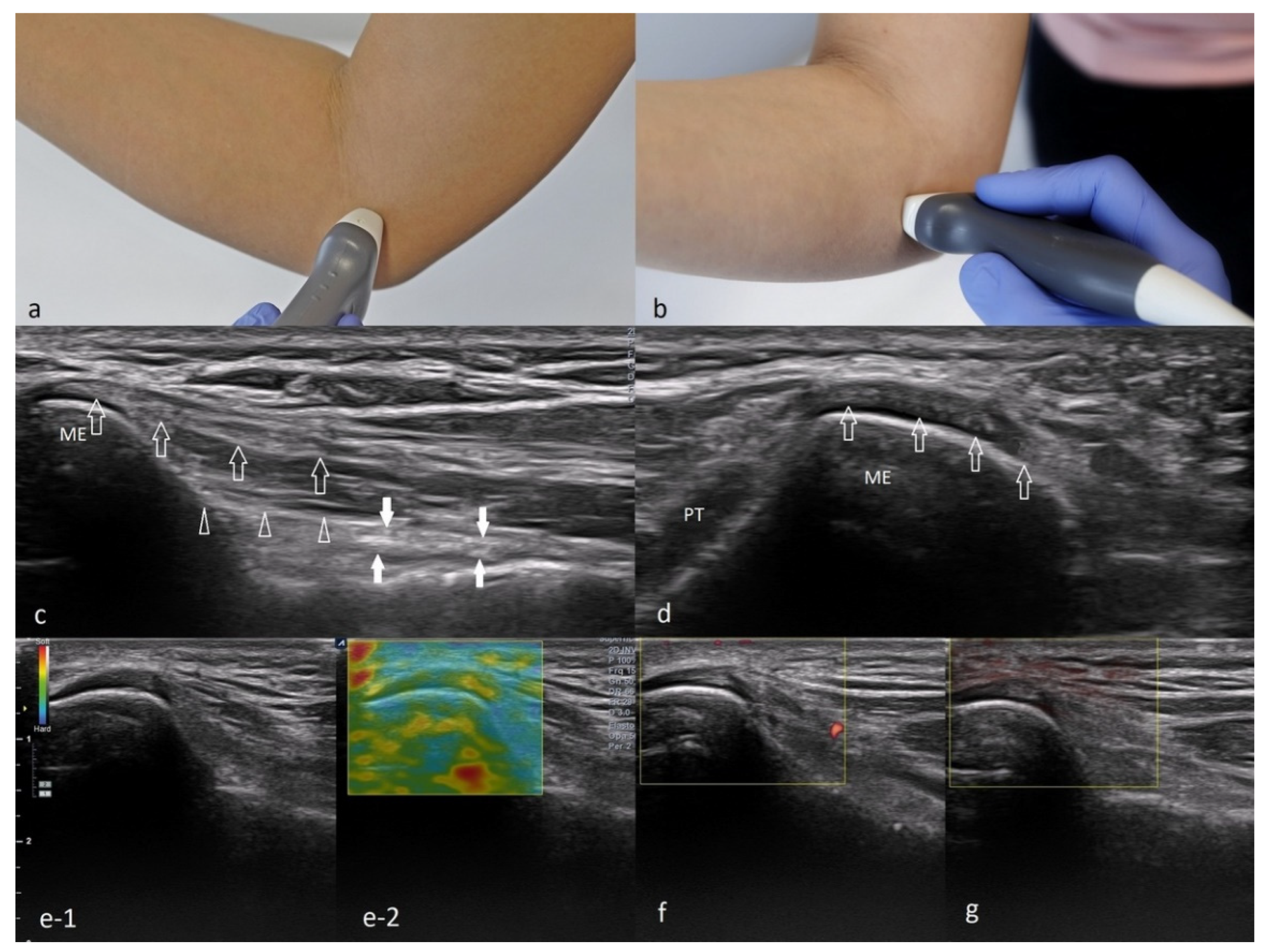
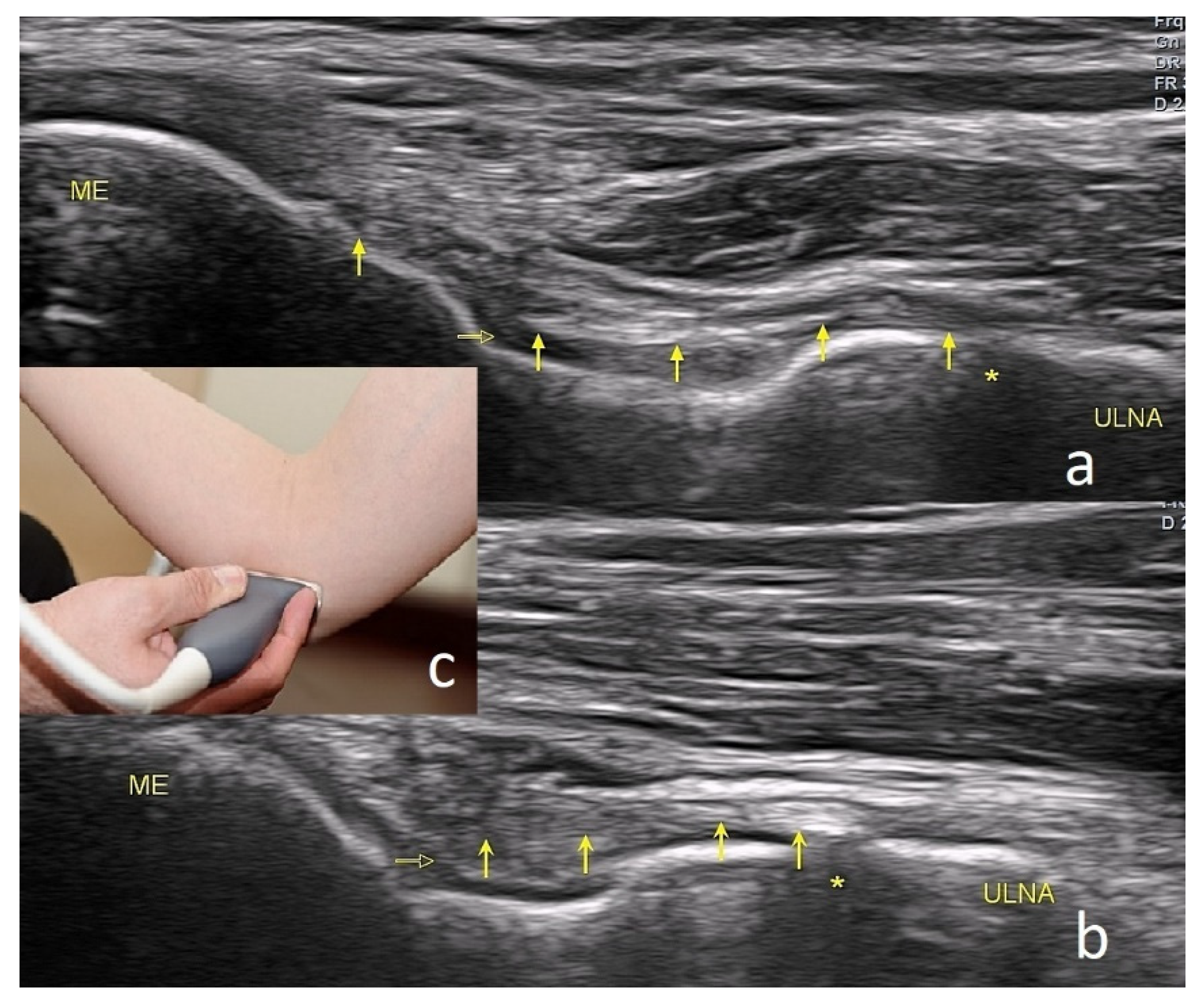
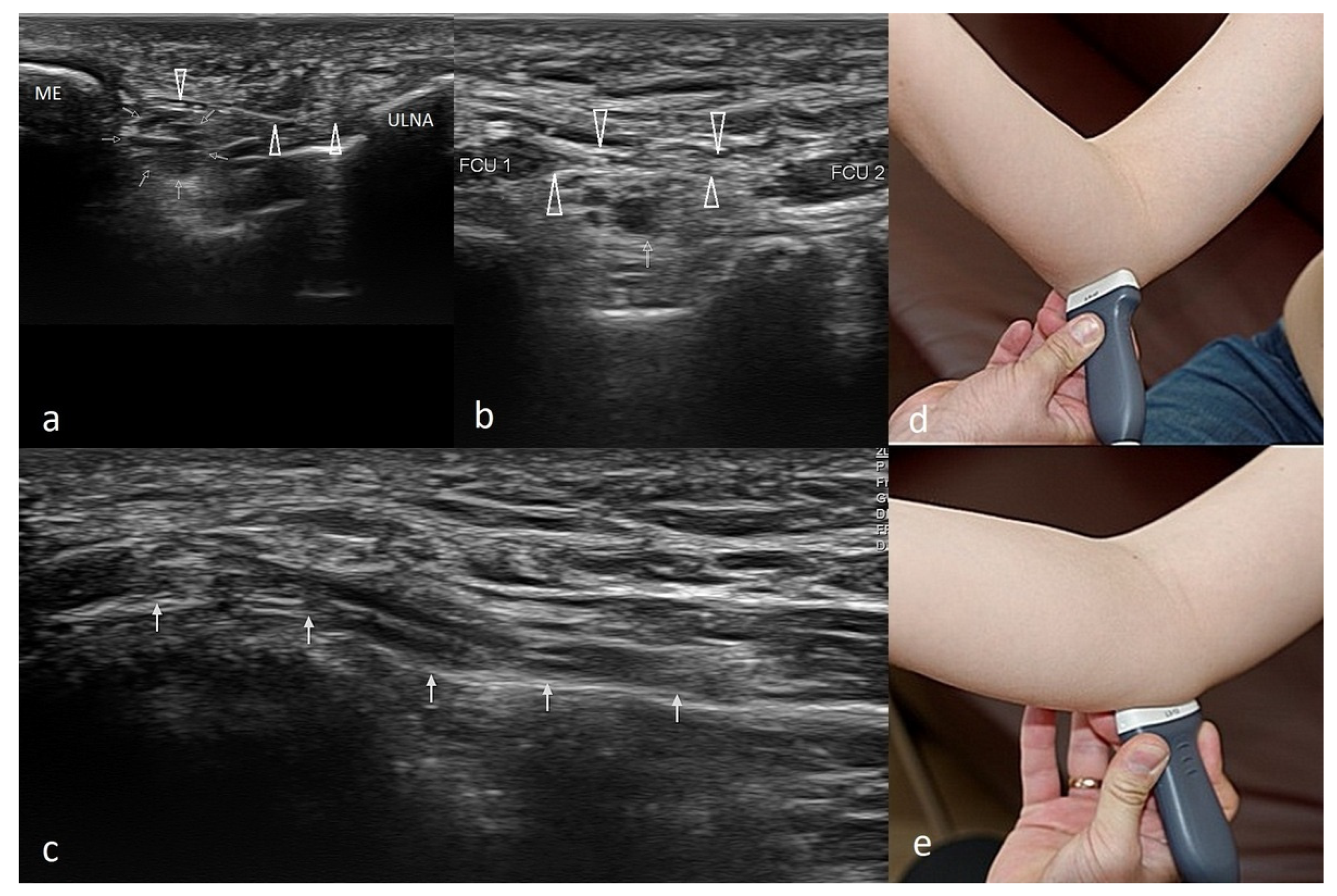
The Technique of Ultrasound Examination of the Medial Portion of the Elbow



4. Discussion
4.1. Cubital Tunnel Syndrome and Ulnar Neuritis
4.2. Snapping Triceps with Ulnar Neuritis
4.3. Ulnar Nerve Compression Caused by Anconeus Epitrochlearis
4.4. Ulnar Collateral Ligament Injury
4.5. Cervical Radiculopathy
4.6. Ganglion Cyst
4.7. Degenerative Changes in the Elbow Joint
4.8. Epitrochlear Lymphadenopathies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Morrey, B.F. (Ed.) The Elbow and Its Disorders, 3rd ed.; WB Saunders: Philadelphia, PA, USA, 2000. [Google Scholar]
- Matthews, J.; Boyle, K. Tennis and Golfer’s Elbow: Epicondylitis. In Orthopedic Surgery Clerkship; Eltorai, A.E.M., Eberson, C.P., Daniels, A.H., Eds.; Springer International Publishing: Cham, Germany, 2017; pp. 87–90. [Google Scholar]
- Morris, H. The rider’s sprain. Lancet 1882, 120, 133–134. [Google Scholar] [CrossRef]
- Hultman, K.L.; Goldman, B.H.; Nazarian, L.N.; Ciccotti, M.G. Ultrasound Examination Techniques for Elbow Injuries in Overhead Athletes. J. Am. Acad. Orthop. Surg. 2021, 29, 227–234. [Google Scholar] [CrossRef]
- Kane, S.F.; Lynch, J.H.; Taylor, J.C. Evaluation of elbow pain in adults. Am. Fam. Physician 2014, 89, 649–657. [Google Scholar]
- Barret, H.; Gastaud, O.; Laumonerie, P.; Faruch, M.; Bonnevialle, N.; Mansat, P.; Langlais, T. Feasibility and technique of ultrasound traumatic elbow lesion assessment. Orthop. Traumatol. Surg. Res. 2021, 107, 102836. [Google Scholar] [CrossRef]
- Jeong, J.S. Dual-element transducer with phase-inversion for wide depth of field in high-frequency ultrasound imaging. Sensors 2014, 14, 14278–14288. [Google Scholar] [CrossRef] [PubMed]
- Jäschke, M.; Weber, M.A. Sonographie des Ellenbogens—Standardschnitte und Normalanatomie [Ultrasound of the elbow-standard examination technique and normal anatomy]. Radiologe 2018, 58, 985–990. [Google Scholar] [CrossRef] [PubMed]
- Entrekin, R.R.; Porter, B.A.; Sillesen, H.H.; Wong, A.D.; Cooperberg, P.L.; Fix, C.H. Real-time spatial compound imaging: Application to breast, vascular, and musculoskeletal ultrasound. Semin. Ultrasound. CT MR 2001, 22, 50–64. [Google Scholar] [CrossRef]
- Amin, N.H.; Kumar, N.S.; Schickendantz, M.S. Medial epicondylitis: Evaluation and management. J. Am. Acad. Orthop. Surg. 2015, 23, 348–355. [Google Scholar] [CrossRef]
- Plancher, K.D.; Halbrecht, J.; Lourie, G.M. Medial and lateral epicondylitis in the athlete. Clin. Sports Med. 1996, 15, 283–305. [Google Scholar] [CrossRef]
- Descatha, A.; Dale, A.M.; Jaegers, L.; Herquelot, E.; Evanoff, B. Self-reported physical exposure association with medial and lateral epicondylitis incidence in a large longitudinal study. Occup. Environ. Med. 2013, 70, 670–673. [Google Scholar] [CrossRef]
- Descatha, A.; Leclerc, A.; Chastang, J.F.; Roquelaure, Y. Study Group on Repetitive Work. Medial epicondylitis in occupational settings: Prevalence, incidence and associated risk factors. J. Occup. Environ. Med. 2003, 45, 993–1001. [Google Scholar] [CrossRef]
- Shiri, R.; Viikari-Juntura, E.; Varonen, H.; Heliövaara, M. Prevalence and determinants of lateral and medial epicondylitis: A population study. Am. J. Epidemiol. 2006, 164, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Shiri, R.; Viikari-Juntura, E. Lateral and medial epicondylitis: Role of occupational factors. Best Pract. Res. Clin. Rheumatol. 2011, 25, 43–57. [Google Scholar] [CrossRef]
- Walker-Bone, K.; Palmer, K.T.; Reading, I.; Coggon, D.; Cooper, C. Occupation and epicondylitis: A population-based study. Rheumatology 2012, 51, 305–310. [Google Scholar] [CrossRef]
- Ciccotti, M.C.; Schwartz, M.A.; Ciccotti, M.G. Diagnosis and treatment of medial epicondylitis of the elbow. Clin. Sports Med. 2004, 23, 693–705. [Google Scholar] [CrossRef] [PubMed]
- Sluiter, J.K.; Rest, K.M.; Frings-Dresen, M.H. Criteria document for evaluating the work-relatedness of upper-extremity musculoskeletal disorders. Scand. J. Work Environ. Health 2001, 27, 1–102. [Google Scholar] [CrossRef]
- Jobe, F.W.; Ciccotti, M.G. Lateral and Medial Epicondylitis of the Elbow. J. Am. Acad. Orthop. Surg. 1994, 2, 1–8. [Google Scholar] [CrossRef]
- van Rijn, R.M.; Huisstede, B.M.; Koes, B.W.; Burdorf, A. Associations between work-related factors and specific disorders at the elbow: A systematic literature review. Rheumatology 2009, 48, 528–536. [Google Scholar] [CrossRef]
- Erdem, Y.; Neyisci, C. Lateral and Medial Epicondylitis: Definition, Diagnosis, Screening and Treatment Algorithms, Work-Related Musculoskeletal Disorders; IntechOpen: Ankara, Turkey, 2019. [Google Scholar]
- Reece, C.L.; Susmarski, A. Medial Epicondylitis. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK557869/ (accessed on 19 April 2022).
- Brady, C.; Dutta, A. Medial epicondylitis and medial elbow pain syndrome: Current treatment strategies. J. Musculoskelet Disord. Treat. 2016, 2, 1–5. [Google Scholar] [CrossRef]
- Copas, D.; Talbot, J.C. Clinical assessment of the elbow. Orthop. Trauma 2016, 30, 291–300. [Google Scholar] [CrossRef]
- Ciccotti, M.G. Epicondylitis in the athlete. Instr. Course Lect. 1999, 48, 375–381. [Google Scholar] [CrossRef]
- Zahn, K.V.; Byerly, D.W. Medial Epicondyle Injection. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Boyd, H.B.; McLeod, A.C., Jr. Tennis elbow. J. Bone Jt. Surg. Am. 1973, 55, 1183–1187. [Google Scholar] [CrossRef]
- Regan, W.; Wold, L.E.; Coonrad, R.; Morrey, B.F. Microscopic histopathology of chronic refractory lateral epicondylitis. Am. J. Sports Med. 1992, 20, 746–749. [Google Scholar] [CrossRef] [PubMed]
- Kiel, J.; Kaiser, K. Golfers Elbow. [Updated 2021 July 25]; In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK519000/ (accessed on 19 April 2022).
- Otoshi, K.; Kikuchi, S.; Shishido, H.; Konno, S. The proximal origins of the flexor–pronator muscles and their role in the dynamic stabilization of the elbow joint: An anatomical study. Surg. Radiol. Anat. 2014, 36, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Radunovic, G.; Vlad, V.; Micu, M.C.; Nestorova, R.; Petranova, T.; Porta, F.; Iagnocco, A. Ultrasound assessment of the elbow. Med. Ultrason. 2012, 14, 141–146. [Google Scholar]
- Gołąb, B.K. (Ed.) Anatomia i Fizjologia Człowieka: Podręcznik dla Studentów Wydziałów Farmacji, Zdrowia Publicznego, Analityki Medycznej, Pielęgniarstwa, Biologii i Nauki o Ziemi, Studiów Kosmetycznych i Innych; Ośrodek Doradztwa i Szkolenia “TUR”: Łódź, Jaktorów, 1997. [Google Scholar]
- Terranova, L.M. Medial Epicondylitis. In Musculoskeletal Sports and Spine Disorders: A Comprehensive Guide; Kahn, S.B., Xu, R.Y., Eds.; Springer International Publishing: Cham, Germany, 2017; pp. 93–95. [Google Scholar]
- Barco, R.; Antuña, S.A. Medial elbow pain. EFORT Open Rev. 2017, 2, 362–371. [Google Scholar] [CrossRef] [PubMed]
- van der Molen, H.F.; Visser, S.; Alfonso, J.H.; Curti, S.; Mattioli, S.; Rempel, D.; Roquelaure, Y.; Kuijer, P.P.; Tamminga, S.J. Diagnostic criteria for musculoskeletal disorders for use in occupational healthcare or research: A scoping review of consensus- and synthesised-based case definitions. BMC Musculoskelet Disord. 2021, 22, 169. [Google Scholar] [CrossRef] [PubMed]
- Zwerus, E.L.; Somford, M.P.; Maissan, F.; Heisen, J.; Eygendaal, D.; van den Bekerom, M.P. Physical examination of the elbow, what is the evidence? A systematic literature review. Br. J. Sports Med. 2018, 52, 1253–1260. [Google Scholar] [CrossRef]
- Ciccotti, M.G.; Ramani, M.N. Medial epicondylitis. Tech. Hand Up Extrem. Surg. 2003, 7, 190–196. [Google Scholar] [CrossRef]
- Pienimäki, T.; Siira, P.; Vanharanta, H. Widespread pain in chronic epicondylitis. Eur. J. Pain. 2011, 15, 921–927. [Google Scholar] [CrossRef]
- Polkinghorn, B.S. A novel method for assessing elbow pain resulting from epicondylitis. J. Chiropr. Med. 2002, 1, 117–121. [Google Scholar] [CrossRef]
- Donaldson, O.; Vannet, N.; Gosens, T.; Kulkarni, R. Tendinopathies around the Elbow Part 2: Medial Elbow, Distal Biceps and Triceps Tendinopathies. Shoulder Elb. 2014, 6, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Kijowski, R.; De Smet, A.A. Magnetic resonance imaging findings in patients with medial epicondylitis. Skelet. Radiol. 2005, 34, 196–202. [Google Scholar] [CrossRef]
- Park, G.Y.; Lee, S.M.; Lee, M.Y. Diagnostic value of ultrasonography for clinical medial epicondylitis. Arch. Phys. Med. Rehabil. 2008, 89, 738–742. [Google Scholar] [CrossRef] [PubMed]
- American College of Radiology (ACR); Society for Pediatric Radiology (SPR); Society of Radiologists in Ultrasound (SRU). AIUM practice guideline for the performance of a musculoskeletal ultrasound examination. J. Ultrasound Med. 2012, 31, 1473–1488. [Google Scholar] [CrossRef]
- Lin, E.; Aligene, K.; Kirschner, J.S. Elbow. In Atlas of Ultrasound Guided Musculoskeletal Injections; Spinner, D.A., Kirschner, J.S., Herrera, J.E., Eds.; Springer: New York, NY, USA, 2014; pp. 17–28. [Google Scholar]
- Sigrist, R.M.S.; Liau, J.; Kaffas, A.E.; Chammas, M.C.; Willmann, J.K. Ultrasound Elastography: Review of Techniques and Clinical Applications. Theranostics 2017, 7, 1303–1329. [Google Scholar] [CrossRef] [PubMed]
- Bang, J.Y.; Hahn, S.; Yi, J.; Lim, Y.J.; Jung, H.K. Clinical applicability of shear wave elastography for the evaluation of medial epicondylitis. Eur. Radiol. 2021, 31, 6726–6735. [Google Scholar] [CrossRef] [PubMed]
- du Toit, C.; Stieler, M.; Saunders, R.; Bisset, L.; Vicenzino, B. Diagnostic accuracy of power Doppler ultrasound in patients with chronic tennis elbow. Br. J. Sports Med. 2009, 42, 872–876, Correction in Br. J. Sports Med. 2009, 43, 310–311. [Google Scholar] [CrossRef]
- Shin, M.; Hahn, S.; Yi, J.; Lim, Y.J.; Bang, J.Y. Clinical Application of Real-Time Sonoelastography for Evaluation of Medial Epicondylitis: A Pilot Study. Ultrasound Med. Biol. 2019, 45, 246–254. [Google Scholar] [CrossRef]
- Finlay, K.; Ferri, M.; Friedman, L. Ultrasound of the elbow. Skelet. Radiol. 2004, 33, 63–79. [Google Scholar] [CrossRef]
- Granger, A.; Sardi, J.P.; Iwanaga, J.; Wilson, T.J.; Yang, L.; Loukas, M.; Oskouian, R.J.; Tubbs, R.S. Osborne’s Ligament: A Review of its History, Anatomy, and Surgical Importance. Cureus 2017, 9, e1080. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.A.; Hannafin, J.A. Evaluation and management of elbow tendinopathy. Sports Health 2012, 4, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Cutts, S. Cubital tunnel syndrome. Postgrad. Med. J. 2007, 83, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Andrews, K.; Rowland, A.; Pranjal, A.; Ebraheim, N. Cubital tunnel syndrome: Anatomy, clinical presentation, and management. J. Orthop. 2018, 15, 832–836, Correction in J. Orthop. 2020, 23, 275. [Google Scholar] [CrossRef]
- Bordes, S.J.; Jenkins, S., Jr.; Bang, K.; Turgut, M.; Iwanaga, J.; Loukas, M.; Spinner, R.J.; Dumont, A.S.; Tubbs, R.S. Ulnar nerve subluxation and dislocation: A review of the literature. Neurosurg. Rev. 2021, 44, 793–798. [Google Scholar] [CrossRef]
- Tsukada, K.; Yasui, Y.; Sasahara, J.; Okawa, Y.; Nakagawa, T.; Kawano, H.; Miyamoto, W. Ulnar Nerve Dislocation and Subluxation from the Cubital Tunnel Are Common in College Athletes. J. Clin. Med. 2021, 10, 3131. [Google Scholar] [CrossRef]
- Rioux-Forker, D.; Bridgeman, J.; Brogan, D.M. Snapping Triceps Syndrome. J. Hand Surg. Am. 2018, 43, 90.e1–90.e5. [Google Scholar] [CrossRef]
- Shuttlewood, K.; Beazley, J.; Smith, C.D. Distal triceps injuries (including snapping triceps): A systematic review of the literature. World J. Orthop. 2017, 8, 507–513. [Google Scholar] [CrossRef]
- Chalmers, J. Unusual causes of peripheral nerve compression. Hand 1978, 10, 168–175. [Google Scholar] [CrossRef]
- Husarik, D.B.; Saupe, N.; Pfirrmann, C.W.; Jost, B.; Hodler, J.; Zanetti, M. Elbow nerves: MR findings in 60 asymptomatic subjects—normal anatomy, variants, and pitfalls. Radiology 2009, 252, 148–156. [Google Scholar] [CrossRef]
- Masear, V.R.; Hill, J.J., Jr.; Cohen, S.M. Ulnar compression neuropathy secondary to the anconeus epitrochlearis muscle. J. Hand Surg. Am. 1988, 13, 720–724. [Google Scholar] [CrossRef]
- Maslow, J.I.; Johnson, D.J.; Block, J.J.; Lee, D.H.; Desai, M.J. Prevalence and Clinical Manifestations of the Anconeus Epitrochlearis and Cubital Tunnel Syndrome. Hand 2020, 15, 69–74. [Google Scholar] [CrossRef]
- Freehill, M.T.; Safran, M.R. Diagnosis and management of ulnar collateral ligament injuries in throwers. Curr. Sports Med. Rep. 2011, 10, 271–278. [Google Scholar] [CrossRef]
- Zaremski, J.L.; Vincent, K.R.; Vincent, H.K. Elbow Ulnar Collateral Ligament: Injury, Treatment Options, and Recovery in Overhead Throwing Athletes. Curr. Sports Med. Rep. 2019, 18, 338–345. [Google Scholar] [CrossRef]
- Lee, A.T.; Lee-Robinson, A.L. The prevalence of medial epicondylitis among patients with c6 and c7 radiculopathy. Sports Health 2010, 2, 334–336. [Google Scholar] [CrossRef] [PubMed]
- Polston, D.W. Cervical radiculopathy. Neurol. Clin. 2007, 25, 373–385. [Google Scholar] [CrossRef] [PubMed]
- Vaishya, R.; Kapoor, C.; Agarwal, A.K.; Vijay, V. A Rare Presentation of Ganglion Cyst of the Elbow. Cureus 2016, 8, e665. [Google Scholar] [CrossRef]
- Chim, H.; Yam, A.K.; Teoh, L.C. Elbow ganglion arising from medial epicondyle pseudarthrosis. Hand Surg. 2007, 12, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Kuboi, T.; Tajika, T.; Endo, F.; Hatori, Y.; Saida, R.; Chikuda, H. Cubital tunnel syndrome with small occult ganglion: A case report of bike rider. SAGE Open Med. Case Rep. 2020, 8, 2050313X20972850. [Google Scholar] [CrossRef]
- Lee, S.W.; Kim, S.G.; Oh-Park, M. Ganglion cyst of radiocapitellar joint mimicking lateral epicondylitis: Role of ultrasonography. Am. J. Phys. Med. Rehabil. 2013, 92, 459–460. [Google Scholar] [CrossRef] [PubMed]
- Kokkalis, Z.T.; Schmidt, C.C.; Sotereanos, D.G. Elbow arthritis: Current concepts. J Hand Surg. Am. 2009, 34, 761–768. [Google Scholar] [CrossRef]
- Soojian, M.G.; Kwon, Y.W. Elbow arthritis. Bull NYU Hosp. Jt. Dis. 2007, 65, 61–71. [Google Scholar]
- Catalano, O.; Nunziata, A.; Saturnino, P.P.; Siani, A. Epitrochlear lymph nodes: Anatomy, clinical aspects, and sonography features. Pictorial essay. J. Ultrasound 2010, 13, 168–174. [Google Scholar] [CrossRef]
- Pannu, A.K.; Prakash, G.; Jandial, A.; Kopp, C.R.; Kumari, S. Epitrochlear lymphadenopathy. Korean J. Intern. Med. 2019, 34, 1396. [Google Scholar] [CrossRef]
- Selby, C.D.; Marcus, H.S.; Toghill, P.J. Enlarged epitrochlear lymph nodes: An old physical sign revisited. J. R. Coll. Physicians Lond. 1992, 26, 159–161. [Google Scholar]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konarski, W.; Poboży, T.; Kotela, A.; Hordowicz, M.; Poboży, K. Ultrasound in the Differential Diagnosis of Medial Epicondylalgia and Medial Elbow Pain—Imaging Findings and Narrative Literature Review. Healthcare 2022, 10, 1529. https://doi.org/10.3390/healthcare10081529
Konarski W, Poboży T, Kotela A, Hordowicz M, Poboży K. Ultrasound in the Differential Diagnosis of Medial Epicondylalgia and Medial Elbow Pain—Imaging Findings and Narrative Literature Review. Healthcare. 2022; 10(8):1529. https://doi.org/10.3390/healthcare10081529
Chicago/Turabian StyleKonarski, Wojciech, Tomasz Poboży, Andrzej Kotela, Martyna Hordowicz, and Kamil Poboży. 2022. "Ultrasound in the Differential Diagnosis of Medial Epicondylalgia and Medial Elbow Pain—Imaging Findings and Narrative Literature Review" Healthcare 10, no. 8: 1529. https://doi.org/10.3390/healthcare10081529