

Localization Strategy Prior to Radiofrequency Ablation for Primary and Secondary Hyperparathyroidism
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
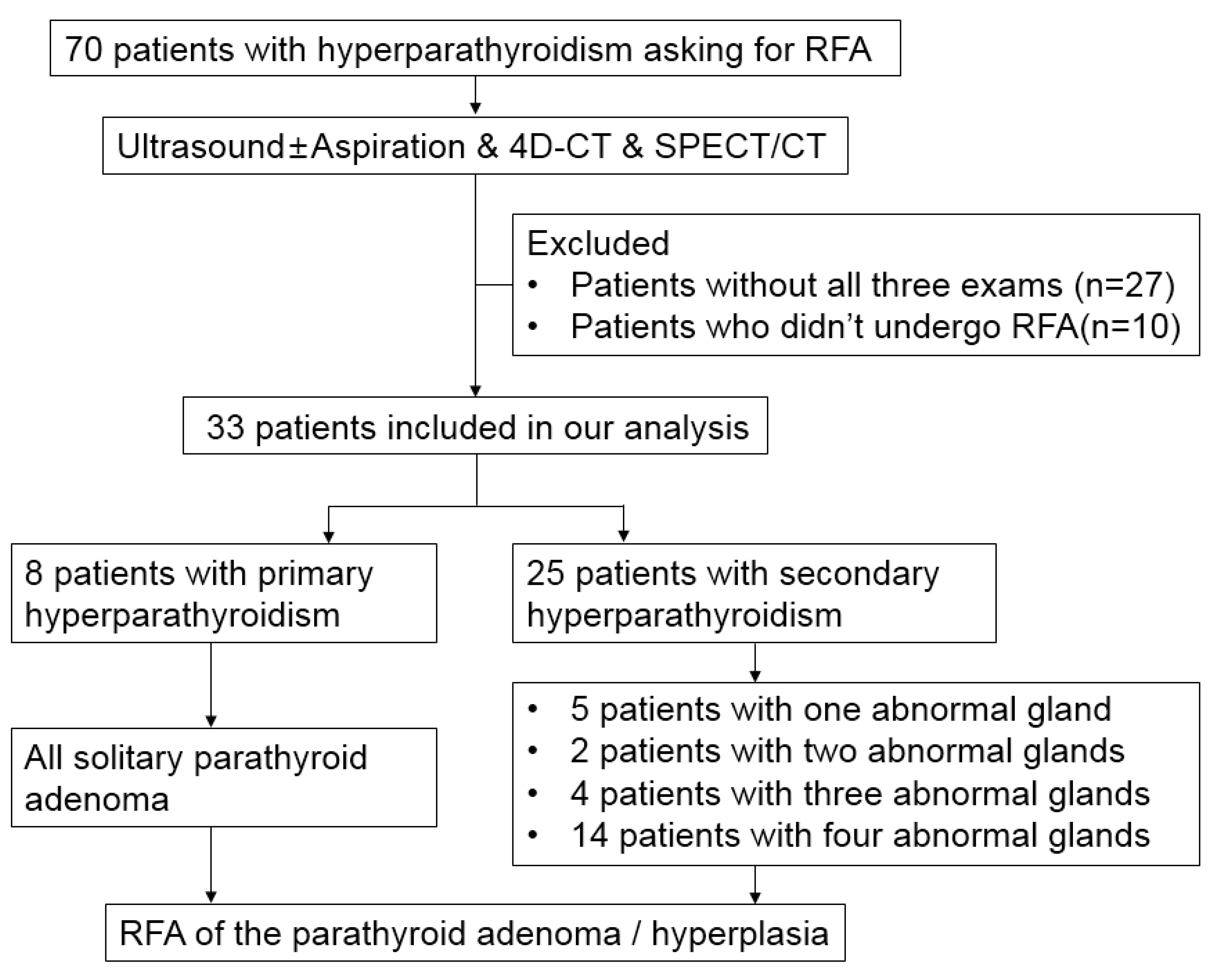
2.1. Patient Selection
2.2. Image Protocol
2.3. Image Interpretation
2.4. Radiofrequency Ablation Procedure and Data Collection
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of Patients
3.2. Characteristics of Positive Lesions
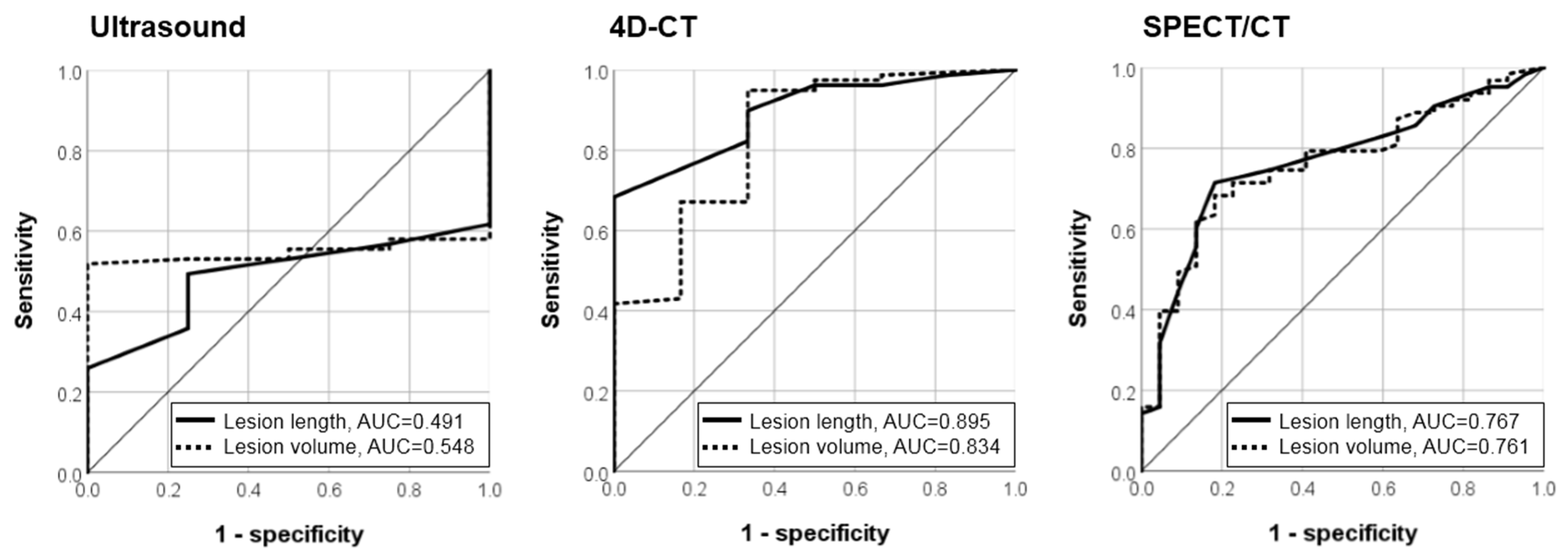
3.3. Diagnostic Accuracy of the Imaging Modalities
3.4. The Effect of Image Features on Different Imaging Modalities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 4D-CT | Four-dimensional computed tomography |
| ALK-P | Alkaline phosphatase |
| AUC | Area under curve |
| NPV | Negative predictive value |
| PHPT | Primary hyperparathyroidism |
| PPV | Positive predictive value |
| PTH | Parathyroid hormone |
| RFA | Radiofrequency ablation |
| ROC | Receiver operating characteristic |
| Sestamibi SPECT/CT | Technetium 99m–sestamibi single-photon-emission-computed tomography/computed tomography |
| SHPT | Secondary hyperparathyroidism |
| US | Ultrasound |
References
- Fraser, W.D. Hyperparathyroidism. Lancet 2009, 374, 145–158. [Google Scholar] [CrossRef]
- Bilezikian, J.P.; Bandeira, L.; Khan, A.; Cusano, N.E. Hyperparathyroidism. Lancet 2018, 391, 168–178. [Google Scholar] [CrossRef]
- Wilhelm, S.M.; Wang, T.S.; Ruan, D.T.; Lee, J.A.; Asa, S.; Duh, Q.-Y.; Doherty, G.M.; Herrera, M.F.; Pasieka, J.L.; Perrier, N.D.; et al. The American Association of Endocrine Surgeons Guidelines for Definitive Management of Primary Hyperparathyroidism. JAMA Surg. 2016, 151, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Hamdy, N.A. Parathyroid gland: Is parathyroidectomy safe and beneficial in the elderly? Nat. Rev. Endocrinol. 2009, 5, 422–423. [Google Scholar] [CrossRef] [PubMed]
- Ha, E.J.; Baek, J.H.; Baek, S.M. Minimally Invasive Treatment for Benign Parathyroid Lesions: Treatment Efficacy and Safety Based on Nodule Characteristics. Korean J. Radiol. 2020, 21, 1383–1392. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Cheng, L.; Zhang, W.; He, W. Ultrasound-guided thermal ablation for hyperparathyroidism: Current status and prospects. Int. J. Hyperth. 2022, 39, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Ebrahiminik, H.; Chegeni, H.; Khah, A.M.; Salouti, R.; Ghomashchi, G.; Pasikhani, M.D.; Heydari, I.; Shamsi, K.; Beiranvand, B.; Aval, M.R.A.; et al. Radiofrequency ablation of parathyroid adenomas causing primary hyperparathyroidism: A report of 27 patients. J. Clin. Ultrasound 2022, 50, 540–546. [Google Scholar] [CrossRef]
- Li, X.; Tufano, R.P.; Russell, J.O.; Yan, L.; Xiao, J.; Li, Y.; Zhang, M.; Luo, Y. Ultrasound-Guided Radiofrequency Ablation for the Treatment of Primary Hyperparathyroidism: An Efficacy and Safety Study. Endocr. Pract. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Peng, C.Z.; Chai, H.H.; Zhang, Z.X.; Hu, Q.H.; Zeng, Z.; Cui, A.L.; Pang, H.S.; Ruan, L.T. Radiofrequency ablation for primary hyperparathyroidism and risk factors for postablative eucalcemic parathyroid hormone elevation. Int. J. Hyperth. 2022, 39, 490–496. [Google Scholar] [CrossRef]
- Wei, Y.; Peng, C.Z.; Wang, S.R.; He, J.F.; Peng, L.L.; Zhao, Z.L.; Cao, X.J.; Li, Y.; Yu, M.A. Effectiveness and Safety of Thermal Ablation in the Treatment of Primary Hyperparathyroidism: A Multicenter Study. J. Clin. Endocrinol. Metab. 2021, 106, 2707–2717. [Google Scholar] [CrossRef]
- Ye, J.; Huang, W.; Huang, G.; Qiu, Y.; Peng, W.; Lan, N.; Xie, X.; Liu, B. Efficacy and safety of US-guided thermal ablation for primary hyperparathyroidism: A systematic review and meta-analysis. Int. J. Hyperth. 2020, 37, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Peng, C.-Z.; Liu, J.-B.; Li, Y.-W.; He, H.-F.; Hu, Q.-H.; Lin, B.; Shen, X.-G. Efficacy of Ultrasound-guided Radiofrequency Ablation of Parathyroid Hyperplasia: Single Session vs. Two-Session for Effect on Hypocalcemia. Sci. Rep. 2020, 10, 6206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qin, X.; Wang, B.; Li, B.; Lin, C.; Liu, X.; Xie, X. Value of contrast-enhanced ultrasonography in radiofrequency ablation of secondary hyperparathyroidism. Ren. Fail. 2021, 43, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.L.; Chen, S.; Gao, M.Z.; Lin, Y.C.; Hong, F.Y.; You, Z.H.; Chen, X.; Wu, S.S. Ultrasound-Guided Radiofrequency Ablation: A New Attempt to the Treatment of Refractory Hyperparathyroidism Secondary to Chronic Kidney Disease. Kidney Int. Rep. 2021, 7, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Zhang, Z.; Liu, J.; Chen, H.; Tu, X.; Hu, R.; Ni, J.; Weng, N.; Pang, H.; Xue, Z. Efficacy and safety of ultrasound-guided radiofrequency ablation of hyperplastic parathyroid gland for secondary hyperparathyroidism associated with chronic kidney disease. Head Neck 2017, 39, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Qian, L.; Zu, Y.; Wei, Y.; Hu, X. Efficacy of Ablation Therapy for Secondary Hyperparathyroidism by Ultrasound Guided Percutaneous Thermoablation. Ultrasound Med. Biol. 2016, 42, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.A.; Tublin, M.E.; Ogilvie, J.B. Parathyroid imaging: Technique and role in the preoperative evaluation of primary hyperparathyroidism. AJR Am. J. Roentgenol. 2007, 188, 1706–1715. [Google Scholar] [CrossRef]
- Tominaga, Y.; Tanaka, Y.; Sato, K.; Nagasaka, T.; Takagi, H. Histopathology, pathophysiology, and indications for surgical treatment of renal hyperparathyroidism. Semin. Surg. Oncol. 1997, 13, 78–86. [Google Scholar] [CrossRef]
- Wieneke, J.A.; Smith, A. Parathyroid adenoma. Head Neck Pathol. 2008, 2, 305–308. [Google Scholar] [CrossRef]
- Yeh, R.; Tay, Y.K.; Tabacco, G.; Dercle, L.; Kuo, J.H.; Bandeira, L.; McManus, C.; Leung, D.K.; Lee, J.A.; Bilezikian, J.P. Diagnostic Performance of 4D CT and Sestamibi SPECT/CT in Localizing Parathyroid Adenomas in Primary Hyperparathyroidism. Radiology 2019, 291, 469–476. [Google Scholar] [CrossRef]
- Ruda, J.M.; Hollenbeak, C.S.; Stack, B.C., Jr. A Systematic Review of the Diagnosis and Treatment of Primary Hyperparathyroidism from 1995 to 2003. Otolaryngol. Head Neck Surg. 2005, 132, 359–372. [Google Scholar] [CrossRef] [PubMed]
- Tay, D.; Das, J.P.; Yeh, R. Preoperative Localization for Primary Hyperparathyroidism: A Clinical Review. Biomedicines 2021, 9, 390. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.; Wang, T.S.; Farrokhyar, F.; Roman, S.A.; Sosa, J.A. A meta-analysis of preoperative localization techniques for patients with primary hyperparathyroidism. Ann. Surg. Oncol. 2012, 19, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Kunstman, J.W.; Kirsch, J.D.; Mahajan, A.; Udelsman, R. Clinical review: Parathyroid localization and implications for clinical management. J. Clin. Endocrinol. Metab. 2013, 98, 902–912. [Google Scholar] [CrossRef] [Green Version]
- Zhu, M.; He, Y.; Liu, T.; Tao, B.; Zhan, W.; Zhang, Y.; Xie, J.; Chen, X.; Zhao, H.; Sun, L.; et al. Factors That Affect the Sensitivity of Imaging Modalities in Primary Hyperparathyroidism. Int. J. Endocrinol. 2021, 2021, 3108395. [Google Scholar] [CrossRef]
- Wan, Q.C.; Li, J.F.; Tang, L.L.; Lv, J.; Xie, L.J.; Li, J.P.; Qin, L.P.; Cheng, M.H. Comparing the diagnostic accuracy of 4D CT and 99mTc-MIBI SPECT/CT for localizing hyperfunctioning parathyroid glands: A systematic review and meta-analysis. Nucl. Med. Commun. 2021, 42, 225–233. [Google Scholar] [CrossRef]
- Galvin, L.; Oldan, J.D.; Bahl, M.; Eastwood, J.D.; Sosa, J.A.; Hoang, J.K. Parathyroid 4D CT and Scintigraphy: What Factors Contribute to Missed Parathyroid Lesions? Otolaryngol. Head Neck Surg. 2016, 154, 847–853. [Google Scholar] [CrossRef]
- Kukar, M.; Platz, T.A.; Schaffner, T.J.; Elmarzouky, R.; Groman, A.; Kumar, S.; Abdelhalim, A.; Cance, W.G. The use of modified four-dimensional computed tomography in patients with primary hyperparathyroidism: An argument for the abandonment of routine sestamibi single-positron emission computed tomography (SPECT). Ann. Surg. Oncol. 2015, 22, 139–145. [Google Scholar] [CrossRef]
- Eichhorn-Wharry, L.I.; Carlin, A.M.; Talpos, G.B. Mild hypercalcemia: An indication to select 4-dimensional computed tomography scan for preoperative localization of parathyroid adenomas. Am. J. Surg. 2011, 201, 334–338; discussion 338. [Google Scholar] [CrossRef]
- Kuzminski, S.J.; Sosa, J.A.; Hoang, J.K. Update in Parathyroid Imaging. Magn. Reson. Imaging Clin. N. Am. 2018, 26, 151–166. [Google Scholar] [CrossRef]
- Chen, C.C.; Chen, H.L.; Chiang, P.L.; Luo, S.D.; Chang, Y.H.; Chen, W.C.; Wang, C.K.; Lin, A.N.; Chen, Y.S.; Chi, S.Y.; et al. Efficacy and safety of radiofrequency ablation for primary and secondary hyperparathyroidism with or without previous parathyroidectomy: A retrospective study. Int. J. Hyperth. 2022, 39, 907–917. [Google Scholar] [CrossRef]
- Hanley, J.A.; McNeil, B.J. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 1983, 148, 839–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rickes, S.; Sitzy, J.; Neye, H.; Ocran, K.W.; Wermke, W. High-resolution ultrasound in combination with colour-Doppler sonography for preoperative localization of parathyroid adenomas in patients with primary hyperparathyroidism. Ultraschall Med. 2003, 24, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Day, K.M.; Elsayed, M.; Beland, M.D.; Monchik, J.M. The utility of 4-dimensional computed tomography for preoperative localization of primary hyperparathyroidism in patients not localized by sestamibi or ultrasonography. Surgery 2015, 157, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Cunha-Bezerra, P.; Vieira, R.; Amaral, F.; Cartaxo, H.; Lima, T.; Montarroyos, U.; Bandeira, F. Better performance of four-dimension computed tomography as a localization procedure in normocalcemic primary hyperparathyroidism. J. Med. Imaging Radiat. Oncol. 2018, 62, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Kelly, H.R.; Hamberg, L.M.; Hunter, G.J. 4D-CT for preoperative localization of abnormal parathyroid glands in patients with hyperparathyroidism: Accuracy and ability to stratify patients by unilateral versus bilateral disease in surgery-naive and re-exploration patients. AJNR Am. J. Neuroradiol. 2014, 35, 176–181. [Google Scholar] [CrossRef] [Green Version]
- Mahajan, A.; Starker, L.F.; Ghita, M.; Udelsman, R.; Brink, J.A.; Carling, T. Parathyroid four-dimensional computed tomography: Evaluation of radiation dose exposure during preoperative localization of parathyroid tumors in primary hyperparathyroidism. World J. Surg. 2012, 36, 1335–1339. [Google Scholar] [CrossRef]
- Hung, C.L.; Hsu, Y.C.; Huang, S.M.; Hung, C.J. Application of Tissue Aspirate Parathyroid Hormone Assay for Imaging Suspicious Neck Lesions in Patients with Complicated Recurrent or Persistent Renal Hyperparathyroidism. J. Clin. Med. 2021, 10, 329. [Google Scholar] [CrossRef]
- Abdelghani, R.; Noureldine, S.; Abbas, A.; Moroz, K.; Kandil, E. The diagnostic value of parathyroid hormone washout after fine-needle aspiration of suspicious cervical lesions in patients with hyperparathyroidism. Laryngoscope 2013, 123, 1310–1313. [Google Scholar] [CrossRef] [PubMed]
- Stephen, A.E.; Milas, M.; Garner, C.N.; Wagner, K.E.; Siperstein, A.E. Use of surgeon-performed office ultrasound and parathyroid fine needle aspiration for complex parathyroid localization. Surgery 2005, 138, 1143–1150; discussion 1150–1151. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, M.P.; Fraker, D.L.; Shawker, T.H.; A Norton, J.; Doppman, J.L.; A Chang, R.; Skarulis, M.C.; Marx, S.J.; Spiegel, A.M.; Alexander, H.R. Use of preoperative fine-needle aspiration in patients undergoing reoperation for primary hyperparathyroidism. Surgery 1994, 116, 959–964; discussion 964–965. [Google Scholar]
- Kendrick, M.L.; Charboneau, J.W.; Curlee, K.J.; van Heerden, J.A.; Farley, D.R. Risk of parathyromatosis after fine-needle aspiration. Am. Surg. 2001, 67, 290–293; discussion 293–294. [Google Scholar] [CrossRef] [PubMed]
- Cotoi, L.; Amzar, D.; Sporea, I.; Borlea, A.; Navolan, D.; Varcus, F.; Stoian, D. Shear Wave Elastography versus Strain Elastography in Diagnosing Parathyroid Adenomas. Int. J. Endocrinol. 2020, 2020, 3801902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotoi, L.; Borcan, F.; Sporea, I.; Amzar, D.; Schiller, O.; Schiller, A.; Dehelean, C.A.; Pop, G.N.; Stoian, D. Shear wave elastography in diagnosing secondary hyperparathyroidism. Diagnostics 2019, 9, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, R.; Gao, L.; Shi, X.; Ma, L.; Wang, O.; Xia, W.; Hu, Y.; Xia, Y.; Jiang, Y. Shear wave elastography for differentiating parathyroid neoplasms with malignant diagnosis or uncertain malignant potential from parathyroid adenomas: Initial experience. Cancer Imaging 2022, 22, 1–10. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primary Hyperparathyroidism (n = 8) | Secondary Hyperparathyroidism (n = 25) | All (n = 33) | |||
|---|---|---|---|---|---|
| Age (year) | 52.5 (47.75–61.25) | 63 (49–68) | 61 (49–67) | ||
| Gender (Male) | 3 (37.5%) | 11 (44.0%) | 14 (42.4%) | ||
| Serum biochemistry before RFA | |||||
| I-PTH (pg/mL) | 177.0 (145.9–232.1) | 1356.9 (1038.3–1979.8) | 1259.3 (643.5–1829.3) | ||
| Calcium (mg/dL) | 11.4 (11.3–11.6) | 10.4 (9.7–11.0) | 10.6 (9.9–11.3) | ||
| Phosphorus (mg/dL) | 2.6 (2.4–3.1) | 5.3 (4.0–6.1) | 4.7 (3.3–6.1) | ||
| ALK-P (U/L) | 90.5 (86.0–175.3) | 135.5 (88.0–210.75) | 115.5(86.0–195.0) | ||
| Patient-based analysis (number of patients) | |||||
| Previous parathyroidectomy | No (n = 8) (100%) | Yes (n = 0) (0.0%) | No (n = 19) (76.0%) | Yes (n = 6) (24.0%) | |
| One gland | 8 (100%) | 0 (0.0%) | 0 (0.0%) | 5 (83.3%) | 13 (39.4%) |
| Two glands | 0 (0.0%) | 0 (0.0%) | 2 (10.5%) | 0 (0.0%) | 2 (6.1%) |
| Three glands | 0 (0.0%) | 0 (0.0%) | 3 (15.8%) | 1 (16.7%) | 4 (12.1%) |
| Four glands | 0 (0.0%) | 0 (0.0%) | 14 (73.7%) | 0 (0.0%) | 14 (42.4%) |
| Primary Hyperparathyroidism (n = 9) | Secondary Hyperparathyroidism (n = 79) | Total (n = 88) | |
|---|---|---|---|
| Concordant location in three modalities | 5 (55.6%) | 56 (70.9%) | 61 (69.3%) |
| Concordant location in two modalities | 3 (33.3%) | 13 (16.5%) | 16 (18.2%) |
| Only seen in ultrasound * | 0 (0.0%) | 6 (7.6%) | 6 (6.8%) |
| Only seen in 4D-CT | 0 (0.0%) | 2 (2.5%) | 2 (2.3%) |
| Not parathyroid gland | 1 (thyroid Hurthle cell neoplasm) (11.1%) | 2 (thyroid nodule and lymph node) (2.5%) | 3 (3.4%) |
| Total number of parathyroid adenoma/hyperplasia (n= 85) | |||
| Right superior | 0 (0.00%) | 16 (20.8%) | 16 (18.8%) |
| Right inferior | 4 (50.0%) | 23 (29.9%) | 27 (31.8%) |
| Left superior | 3 (37.5%) | 17 (22.1%) | 20 (23.5%) |
| Left inferior | 1 (12.5%) | 21 (27.3%) | 22 (25.9%) |
| % | US | 4D-CT | SPECT | US + 4D-CT | US + SPECT | 4D-CT + SPECT | All |
|---|---|---|---|---|---|---|---|
| Sensitivity | 0.953 (81/85) | 0.929 (79/85) | 0.741 (63/85) | 1.000 (85/85) | 0.976 (83/85) | 0.929 (79/85) | 1.000 (85/85) |
| Specificity | 0.667 (2/3) | 0.667 (2/3) | 0.000 (0/3) | 0.667 (2/3) | 0.667 (2/3) | 0.667 (2/3) | 0.667 (2/3) |
| PPV | 0.988 (81/82) | 0.988 (79/80) | 0.955 (63/66) | 0.988 (85/86) | 0.988 (83/84) | 0.988 (79/80) | 0.988 (85/86) |
| NPV | 0.333 (2/6) | 0.250 (2/8) | 0.000 (0/22) | 1.000 (2/2) | 0.500 (2/4) | 0.250 (2/8) | 1.000 (2/2) |
| Accuracy | 0.943 (83/88) | 0.920 (81/88) | 0.716 (63/88) | 0.989 (87/88) | 0.966 (85/88) | 0.920 (81/88) | 0.989 (87/88) |
| % | US | 4D-CT | SPECT | US + 4D-CT | US + SPECT | 4D-CT + SPECT | All |
|---|---|---|---|---|---|---|---|
| Primary hyperparathyroidism (n = 9) | |||||||
| Sensitivity | 1.000 (8/8) | 1.000 (8/8) | 0.625 (5/8) | 1.000 (8/8) | 1.000 (8/8) | 1.000 (8/8) | 1.000 (8/8) |
| Specificity | 0.000 (0/1) | 0.000 (0/1) | 0.000 (0/1) | 0.000 (0/1) | 0.000 (0/1) | 0.000 (0/1) | 0.000 (0/1) |
| PPV | 0.889 (8/9) | 0.889 (8/9) | 0.833 (5/6) | 0.889 (8/9) | 0.889 (8/9) | 0.889 (8/9) | 0.889 (8/9) |
| NPV | 0.000 (0/0) | 0.000 (0/0) | 0.000 (0/3) | 0.000 (0/0) | 0.000 (0/0) | 0.000 (0/0) | 0.000 (0/0) |
| Accuracy | 0.889 (8/9) | 0.889 (8/9) | 0.556 (5/9) | 0.889 (8/9) | 0.889 (8/9) | 0.889 (8/9) | 0.889 (8/9) |
| Secondary hyperparathyroidism (n = 79) | |||||||
| Sensitivity | 0.948 (73/77) | 0.922 (71/77) | 0.753 (58/77) | 1.000 (77/77) | 0.974 (75/77) | 0.922 (71/77) | 1.000 (77/77) |
| Specificity | 1.000 (2/2) | 1.000 (2/2) | 0.000 (0/2) | 1.000 (2/2) | 1.000 (2/2) | 1.000 (2/2) | 1.000 (2/2) |
| PPV | 1.000 (73/73) | 1.000 (71/71) | 0.967 (58/60) | 1.000 (77/77) | 1.000 (75/75) | 1.000 (71/71) | 1.000 (77/77) |
| NPV | 0.333 (2/6) | 0.250 (2/8) | 0.000 (0/19) | 1.000 (2/2) | 0.500 (2/4) | 0.250 (2/6) | 1.000 (2/2) |
| Accuracy | 0.949 (75/79) | 0.924 (73/79) | 0.734 (58/79) | 1.000 (79/79) | 0.975 (77/79) | 0.924 (73/79) | 1.000 (79/79) |
| All Patients | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| US(+) (n = 81) | US(-) (n = 4) | p | 4D-CT(+) (n = 79) | 4D-CT(-) (n = 6) | p | SPECT(+) (n = 63) | SPECT(-) (n = 22) | p | |||
| Lesion location (n) | RS | 14 | 2 | 0.165 | 13 | 3 | 0.077 | 9 | 7 | 0.343 | |
| RI | 25 | 2 | 27 | 0 | 21 | 6 | |||||
| LS | 20 | 0 | 18 | 2 | 15 | 5 | |||||
| LI | 22 | 0 | 21 | 1 | 18 | 4 | |||||
| Lesion length (cm) | 1.30 (1.10–1.75) | 1.30 (1.23–1.53) | 0.960 | 1.40 (1.10–1.80) | 0.78 (0.68–1.10) | 0.01 * | 1.50 (1.10–2.00) | 1.10 (0.80–1.20) | <0.001 * | ||
| Lesion volume (cm3) | 0.48 (0.21–1.04) | 0.41 (0.37–0.43) | 0.756 | 0.48 (0.24–1.08) | 0.09 (0.05–0.39) | 0.07 * | 0.55 (0.31–1.40) | 0.25 (0.14–0.37) | <0.001 * | ||
| Secondary Hyperparathyroidism | |||||||||||
| US(+) (n = 73) | US(-) (n = 4) | p | 4D-CT(+) (n = 71) | 4D-CT(-) (n = 6) | p | SPECT(+) (n = 58) | SPECT(-) (n = 22) | p | |||
| Location (n) | RS | 14 | 2 | 0.219 | 13 | 3 | 0.095 | 9 | 7 | 0.289 | |
| RI | 21 | 2 | 23 | 0 | 20 | 3 | |||||
| LS | 17 | 0 | 15 | 2 | 12 | 5 | |||||
| LI | 21 | 0 | 20 | 1 | 17 | 4 | |||||
| Lesion length (cm) | 1.30 (1.10–1.65) | 1.30 (1.23–1.53) | 0.886 | 1.40 (1.10–1.70) | 0.78 (0.68–1.10) | 0.001 * | 1.50 (1.10–1.83) | 1.10 (0.80–1.20) | <0.001 * | ||
| Lesion volume (cm3) | 0.48 (0.21–1.04) | 0.41 (0.37–0.43) | 0.799 | 0.48 (0.24–1.08) | 0.09 (0.05–0.39) | 0.008 * | 0.53 (0.30–1.23) | 0.24 (0.13–0.36) | 0.001 * | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-Y.; Chang, Y.-H.; Chiang, P.-L.; Wang, C.-K.; Lin, A.-N.; Chen, C.-C.; Chen, Y.-F.; Chi, S.-Y.; Chou, F.-F.; Lin, W.-C. Localization Strategy Prior to Radiofrequency Ablation for Primary and Secondary Hyperparathyroidism. Biomedicines 2023, 11, 672. https://doi.org/10.3390/biomedicines11030672
Lee C-Y, Chang Y-H, Chiang P-L, Wang C-K, Lin A-N, Chen C-C, Chen Y-F, Chi S-Y, Chou F-F, Lin W-C. Localization Strategy Prior to Radiofrequency Ablation for Primary and Secondary Hyperparathyroidism. Biomedicines. 2023; 11(3):672. https://doi.org/10.3390/biomedicines11030672
Chicago/Turabian StyleLee, Chih-Ying, Yen-Hsiang Chang, Pi-Ling Chiang, Cheng-Kang Wang, An-Ni Lin, Chi-Cheng Chen, Yi-Fan Chen, Shun-Yu Chi, Fong-Fu Chou, and Wei-Che Lin. 2023. "Localization Strategy Prior to Radiofrequency Ablation for Primary and Secondary Hyperparathyroidism" Biomedicines 11, no. 3: 672. https://doi.org/10.3390/biomedicines11030672