
Combined Pulmonary Fibrosis and Emphysema: Comparative Evidence on a Complex Condition




1
Department of Pulmonology and Allergology, State University of Medicine and Pharmacy “Nicolae Testemitanu”, MD-2004 Chisinau, Moldova
2
Division of Immunology, Immunity to Infection and Respiratory Medicine, School of Biological Sciences, The University of Manchester, Manchester M13 9PL, UK
3
Department of Pulmonology, Semmelweis University, 1083 Budapest, Hungary
*
Author to whom correspondence should be addressed.
Biomedicines 2023, 11(6), 1636; https://doi.org/10.3390/biomedicines11061636
Submission received: 28 April 2023
/
Revised: 31 May 2023
/
Accepted: 2 June 2023
/
Published: 4 June 2023
(This article belongs to the Special Issue COPD Phenotypes and Treatable Traits: From Bench to Bedside)
Abstract
:Combined pulmonary fibrosis and emphysema (CPFE) is a clinical syndrome characterized by upper lobe emphysema and lower lobe fibrosis manifested by exercise hypoxemia, normal lung volumes, and severe reduction of diffusion capacity of carbon monoxide. It has varying prevalence worldwide with a male predominance, and with smoking history of more than 40 pack-years being a common risk factor. The unique imaging features of CPFE emphasize its distinct entity, aiding in the timely detection of pulmonary hypertension and lung cancer, both of which are common complications. High-resolution computed tomography (HRCT) is an important diagnostic and prognostic tool, while lung cancer is an independent factor that alters the prognosis in CPFE patients. Treatment options for CPFE are limited, but smoking cessation, usual treatments of pulmonary fibrosis and emphysema, and avoidance of environmental exposures are encouraged.
1. Introduction
Chronic obstructive pulmonary disease (COPD) and idiopathic pulmonary fibrosis (IPF) have long been considered mutually exclusive disorders. However, in recent years, the coexistence of emphysema and pulmonary fibrosis has emerged as a new entity. Historically, these two diseases found concomitantly in the same patient were first described almost half a century ago [1], and it was only in 2005 that Cottin and colleagues proposed the term “combined pulmonary fibrosis and emphysema” (CPFE) as the name of a well-defined condition characterized by upper lobe emphysema and lower lobe pulmonary fibrosis [2], to mark a specific consequence of smoking in susceptible patients. CPFE is considered to have distinct pathophysiological, clinical, radiological, functional, and prognostic features compared to its separate components.
In light of the increased interest in this new entity over the past few years, this article will present a comprehensive overview of the specific features of CPFE and comparative evidence describing COPD and IPF.
2. Definition
CPFE is a clinical syndrome that affects heavy smokers and is characterized by a combination of upper lobe emphysema and lower lobe fibrosis. Symptoms of CPFE include exercise-induced and later resting hypoxemia, normal lung volumes, and a significant reduction in the diffusing capacity, frequently associated with pulmonary hypertension. It is a heterogeneous condition affecting a diverse population of individuals.
3. Epidemiology
COPD prevalence estimates vary across the world in the general population, ranging from 1382.6 cases per 100,000 in Latin America and 1821.5 cases per 100,000 in Eastern Europe to 3017.5 cases per 100,000 in Western Europe and 3558.4 cases per 100,000 in North America [3]. In contrast, idiopathic pulmonary fibrosis (IPF) has a lower prevalence, ranging from 0.33 to 2.51 cases per 10,000 people in Europe, 2.40 to 2.98 in North America, and 0.57 to 4.51 in Asia-Pacific countries [4]. CPFE is estimated to occur in 8–67% of IPF patients, with variations in prevalence depending on the population studied, genetic susceptibility, smoking rates, or CPFE definitions [2,5,6]. Conversely, lung fibrosis was found to occur in 8% of emphysema patients based on HRCT scans [7].
Patients with CPFE are generally older with a heavy smoking history. The majority of studies have shown that almost all CPFE patients have a significant smoking history, suggesting that smoking may be the predominant risk factor for this condition [8,9]. The smoking history does not differ considerably between CPFE and COPD [10], although IPF patients often have fewer pack-years than those with CPFE or COPD [11].
Numerous studies have found a male predominance in CPFE syndrome [12], but more recent data [8] indicate a significant female incidence. Although it has been shown that male smokers are more likely than female smokers to develop emphysema and IPF [13], this does not necessarily mean that gender is a separate risk factor for CPFE. To fully understand the gender variations in this disease, more research is required.
After the sixth decade of life, CPFE seems to affect males more frequently [14]. Patients typically have a smoking history of more than 40 pack-years and are either current or former smokers [15]. However, studies showing CPFE in non-smokers with connective tissue disease have demonstrated a genetic predisposition to the disease [16].
4. Etiology and Pathogenesis
The exact mechanisms leading to the development of both emphysema and fibrotic lesions are not fully understood. Whether the coexistence of two different entities is just a “cohabitation” or if there is a result of shared mechanisms that led to the creation of both is still up for debate. However, the pathogenesis of CPFE is multifactorial, occurring in susceptible individuals after exposure to environmental triggers such as smoking or dust inhalation.
Emphysema and pulmonary fibrosis are both recognized as primarily driven by smoking [17], and most CPFE patients appear to be either current or former smokers [15]. The correlation between CPFE and pack years supports a dose–response relationship [18,19].
Environmental exposures such as noxious particles or gases other than tobacco, asbestos, silica dust, and agrochemical chemicals [20] may contribute to lung damage in CPFE syndrome patients, even in lifelong nonsmokers. Moreover, case-based reports link welding jobs or the tire manufacturing industry to CPFE [21,22]. Interestingly, CPFE can be found in up to 23% of patients with fibrotic hypersensitivity pneumonitis (fHP) [23].
Since nonsmokers also develop CPFE, which is especially true in connective tissue diseases (CTDs) [24,25,26], the condition itself could be considered a risk factor. Radiological findings of CPFE have been documented in systemic sclerosis-associated ILD [25], rheumatoid arthritis-associated ILD [24], systemic vasculitis-associated ILD, and particularly microscopic polyangiitis [26]. Regarding autoimmunity as a potential contributing background, compared to IPF patients, individuals with CPFE were likelier to have high serum antinuclear antibodies, with or without positive perinuclear antineutrophil cytoplasmic antibodies (p-ANCA), and also a better prognosis [27]. The better outcomes in patients with CTD-associated CPFE compared to those with idiopathic CPFE could be linked to an increased infiltration of CD20+ B lymphocytes generating lymphoid follicles in fibrotic lung tissue [27].
Another potential risk factor for the development of both entities is oxidative stress [28,29]. In the case of emphysema, numerous hazardous substances found in cigarette smoke alter bronchoalveolar macrophages, producing an excess of reactive oxygen species (ROS) and nitrogen species (RNS). This results in the production of pro-inflammatory cytokines and the recruitment of inflammatory cells, which generate ROS and increases the oxidative stress burden, impairing the balance of proteases and antiproteases, leading to DNA damage and causing cellular injury and death and decrease in extracellular matrix proteases [29,30]. However, in the case of pulmonary fibrosis, the same oxidizing agents (cigarette smoke, hyperoxia, asbestos, drugs and radiation) induce the production of ROS/RNS, stimulate the production of pro-fibrotic factors—transforming growth factor β (TGF-β)—that activate fibroblasts and their differentiation into myofibroblasts, as well as extracellular matrix deposition [31].
In addition, accelerated lung aging has been suggested as a potential mechanism for the onset of pulmonary fibrosis and pulmonary emphysema [17,32], and both disorders have been linked to senescence markers and mutations in genes associated with lung surfactant [33]. Telomere-shortening mutations in genes encoding telomerase are risk factors for pulmonary fibrosis in up to 20% of familial cases [34]. Similarly, short telomeres can lower the threshold of smoking-induced damage and constitute a genetic susceptibility factor for emphysema.
It is reasonable to assume that the lung parenchyma depicts distinct patterns of injury and repair, displaying various phenotypes of lesions determined by the balance between apoptosis, proteolysis, and fibrosis. Patients with overexpression of genes related to connective tissue synthesis, structural components of the cytoskeleton, and cell adhesion typically exhibit a fibrogenic phenotype similar to that observed in patients with IPF; however, a different inflammatory response to smoking-associated cellular damage (destruction and repair of cells, vessels, and pneumocytes) results in the destruction of the lung parenchyma, leading to pulmonary emphysema [35]. Gene expression analysis of fibrotic and emphysematous lesions in patients with CPFE has demonstrated the presence of a combination of fibrogenic and emphysematous patterns, reflecting ongoing damage to alveolar epithelial cells, attempts at alveolar regeneration, uncontrolled fibrosis proliferation, and parenchymal destruction, resulting in a vicious cycle of continuous injury and fibrosis [36].
Studies suggest that the development of CPFE results from the interaction between environmental exposure, such as smoking, and genetic predisposition in susceptible individuals. COPD and IPF share genetic variants in the MMP9, MUC5B, FAM13A, DSP, and TERT genes [37,38]. Since each disease has a unique pathophysiological profile, it is unknown whether the interaction between COPD and IPF can lead to the development of CPFE. Intriguingly, findings suggest that COPD, IPF, and CPFE syndrome each have a distinct genomic profile. Moreover, studies found that the same allele may have opposite roles in these two conditions. For example, a FAM13A allele was associated with an increased risk of IPF and a decreased risk of COPD [39]. Others report an association between either COPD or IPF with an increased risk of CPFE. A study performed in a Japanese cohort reported that the minor allele of the AGER gene rs2070600 was associated with CPFE among COPD patients [40]. Earlier, it was found that the T allele of MMP9 may be a risk factor for developing emphysema in patients with IPF in the Chinese population [41]. Moreover, the rs2736100 C allele of TERT was associated with a decreased IPF risk and an increased risk for CPFE in a Mexican cohort. Additionally, the rs2076295 TT genotype of DSP was associated with an increased IPF risk, while the GG genotype with CPFE susceptibility [42]. In a recent study, Ghosh, A.J. and colleagues showed divergent gene expression profiles in COPD and IPF, emphasizing opposing inflammatory and immune-related pathways in the pathogenesis of both diseases. Nonetheless, the overexpression of this gene signature in the blood was associated with decreased lung function in both diseases, indicating the presence of a common inflammatory subtype associated with a more severe disease course [43].
Despite sharing age-related alterations, mitochondrial dysfunction, excessive oxidative stress, resulting in pathological tissue repair, the prevalence, pathology, and clinical behavior of IPF and COPD are notably distinct. This is likely due to substantial disparities in genetic background and epigenetic modifications between the two diseases, which result in distinct target cell types and molecular responses to environmental triggers. As such, the mechanisms that contribute to the age-related preference for IPF and COPD, or the combination, currently remain unknown [44].
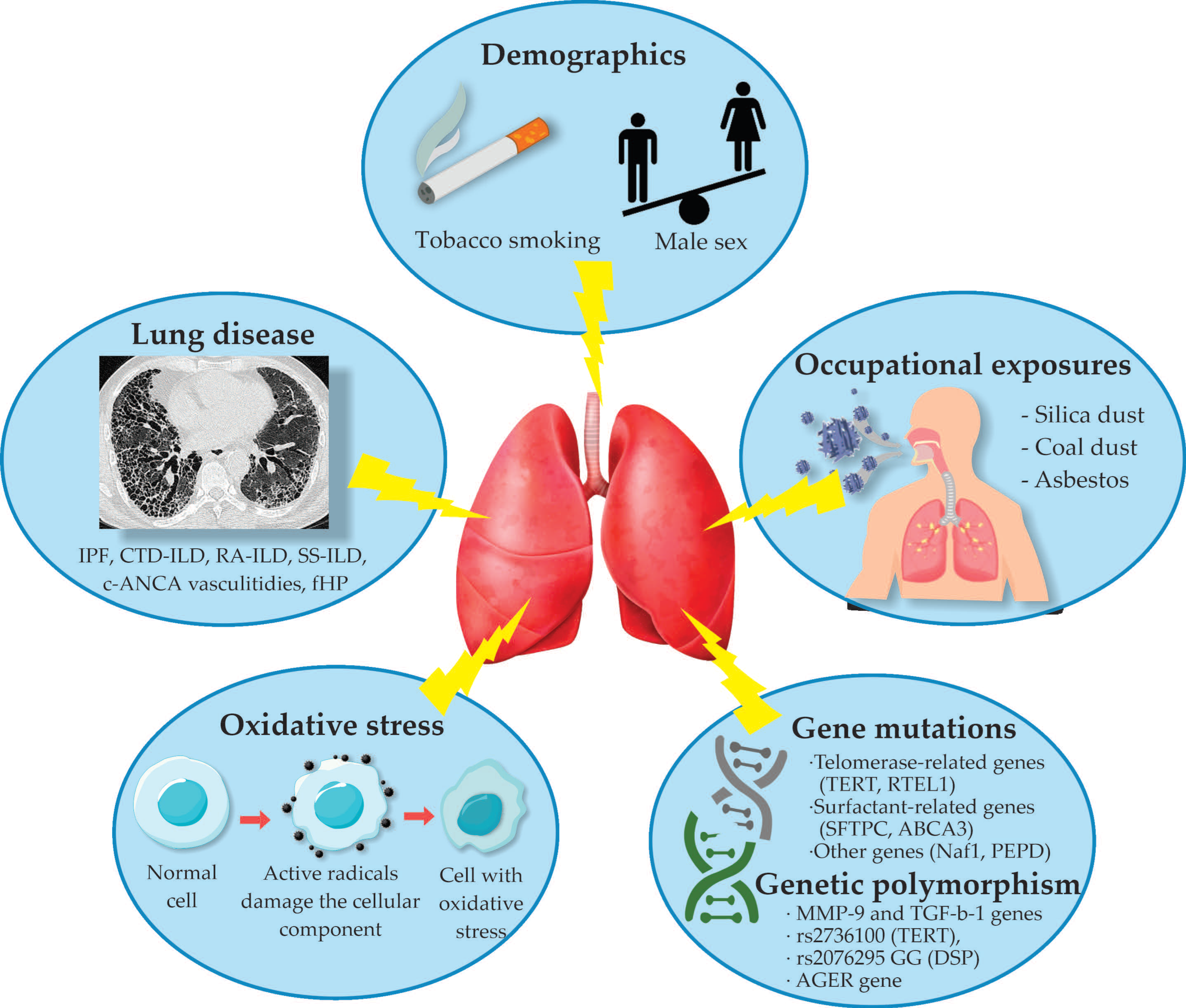
A summary of the factors associated with CPFE is represented in Figure 1.
5. Main Pathological Features
COPD and IPF share common features at both the micro- and macroscopic levels, demonstrating patchy distribution of pathological areas, consisting of extracellular matrix proteins or inflammatory infiltrates with fibrotic regions alternating with regions of normal alveolar tissue or areas with interstitial leukocyte accumulation [45]. The distinction between the two entities consists mainly in the affected compartments of the lung, small airway remodeling, fibrosis, and destruction of the lung parenchyma with an upper lobe predominance in COPD while IPF exclusively affects the lung parenchyma and interstitium, having a lower lobe predilection [46]. Lung alterations found in CPFE most commonly combine emphysema and patchy fibrosis, fibroblast foci, and honeycombing comprising the usual interstitial pneumonia (UIP) pattern. A hallmark of CPFE is the presence of thick-walled cysts on a UIP background, which is a combination of emphysema and smoking-related interstitial fibrosis (SRIF). Alternatively, it may associate the nonspecific interstitial pneumonitis (NSIP) or the desquamative interstitial pneumonitis (DIP) patterns [6].
6. Clinical Features
Compared to IPF and COPD, patients with CPFE typically have a mean age of 65–70 years, and males predominantly account for 73–100% of cases [6].
Cough and dyspnea are frequent symptoms in CPFE, COPD, and IPF. Typically, chronic cough and sputum production, as a hallmark of COPD, occur many years before airflow limitation [47]. In contrast, patients with IPF experience dyspnea in over 90% of cases at the time of diagnosis [48], followed by a dry cough in 80% of patients in the late stage [49]. The symptoms of CPFE resemble those of IPF more closely.
In almost all patients, progressive shortness of breath is the most common symptom and is typically more severe, especially during physical exertion. Exertional dyspnea is the clinical expression of inefficient ventilation and increased dead space ventilation in hypoperfused areas [50].
Other common respiratory signs and symptoms, such as cough, wheezing, cyanosis, and fatigue, may also manifest in some patients.
On physical examination, patients with CPFE typically have inspiratory crackles referred to as “velcro sounds” produced by the underlying pulmonary fibrosis, found in 87–100% of patients, and almost half of them have finger clubbing [15]. In addition, pulmonary hypertension (PH) imposes a New York Heart Association functional class of III or IV during physical exertion [51] and may contribute to peripheral edema and hepatosplenomegaly. Lung cancer and PH are the two most prevalent comorbidities in CPFE [52,53].
7. Lung Function
CPFE is distinguished from pure emphysema and IPF in terms of pulmonary function by the unexpected presence of relatively normal lung volumes in contrast to a severely diminished diffusing capacity (DLCO), as presented in Table 1 [9]. The preserved lung volumes can be attributed to the counterbalancing effects of emphysema’s hyperinflation defect and pulmonary fibrosis’ restrictive defect. Thus, Cottin et al. concluded that serial FVC measurement may not be suitable for monitoring the progression of IPF in patients with an emphysema extent of 15% [5]. At the same time, the diminished diffusing capacity may be attributable to the overlapping negative effects of both decreased capillary blood volume in emphysema and alveolar membrane thickening from pulmonary fibrosis, resulting in more significant reductions in DLCO [10]. Thus, if only spirometry is performed, the relative preservation of spirometric values may lead to an underdiagnosis of chronic lung disease.
The blood gas analysis of CPFE differs from that of COPD and resembles that of IPF more closely. Severe decreases in arterial oxygen saturation and hypoxemia during exercise are highly prevalent in CPFE, particularly when complicated by severe PH [51,54]. Therefore, exercise limitation accompanied by a decrease in oxygen saturation and an isolated and/or severe decrease in DLCO or KCO, in contrast to a mild ventilatory defect, should raise the suspicion of CPFE and/or PH. Hypercapnia occurs very late in the progression of the disease. The functional profile is similar when CPFE is present in CTD or fHP [16,24].
8. Imaging
Imaging demonstrates a variety of findings on chest high-resolution computed tomography (HRCT) dominated by the coexistence of emphysema in the upper zones of the lungs and pulmonary fibrosis in the lower zones [2]. The fibrotic lesions are heterogeneous and commonly represented by the UIP pattern with honeycomb images in 95% of cases, subpleural reticular opacities in 87%, and traction bronchiectasis in 73% of cases [2]. Emphysematous lesions in patients with CPFE include diffuse (centrilobular and/or bullous) emphysema (Figure 2) or paraseptal emphysema with subpleural predominance [2]. In an earlier publication, Cottin et al. suggested that CPFE patients typically have predominantly paraseptal emphysema, which is considered a distinctive feature of this syndrome, compared to the typical centrilobular smoking-related emphysema seen in COPD. However, there are currently no studies that have directly compared patterns of emphysema in CPFE and COPD [49]. The areas of fibrosis and emphysema may be completely separated, or they may transition gradually. Moreover, paraseptal emphysematous lesions may exist at the lung bases within the fibrotic lesions (Figure 3) [55].
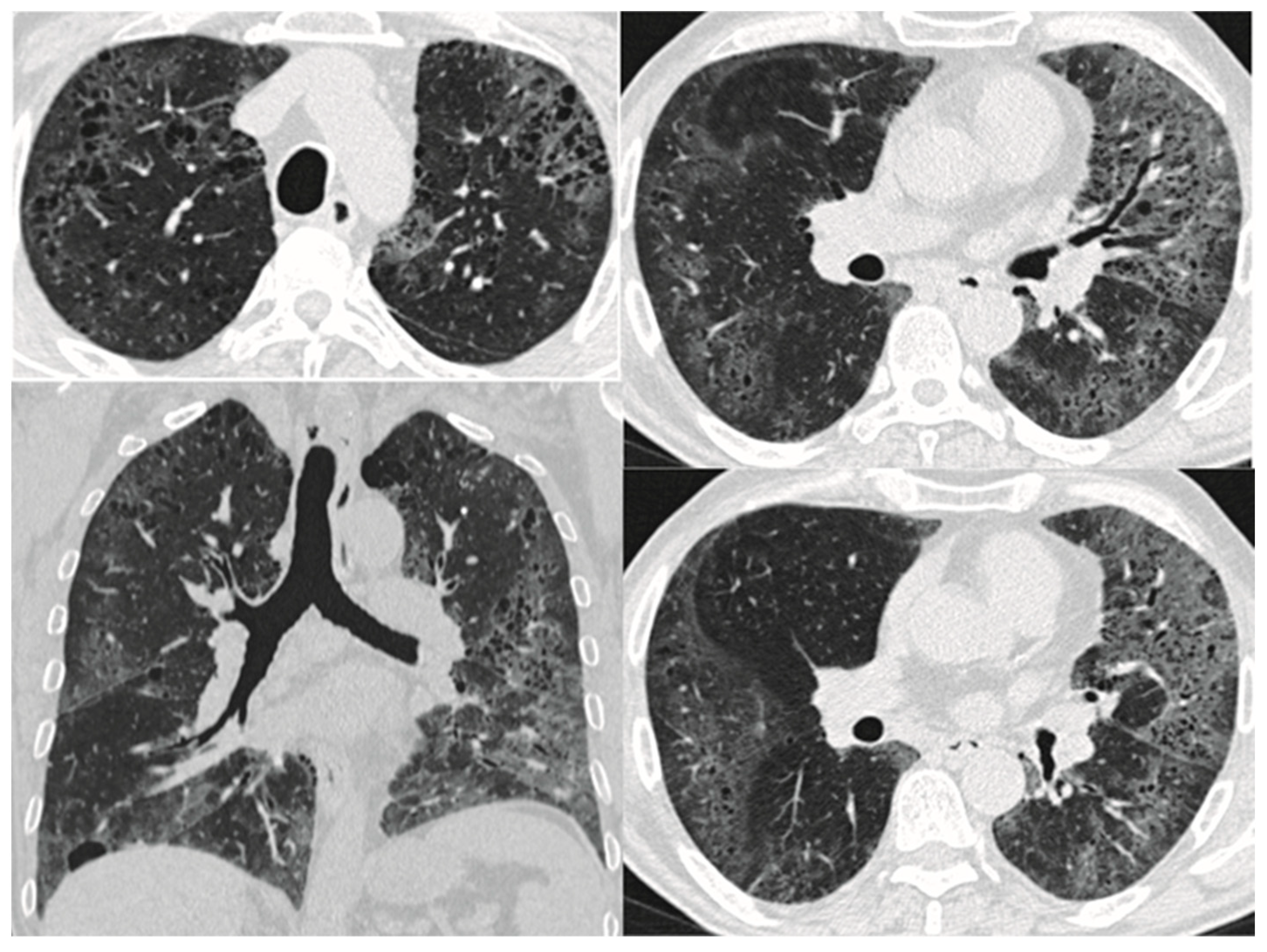
Besides the UIP pattern, several other patterns have been reported, such as non-specific interstitial pneumonia (NSIP) [9]; respiratory bronchiolitis-associated interstitial lung disease (RB-ILD), represented by poorly defined centrilobular nodules [2]; desquamative interstitial pneumonia (DIP) showing ground glass opacities; and smoking-related interstitial fibrosis (SRIF) (Figure 4) [12]. As the risk of lung cancer appears to be higher in CPFE than in IPF or COPD alone [56,57], patients with CPFE may develop lung nodules or masses.
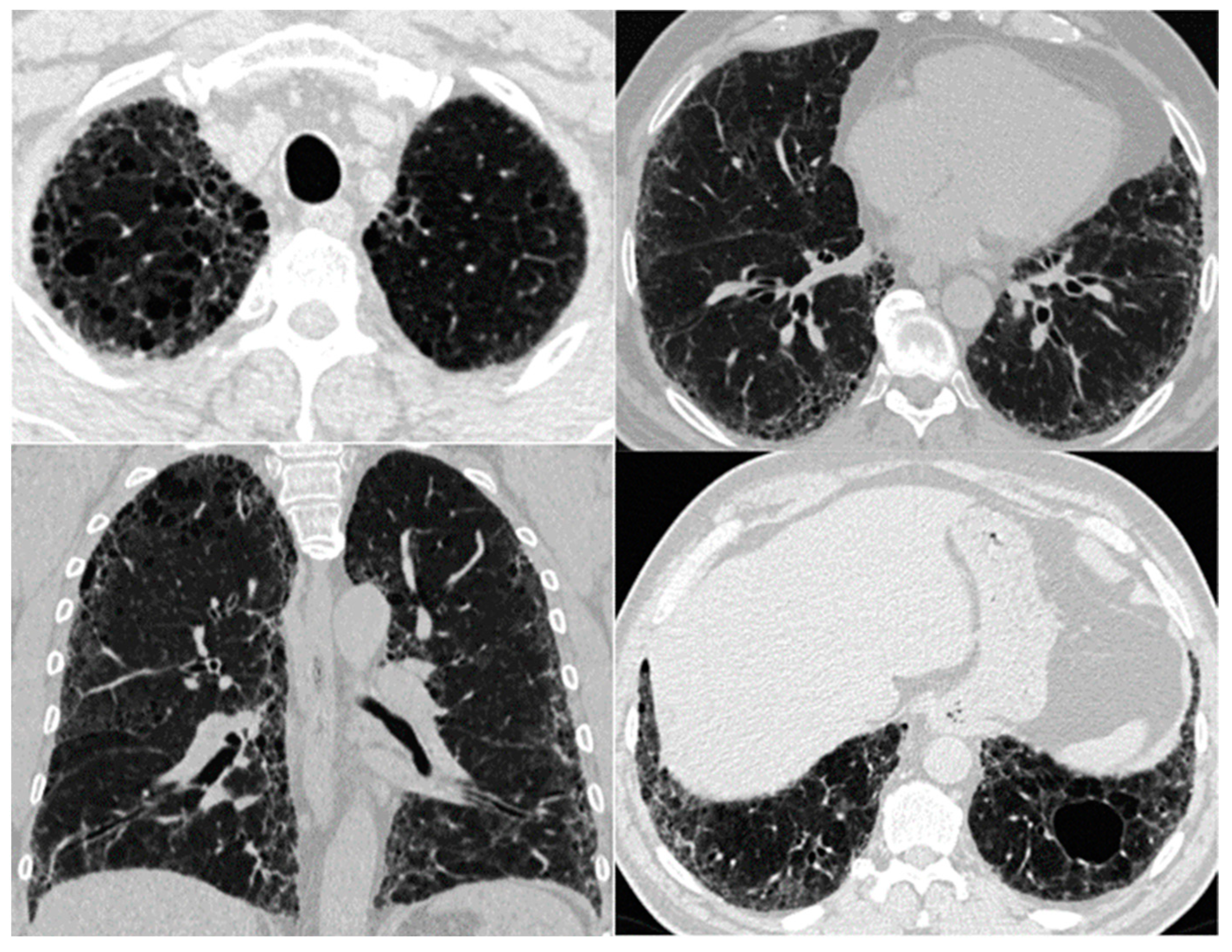
A distinctive imaging feature of CPFE that does not appear to be present in patients with IPF or emphysema alone is the thick-walled large cyst pattern resulting from the combination of emphysema and SRIF [6], i.e., development of pulmonary fibrosis in the emphysematous lung [55]. These cysts are larger than honeycombing cysts (>1 cm in diameter) and have a 1 mm wall thickness. They may be located in the upper lungs in subpleural areas or develop in the reticulation and/or honeycombing regions (Figure 2) [7].
It has been found that the presence of these large cystic lesions with thick walls in CPFE patients suggests greater severity of emphysema compared to patients with no such lesions [58].
9. Comorbidities
9.1. Lung Cancer
As smoking-related diseases, emphysema and IPF have been identified as independent risk factors for developing lung cancer [61,62].
CPFE patients appears to have a higher incidence of lung cancer (6.1–46.8%) [53] compared to IPF (7–20%) [62] or COPD (12–14%) [63]. The study published by Yoo and colleagues on IPF patients with lung cancer revealed that male gender, smoking at the time of IPF diagnosis, and an annual decline of 10% or more in FVC were risk factors for lung cancer [64]. Similarly, lung cancer in CPFE was typically diagnosed in elderly, heavy smokers who are predominately male with a median survival time of 19.5 months [65]. Another study revealed that lung cancer in CPFE more frequently has a squamous cell carcinoma histology and a lower lobe predominance occurring in the field of fibrosis, it is diagnosed in the advanced pathological stage, and is associated with increased mortality [66]. In addition, CPFE patients with concomitant non-small cell lung cancer (NSCLC) are at a greater risk for acute exacerbation than IPF patients with NSCLC [67], and thus have an increased mortality [53].
9.2. Pulmonary Hypertension
Pulmonary hypertension (PH) is a significant complication of COPD, IPF, and CPFE and is associated with a lower survival rate [68]. Approximately 50% of COPD cases, 31–46% of advanced IPF cases [68,69], and 15%–55% of CPFE patients are complicated by PH [6].
While PH in COPD or IPF patients is generally mild to moderate, in most CPFE cases, it is moderate to severe [69]. This severity is likely due to the combined effects of emphysema and fibrosis, leading to a reduction in the pulmonary capillary bed and hypoxic vascular constriction, resulting in a more severe increase in pulmonary vascular resistance. Furthermore, chronic inflammation induced by cigarette smoke in susceptible individuals may contribute to vascular remodeling [9]. Pulmonary artery intimal fibrosis and medial hypertrophy, thickening, and fibrosis of the pulmonary veins are among the changes that occur, leading to significant luminal obstruction and modest venopathy, but no apparent capillary alterations [70]. Interestingly, in CPFE-induced PH, narrowing of pulmonary arteries due to muscular layer hypertrophy is a global finding, even in areas of normal lung tissue [70].
PH becomes a dominant clinical feature and a major complication of CPFE, resulting in severe dyspnea, markedly impaired gas transfer (DLCO), and exercise hypoxemia, all of which contribute to a poor prognosis [6]. Given the added mechanisms contributing to increased pulmonary pressure, patients with CPFE and PH have a lower survival rate compared to patients with PH and IPF (25 vs. 34 months) [71] or COPD (5-year survival rate 25% vs. 36%) [68].
10. Treatment
Currently, there is limited evidence regarding CPFE treatment; therefore, management strategies are based solely on data derived from studies on COPD and IPF patients with concurrent CPFE. Encouraging general measures such as smoking cessation and avoiding environmental exposures may slow down disease progression [17,72]. Because infectious exacerbations significantly deteriorate lung function, vaccination against influenza viruses, COVID-19, and Streptococcus pneumoniae is considered beneficial [6].
Although inhaled bronchodilators with or without corticosteroids have shown to be effective in CPFE patients with significant airflow limitation [73,74], the evidence is scarce, and further studies are needed to address patients with preserved lung function.
Currently, only two drugs, pirfenidone and nintedanib, have proven efficacy in both IPF and fibrotic ILD, reducing the progression rate by half [75,76,77]. However, in patients with IPF who have emphysema, FVC decline, which is a traditional primary endpoint in most trials, is attenuated, and there is a lack of clear-cut efficacy in this group of patients. Despite this, the ATS/ERS/JRS/ALAT guideline suggests that antifibrotic medication may be beneficial for IPF patients with CPFE [6]. Similarly, patients with CTD-ILD or fibrotic HP and emphysema may benefit from therapy with glucocorticoids and/or immunosuppressive agents [78].
Regarding therapy for pulmonary hypertension, there is a significant discrepancy between controlled and uncontrolled data. As a result, there is limited evidence regarding the use of pulmonary vasodilators, leading to limited treatment options [79]. However, uncontrolled observational studies suggest that sildenafil may be beneficial for patients with IPF [80,81], and the current clinical guideline states that in patients with severe PH associated with ILD, phosphodiesterase 5-inhibitors may be considered, based on individual decision making [82]. In CPFE patients with hypoxemia at rest or during exercise, oxygen supplementation may alleviate pulmonary hypertension [74].
The approach to treating lung cancer in CPFE patients is similar to other patients. Unfortunately, the combined severity of emphysema and underlying fILD likely contribute to the greater complication rates among CPFE individuals receiving treatment [83]. Moreover, studies suggest a higher rate of exacerbation and malignancy recurrence compared to patients without CPFE, which increases the postsurgical risk of morbidity and mortality (Table 2).
11. Conclusions
CPFE is a distinct entity that sums up the pathogenic pathways found in both COPD and IPF, which determine the impaired regeneration of the lung parenchyma after damage. More research is needed to understand the coexistence of the divergent phenotypes of response to injury driven by environmental factors in CPFE. This entity has a wide variety of imaging and histopathological appearances. From the clinical perspective, CPFE combines the effects of emphysema and fibrosis, resulting in patients with increased symptoms that frequently associate with severe comorbidities such as lung cancer and pulmonary hypertension, which impose a poor prognosis and increased mortality. Treatment options are scarce, as they derive from studies on COPD and IPF patients with concurrent CPFE, and include similar recommendations with limited supporting evidence.
Author Contributions
Conceptualization, D.C. and A.C.; writing—original draft preparation, D.C.; writing—review and editing, D.C., A.G.M. and Z.L.; supervision, A.C.; project administration, A.C.; funding acquisition, A.G.M. All authors have read and agreed to the published version of the manuscript.
Funding
Alexander G. Mathioudakis was supported by the NIHR Manchester Biomedical Research Centre (NIHR203308) and by an NIHR Clinical Lectureship in Respiratory Medicine.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent was obtained from the patients to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Auerbach, O.; Garfinkel, L.; Hammond, E.C. Relation of Smoking and Age to Findings in Lung Parenchyma: A Microscopic Study. Chest 1974, 65, 29–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cottin, V.; Nunes, H.; Brillet, P.-Y.; Delaval, P.; Devouassaoux, G.; Tillie-Leblond, I.; Israel-Biet, D.; Court-Fortune, I.; Valeyre, D.; Cordier, J.-F. Combined pulmonary fibrosis and emphysema: A distinct underrecognised entity. Eur. Respir. J. 2005, 26, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Safiri, S.; Carson-Chahhoud, K.; Noori, M.; Nejadghaderi, S.A.; Sullman, M.J.M.; Heris, J.A.; Ansarin, K.; Mansournia, M.A.; Collins, G.S.; Kolahi, A.-A.; et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: Results from the Global Burden of Disease Study 2019. BMJ 2022, 378, e069679. [Google Scholar] [CrossRef] [PubMed]
- Maher, T.M.; Bendstrup, E.; Dron, L.; Langley, J.; Smith, G.; Khalid, J.M.; Patel, H.; Kreuter, M. Global incidence and prevalence of idiopathic pulmonary fibrosis. Respir. Res. 2021, 22, 197. [Google Scholar] [CrossRef]
- Cottin, V.; Hansell, D.M.; Sverzellati, N.; Weycker, D.; Antoniou, K.M.; Atwood, M.; Oster, G.; Kirchgaessler, K.-U.; Collard, H.R.; Wells, A.U. Effect of Emphysema Extent on Serial Lung Function in Patients with Idiopathic Pulmonary Fibrosis. Am. J. Respir. Crit. Care Med. 2017, 196, 1162–1171. [Google Scholar] [CrossRef]
- Cottin, V.; Selman, M.; Inoue, Y.; Wong, A.W.; Corte, T.J.; Flaherty, K.R.; Han, M.K.; Jacob, J.; Johannson, K.A.; Kitaichi, M.; et al. Syndrome of Combined Pulmonary Fibrosis and Emphysema: An Official ATS/ERS/JRS/ALAT Research Statement. Am. J. Respir. Crit. Care Med. 2022, 206, e7–e41. [Google Scholar] [CrossRef]
- Sakai, F.; Tominaga, J.; Kaga, A.; Usui, Y.; Kanazawa, M.; Ogura, T.; Yanagawa, N.; Takemura, T. Imaging Diagnosis of Interstitial Pneumonia with Emphysema (Combined Pulmonary Fibrosis and Emphysema). Pulm. Med. 2012, 2012, 816541. [Google Scholar] [CrossRef] [Green Version]
- Sangani, R.; Ghio, A.; Culp, S.; Patel, Z.; Sharma, S. Combined Pulmonary Fibrosis Emphysema: Role of Cigarette Smoking and Pulmonary Hypertension in a Rural Cohort. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 1873–1885. [Google Scholar] [CrossRef]
- Lin, H.; Jiang, S. Combined pulmonary fibrosis and emphysema (CPFE): An entity different from emphysema or pulmonary fibrosis alone. J. Thorac. Dis. 2015, 7, 767–779. [Google Scholar]
- Kitaguchi, Y.; Fujimoto, K.; Hayashi, R.; Hanaoka, M.; Honda, T.; Kubo, K. Annual changes in pulmonary function in combined pulmonary fibrosis and emphysema: Over a 5-year follow-up. Respir. Med. 2013, 107, 1986–1992. [Google Scholar] [CrossRef] [Green Version]
- Antoniou, K.M.; Walsh, S.L.; Hansell, D.M.; Rubens, M.R.; Marten, K.; Tennant, R.; Hansel, T.; Desai, S.R.; Siafakas, N.M.; du Bois, R.M.; et al. Smoking-related emphysema is associated with idiopathic pulmonary fibrosis and rheumatoid lung. Respirology 2013, 18, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- Jankowich, M.D.; Rounds, S.I. Combined Pulmonary Fibrosis and Emphysema Syndrome: A Review. Chest 2012, 141, 222–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kärkkäinen, M.; Kettunen, H.-P.; Nurmi, H.; Selander, T.; Purokivi, M.; Kaarteenaho, R. Effect of smoking and comorbidities on survival in idiopathic pulmonary fibrosis. Respir. Res. 2017, 18, 160. [Google Scholar] [CrossRef] [Green Version]
- Grubstein, A.; Bendayan, D.; Schactman, I.; Cohen, M.; Shitrit, D.; Kramer, M.R. Concomitant upper-lobe bullous emphysema, lower-lobe interstitial fibrosis and pulmonary hypertension in heavy smokers: Report of eight cases and review of the literature. Respir. Med. 2005, 99, 948–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cottin, V. The impact of emphysema in pulmonary fibrosis. Eur. Respir. Rev. 2013, 22, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Cottin, V.; Cordier, J.-F. Combined pulmonary fibrosis and emphysema in connective tissue disease. Curr. Opin. Pulm. Med. 2012, 18, 418–427. [Google Scholar] [CrossRef]
- Morse, D.; Rosas, I.O. Tobacco Smoke–Induced Lung Fibrosis and Emphysema. Annu. Rev. Physiol. 2014, 76, 493–513. [Google Scholar] [CrossRef]
- Ye, Q.; Huang, K.; Ding, Y.; Lou, B.; Hou, Z.; Dai, H.; Wang, C. Cigarette smoking contributes to idiopathic pulmonary fibrosis associated with emphysema. Chin. Med. J. 2014, 127, 469–474. [Google Scholar]
- Chae, K.J.; Jin, G.Y.; Jung, H.N.; Kwon, K.S.; Choi, H.; Lee, Y.C.; Chung, M.J.; Park, H.S. Differentiating Smoking-Related Interstitial Fibrosis (SRIF) from Usual Interstitial Pneumonia (UIP) with Emphysema Using CT Features Based on Pathologically Proven Cases. PLoS ONE 2016, 11, e0162231. [Google Scholar] [CrossRef] [Green Version]
- Kitaguchi, Y.; Fujimoto, K.; Hanaoka, M.; Kawakami, S.; Honda, T.; Kubo, K. Clinical characteristics of combined pulmonary fibrosis and emphysema. Respirology 2010, 15, 265–271. [Google Scholar] [CrossRef]
- Joshi, J.M.; Karkhanis, V.S. Combined pulmonary fibrosis and emphysema in a tyre industry worker. Lung India 2012, 29, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Roshan, R.; Gupta, M.; Kulshrestha, R.; Menon, B.; Chhabra, S. Combined Pulmonary Fibrosis and Emphysema in a welder. Monaldi Arch. Chest Dis. 2012, 77, 26–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cormier, Y.; Brown, M.; Worthy, S.; Racine, G.; Muller, N.L. High-resolution computed tomographic characteristics in acute farmer’s lung and in its follow-up. Eur. Respir. J. 2000, 16, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Jacob, J.; Song, J.W.; Yoon, H.-Y.; Cross, G.; Barnett, J.; Woo, W.L.; Adams, F.; Kokosi, M.; Devaraj, A.; Renzoni, E.; et al. Prevalence and Effects of Emphysema in Never-Smokers with Rheumatoid Arthritis Interstitial Lung Disease. Ebiomedicine 2018, 28, 303–310. [Google Scholar] [CrossRef] [Green Version]
- Antoniou, K.M.; Margaritopoulos, G.A.; Goh, N.S.; Karagiannis, K.; Desai, S.R.; Nicholson, A.G.; Siafakas, N.M.; Coghlan, J.G.; Denton, C.P.; Hansell, D.M.; et al. Combined Pulmonary Fibrosis and Emphysema in Scleroderma-Related Lung Disease Has a Major Confounding Effect on Lung Physiology and Screening for Pulmonary Hypertension. Arthritis Rheumatol. 2016, 68, 1004–1012. [Google Scholar] [CrossRef]
- Gocho, K.; Sugino, K.; Sato, K.; Hasegawa, C.; Uekusa, T.; Homma, S. Microscopic polyangiitis preceded by combined pulmonary fibrosis and emphysema. Respir. Med. Case Rep. 2015, 15, 128–132. [Google Scholar] [CrossRef] [Green Version]
- Tzouvelekis, A.; Zacharis, G.; Oikonomou, A.; Mikroulis, D.; Margaritopoulos, G.; Koutsopoulos, A.; Antoniadis, A.; Koulelidis, A.; Steiropoulos, P.; Boglou, P.; et al. Increased incidence of autoimmune markers in patients with combined pulmonary fibrosis and emphysema. BMC Pulm. Med. 2013, 13, 31. [Google Scholar] [CrossRef] [Green Version]
- Manni, M.; Oury, T. Oxidative Stress and Pulmonary Fibrosis. In Systems Biology of Free Radicals and Antioxidants; Laher, I., Ed.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 1611–1631. [Google Scholar]
- Marginean, C.; Popescu, M.S.; Vladaia, M.; Tudorascu, D.; Pirvu, D.C.; Petrescu, F. Involvement of Oxidative Stress in COPD. Curr. Health Sci. J. 2018, 44, 48–55. [Google Scholar]
- Finicelli, M.; Digilio, F.A.; Galderisi, U.; Peluso, G. The Emerging Role of Macrophages in Chronic Obstructive Pulmonary Disease: The Potential Impact of Oxidative Stress and Extracellular Vesicle on Macrophage Polarization and Function. Antioxidants 2022, 11, 464. [Google Scholar] [CrossRef]
- Estornut, C.; Milara, J.; Bayarri, M.A.; Belhadj, N.; Cortijo, J. Targeting Oxidative Stress as a Therapeutic Approach for Idiopathic Pulmonary Fibrosis. Front. Pharmacol. 2022, 12, 794997. [Google Scholar] [CrossRef]
- Duckworth, A.; Gibbons, M.A.; Allen, R.J.; Almond, H.; Beaumont, R.N.; Wood, A.R.; Lunnon, K.; Lindsay, M.A.; Wain, L.V.; Tyrrell, J.; et al. Telomere length and risk of idiopathic pulmonary fibrosis and chronic obstructive pulmonary disease: A mendelian randomisation study. Lancet Respir. Med. 2021, 9, 285–294. [Google Scholar] [CrossRef] [PubMed]
- van Moorsel, C.H.; van Oosterhout, M.F.; Barlo, N.P.; de Jong, P.A.; van der Vis, J.J.; Ruven, H.J.; van Es, H.W.; van den Bosch, J.M.; Grutters, J.C. Surfactant protein C mutations are the basis of a significant portion of adult familial pulmonary fibrosis in a dutch cohort. Am. J. Respir. Crit. Care Med. 2010, 182, 1419–1425. [Google Scholar] [CrossRef]
- Cronkhite, J.T.; Xing, C.; Raghu, G.; Chin, K.M.; Torres, F.; Rosenblatt, R.L.; Garcia, C.K. Faculty Opinions recommendation of Telomere shortening in familial and sporadic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 2008, 178, 729–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanaoka, M.; Ito, M.; Droma, Y.; Ushiki, A.; Kitaguchi, Y.; Yasuo, M.; Kubo, K. Comparison of gene expression profiling between lung fibrotic and emphysematous tissues sampled from patients with combined pulmonary fibrosis and emphysema. Fibrogenesis Tissue Repair 2012, 5, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, O.M.; Baldi, B.G.; Costa, A.N.; Carvalho, C.R.R. Combined pulmonary fibrosis and emphysema: An increasingly recognized condition. J. Bras. Pneumol. 2014, 40, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Liang, B.; Yang, J.; Xiao, J.; Ma, C.; Xu, S.; Lei, J.; Xu, X.; Liao, Z.; Liu, H.; et al. Association of FAM13A polymorphisms with COPD and COPD-related phenotypes in Han Chinese. Clin. Biochem. 2013, 46, 1683–1688. [Google Scholar] [CrossRef]
- Fingerlin, T.E.; Murphy, E.; Zhang, W.; Peljto, A.L.; Brown, K.K.; Steele, M.P.; Loyd, J.E.; Cosgrove, G.P.; Lynch, D.; Groshong, S.; et al. Genome-wide association study identifies multiple susceptibility loci for pulmonary fibrosis. Nat. Genet. 2013, 45, 613–620. [Google Scholar] [CrossRef] [Green Version]
- Hobbs, B.D.; de Jong, K.; Lamontagne, M.; Bossé, Y.; Shrine, N.; Artigas, M.S.; Wain, L.V.; Hall, I.P.; Jackson, V.E.; COPDGene Investigators; et al. Genetic loci associated with chronic obstructive pulmonary disease overlap with loci for lung function and pulmonary fibrosis. Nat. Genet. 2017, 49, 426–432. [Google Scholar] [CrossRef] [Green Version]
- Kinjo, T.; Kitaguchi, Y.; Droma, Y.; Yasuo, M.; Wada, Y.; Ueno, F.; Ota, M.; Hanaoka, M. The Gly82Ser mutation in AGER contributes to pathogenesis of pulmonary fibrosis in combined pulmonary fibrosis and emphysema (CPFE) in Japanese patients. Sci. Rep. 2020, 10, 12811. [Google Scholar] [CrossRef]
- Xu, L.; Bian, W.; Gu, X.-H.; Shen, C. Genetic polymorphism in matrix metalloproteinase-9 and transforming growth factor-β1 and susceptibility to combined pulmonary fibrosis and emphysema in a Chinese population. Kaohsiung J. Med. Sci. 2017, 33, 124–129. [Google Scholar] [CrossRef]
- Guzmán-Vargas, J.; Ambrocio-Ortiz, E.; Pérez-Rubio, G.; Ponce-Gallegos, M.A.; Hernández-Zenteno, R.D.J.; Mejía, M.; Ramírez-Venegas, A.; Buendia-Roldan, I.; Falfán-Valencia, R. Differential Genomic Profile in TERT, DSP, and FAM13A Between COPD Patients With Emphysema, IPF, and CPFE Syndrome. Front. Med. 2021, 8, 725144. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.J.; Hobbs, B.D.; Yun, J.H.; Saferali, A.; Moll, M.; Xu, Z.; Chase, R.P.; Morrow, J.; Ziniti, J.; Sciurba, F.; et al. Lung tissue shows divergent gene expression between chronic obstructive pulmonary disease and idiopathic pulmonary fibrosis. Respir. Res. 2022, 23, 97. [Google Scholar] [CrossRef] [PubMed]
- Spagnolo, P.; Semenzato, U. Revealing the pathogenic and ageing-related mechanisms of the enigmatic idiopathic pulmonary fibrosis (and chronic obstructive pulmonary disease). Curr. Opin. Pulm. Med. 2022, 28, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Murray, L.A. Commonalities between the pro-fibrotic mechanisms in COPD and IPF. Pulm. Pharmacol. Ther. 2012, 25, 276–280. [Google Scholar] [CrossRef]
- Beghé, B.; Cerri, S.; Fabbri, L.M.; Marchioni, A. COPD, Pulmonary Fibrosis and ILAs in Aging Smokers: The Paradox of Striking Different Responses to the Major Risk Factors. Int. J. Mol. Sci. 2021, 22, 9292. [Google Scholar] [CrossRef]
- Miravitlles, M.; Ribera, A. Understanding the impact of symptoms on the burden of COPD. Respir. Res. 2017, 18, 67. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.S.; Mira-Avendano, I.; Ryu, J.H.; Daniels, C.E. The burden of idiopathic pulmonary fibrosis: An unmet public health need. Respir. Med. 2014, 108, 955–967. [Google Scholar] [CrossRef] [Green Version]
- Mann, J.; Goh, N.S.L.; Holland, A.E.; Khor, Y.H. Cough in Idiopathic Pulmonary Fibrosis. Front. Rehabil. Sci. 2021, 2, 751798. [Google Scholar] [CrossRef]
- Costa, C.M.; Neder, J.A.; Verrastro, C.G.; Paula-Ribeiro, M.; Ramos, R.; Ferreira, E.M.; Nery, L.E.; O’Donnell, D.E.; Pereira, C.A.; Ota-Arakaki, J. Uncovering the mechanisms of exertional dyspnoea in combined pulmonary fibrosis and emphysema. Eur. Respir. J. 2020, 55, 1901319. [Google Scholar] [CrossRef]
- Cottin, V.; Le Pavec, J.; Prévot, G.; Mal, H.; Humbert, M.; Simonneau, G.; Cordier, J.F. Pulmonary hypertension in patients with combined pulmonary fibrosis and emphysema syndrome. Eur. Respir. J. 2010, 35, 105–111. [Google Scholar] [CrossRef]
- Kusaka, K.; Morio, Y.; Kimura, Y.; Takeda, K.; Kawashima, M.; Masuda, K.; Matsui, H. Improvement of pulmonary arterial compliance by pulmonary vasodilator in pulmonary hypertension from combined pulmonary fibrosis and emphysema. Respir. Med. Case Rep. 2019, 28, 100940. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.Y.; Lee, Y.S.; Min, K.H.; Hur, G.Y.; Lee, S.Y.; Kang, K.H.; Shim, J.J. Impact and prognosis of lung cancer in patients with combined pulmonary fibrosis and emphysema. Sarcoidosis Vasc. Diffus. Lung Dis. 2020, 37, e2020020. [Google Scholar]
- Çiftci, F.; Gülpınar, B.; Atasoy, Ç.; Kayacan, O.; Saryal, S. Combined pulmonary fibrosis and emphysema: How does cohabitation affect respiratory functions? Adv. Med. Sci. 2019, 64, 285–291. [Google Scholar] [CrossRef]
- Brillet, P.; Cottin, V.; Letoumelin, P.; Landino, F.; Brauner, M.; Valeyre, D.; Cordier, J.; Nunes, H. Combined apical emphysema and basal fibrosis syndrome [emphysema/fibrosis syndrome]: CT imaging features and pulmonary function tests. Clin. Imaging 2009, 33, 332. (In French) [Google Scholar] [CrossRef]
- Sekine, Y.; Katsura, H.; Koh, E.; Hiroshima, K.; Fujisawa, T. Early detection of COPD is important for lung cancer surveillance. Eur. Respir. J. 2011, 39, 1230–1240. [Google Scholar] [CrossRef] [Green Version]
- Mimae, T.; Suzuki, K.; Tsuboi, M.; Ikeda, N.; Takamochi, K.; Aokage, K.; Shimada, Y.; Miyata, Y.; Okada, M. Severity of lung fibrosis affects early surgical outcomes of lung cancer among patients with combined pulmonary fibrosis and emphysema. Medicine 2016, 95, e4314. [Google Scholar] [CrossRef] [PubMed]
- IInomata, M.; Ikushima, S.; Awano, N.; Kondoh, K.; Satake, K.; Masuo, M.; Kusunoki, Y.; Moriya, A.; Kamiya, H.; Ando, T.; et al. An autopsy study of combined pulmonary fibrosis and emphysema: Correlations among clinical, radiological, and pathological features. BMC Pulm. Med. 2014, 14, 104. [Google Scholar] [CrossRef] [Green Version]
- Ando, K.; Sekiya, M.; Tobino, K.; Takahashi, K. Relationship Between Quantitative CT Metrics and Pulmonary Function in Combined Pulmonary Fibrosis and Emphysema. Lung 2013, 191, 585–591. [Google Scholar] [CrossRef]
- Matsuoka, S.; Yamashiro, T.; Matsushita, S.; Fujikawa, A.; Kotoku, A.; Yagihashi, K.; Kurihara, Y.; Nakajima, Y. Morphological disease progression of combined pulmonary fibrosis and emphysema: Comparison with emphysema alone and pulmonary fibrosis alone. J. Comput. Assist. Tomogr. 2015, 39, 153–159. [Google Scholar] [CrossRef]
- Wilson, D.O.; Weissfeld, J.L.; Balkan, A.; Schragin, J.G.; Fuhrman, C.R.; Fisher, S.N.; Wilson, J.; Leader, J.K.; Siegfried, J.M.; Shapiro, S.D.; et al. Association of radiographic emphysema and airflow obstruction with lung cancer. Am. J. Respir. Crit. Care Med. 2008, 178, 738–744. [Google Scholar] [CrossRef] [Green Version]
- Ballester, B.; Milara, J.; Cortijo, J. Idiopathic Pulmonary Fibrosis and Lung Cancer: Mechanisms and Molecular Targets. Int. J. Mol. Sci. 2019, 20, 593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, C.; Sun, S.-W.; Xiong, X.-Z. From COPD to Lung Cancer: Mechanisms Linking, Diagnosis, Treatment, and Prognosis. Int. J. Chronic Obstr. Pulm. Dis. 2022, 17, 2603–2621. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.; Jeong, B.-H.; Chung, M.J.; Lee, K.S.; Kwon, O.J.; Chung, M.P. Risk factors and clinical characteristics of lung cancer in idiopathic pulmonary fibrosis: A retrospective cohort study. BMC Pulm. Med. 2019, 19, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, H.J.; Do, K.-H.; Lee, J.B.; Alblushi, S.; Lee, S.M. Lung Cancer in Combined Pulmonary Fibrosis and Emphysema: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0161437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.; Wu, W.; Chen, N.; Song, H.; Lu, T.; Yang, Z.; Wang, Z.; Zhou, J.; Liu, L. Clinical characteristics and outcomes of lung cancer patients with combined pulmonary fibrosis and emphysema: A systematic review and meta-analysis of 13 studies. J. Thorac. Dis. 2017, 9, 5322–5334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, S.W.; Park, M.S.; Kim, Y.S.; Jang, J.; Lee, J.H.; Lee, C.-T.; Chung, J.-H.; Shim, H.S.; Lee, K.W.; Kim, S.-S.; et al. Combined pulmonary fibrosis and emphysema and idiopathic pulmonary fibrosis in non-small cell lung cancer: Impact on survival and acute exacerbation. BMC Pulm. Med. 2019, 19, 177. [Google Scholar] [CrossRef] [Green Version]
- Seeger, W.; Adir, Y.; Barberà, J.A.; Champion, H.; Coghlan, J.G.; Cottin, V.; De Marco, T.; Galiè, N.; Ghio, S.; Gibbs, S.; et al. Pulmonary hypertension in chronic lung diseases. J. Am. Coll. Cardiol. 2013, 62, D109–D116. [Google Scholar] [CrossRef]
- Caminati, A.; Cassandro, R.; Harari, S.; Wener, R.R.; Bel, E.H. Pulmonary hypertension in chronic interstitial lung diseases. Eur. Respir. Rev. 2013, 22, 292–301. [Google Scholar] [CrossRef]
- Sato, T.; Tsujino, I.; Tanino, M.; Ohira, H.; Nishimura, M. Broad and heterogeneous vasculopathy in pulmonary fibrosis and emphysema with pulmonary hypertension. Respirol. Case Rep. 2013, 1, 10–13. [Google Scholar] [CrossRef]
- Mejía, M.; Carrillo, G.; Rojas-Serrano, J.; Estrada, A.; Suárez, T.; Alonso, D.; Barrientos, E.; Gaxiola, M.; Navarro, C.; Selman, M. Idiopathic pulmonary fibrosis and emphysema: Decreased survival associated with severe pulmonary arterial hypertension. Chest 2009, 136, 10–15. [Google Scholar] [CrossRef]
- 2023 Gold Report. Global Strategy for Prevention, Diagnosis and Management of COPD: 2023 Report. Available online: https://goldcopd.org/2023-gold-report-2/ (accessed on 26 May 2023).
- Dong, F.; Zhang, Y.; Chi, F.; Song, Q.; Zhang, L.; Wang, Y.; Che, C. Clinical efficacy and safety of ICS/LABA in patients with combined idiopathic pulmonary fibrosis and emphysema. Int. J. Clin. Exp. Med. 2015, 8, 8617–8625. [Google Scholar] [PubMed]
- Zhang, L.; Zhang, C.; Dong, F.; Song, Q.; Chi, F.; Liu, L.; Wang, Y.; Che, C. Combined pulmonary fibrosis and emphysema: A retrospective analysis of clinical characteristics, treatment and prognosis. BMC Pulm. Med. 2016, 16, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richeldi, L.; Du Bois, R.M.; Raghu, G.; Azuma, A.; Brown, K.K.; Costabel, U.; Cottin, V.; Flaherty, K.R.; Hansell, D.M.; Inoue, Y.; et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2071–2082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, T.E., Jr.; Bradford, W.Z.; Castro-Bernardini, S.; Fagan, E.A.; Glaspole, I.; Glassberg, M.K.; Gorina, E.; Hopkins, P.M.; Kardatzke, D.; Lancaster, L.; et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2083–2092. [Google Scholar] [CrossRef] [Green Version]
- Flaherty, K.R.; Wells, A.U.; Cottin, V.; Devaraj, A.; Walsh, S.L.; Inoue, Y.; Richeldi, L.; Kolb, M.; Tetzlaff, K.; Stowasser, S.; et al. Nintedanib in Progressive Fibrosing Interstitial Lung Diseases. N. Engl. J. Med. 2019, 381, 1718–1727. [Google Scholar] [CrossRef] [Green Version]
- Wijsenbeek, M.; Cottin, V. Spectrum of Fibrotic Lung Diseases. N. Engl. J. Med. 2020, 383, 958–968. [Google Scholar] [CrossRef]
- Nathan, S.D.; Barbera, J.A.; Gaine, S.P.; Harari, S.; Martinez, F.J.; Olschewski, H.; Olsson, K.M.; Peacock, A.J.; Pepke-Zaba, J.; Provencher, S.; et al. Pulmonary hypertension in chronic lung disease and hypoxia. Eur. Respir. J. 2019, 53, 1801914. [Google Scholar] [CrossRef] [Green Version]
- Kolb, M.; Raghu, G.; Wells, A.U.; Behr, J.; Richeldi, L.; Schinzel, B.; Quaresma, M.; Stowasser, S.; Martinez, F.J. Nintedanib plus Sildenafil in Patients with Idiopathic Pulmonary Fibrosis. N. Engl. J. Med. 2018, 379, 1722–1731. [Google Scholar] [CrossRef]
- Zimmermann, G.S.; Von Wulffen, W.; Huppmann, P.; Meis, T.; Ihle, F.; Geiseler, J.; Leuchte, H.H.; Tufman, A.; Behr, J.; Neurohr, C. Haemodynamic changes in pulmonary hypertension in patients with interstitial lung disease treated with PDE-5 inhibitors. Respirology 2014, 19, 700–706. [Google Scholar] [CrossRef]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef]
- Girard, N.; Marchand-Adam, S.; Naccache, J.-M.; Borie, R.; Urban, T.; Jouneau, S.; Marchand, E.; Ravel, A.-C.; Kiakouama, L.; Etienne-Mastroianni, B.; et al. Lung Cancer in Combined Pulmonary Fibrosis and Emphysema: A Series of 47 Western Patients. J. Thorac. Oncol. 2014, 9, 1162–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Factors associated with Combined Pulmonary Fibrosis and Emphysema. Abbreviations: IPF—idiopathic pulmonary fibrosis, CTD-ILD—connective tissue disease-associated interstitial lung disease, RA-ILD—rheumatoid arthritis-associated interstitial lung disease, SS-ILD—systemic sclerosis-associated interstitial lung disease, c-ANCA—antineutrophil cytoplasmic autoantibody, fHP—fibrotic hypersensitivity pneumonitis.
Figure 1.
Factors associated with Combined Pulmonary Fibrosis and Emphysema. Abbreviations: IPF—idiopathic pulmonary fibrosis, CTD-ILD—connective tissue disease-associated interstitial lung disease, RA-ILD—rheumatoid arthritis-associated interstitial lung disease, SS-ILD—systemic sclerosis-associated interstitial lung disease, c-ANCA—antineutrophil cytoplasmic autoantibody, fHP—fibrotic hypersensitivity pneumonitis.

Figure 2.
HRCT patterns in CPFE. A predominant pattern of centrilobular emphysema in the upper lobes and a thick-walled cyst in the lower left lung zone in a field of fibrotic lesions in a 60-year-old patient diagnosed with idiopathic pulmonary fibrosis.
Figure 2.
HRCT patterns in CPFE. A predominant pattern of centrilobular emphysema in the upper lobes and a thick-walled cyst in the lower left lung zone in a field of fibrotic lesions in a 60-year-old patient diagnosed with idiopathic pulmonary fibrosis.

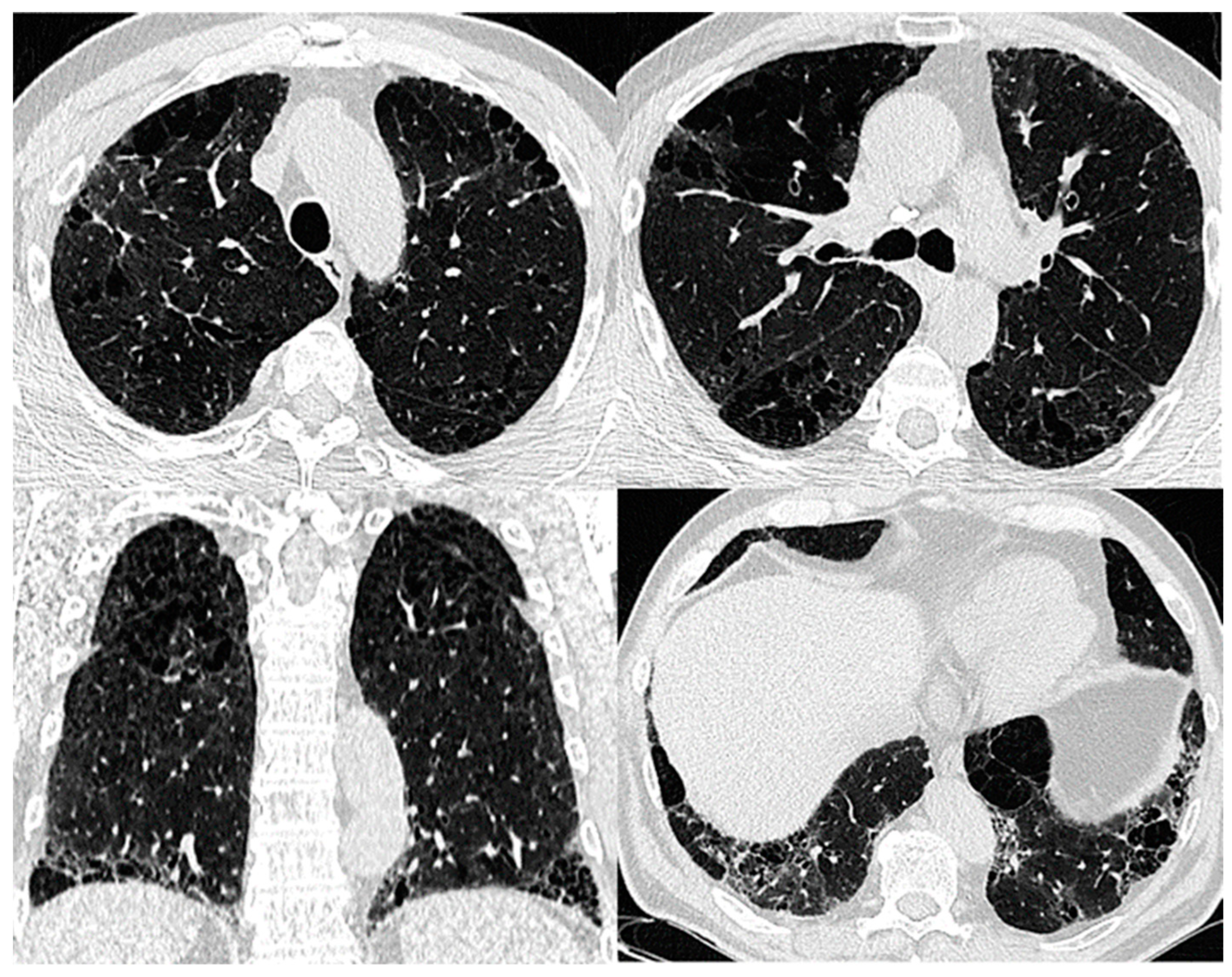
Figure 3.
Progressive transition HRCT pattern of CPFE. The typical distribution: predominant pattern of centrilobular emphysema in the upper lobes, extending to a panlobular emphysema in the midzones, and an isolated area of centrilobular emphysema in the left lower lobe in the field of subpleural reticular opacities, traction bronchiectasis, and bronchioloectasis in a 59-year-old patient with fibrotic hypersensitivity pneumonitis with a history of 30 pack-years of smoking.
Figure 3.
Progressive transition HRCT pattern of CPFE. The typical distribution: predominant pattern of centrilobular emphysema in the upper lobes, extending to a panlobular emphysema in the midzones, and an isolated area of centrilobular emphysema in the left lower lobe in the field of subpleural reticular opacities, traction bronchiectasis, and bronchioloectasis in a 59-year-old patient with fibrotic hypersensitivity pneumonitis with a history of 30 pack-years of smoking.

Figure 4.
HRCT pattern of emphysema admixed with DIP. Areas of low attenuation (emphysema) are mixed with ground-glass opacities (areas of high attenuation) and periemphysematous thickening.
Figure 4.
HRCT pattern of emphysema admixed with DIP. Areas of low attenuation (emphysema) are mixed with ground-glass opacities (areas of high attenuation) and periemphysematous thickening.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Distinctive functional features of CPFE compared to its separate components.
| Pulmonary Function Test Variable | CPFE | Fibrotic ILD | Emphysema |
|---|---|---|---|
| FVC | N/↓ | ↓ | N/↓ |
| FEV1 | N/↓ | ↓ | N/↓ |
| FEV1/FVC | N/↓/↑ | N/↑ | N/↓ |
| TLC | N/↓/↑ | N/↓ | ↑ |
| FRC | N/↓/↑ | N/↓ | ↑ |
| RV | N/↓/↑ | N/↓ | ↑ |
| DLCO | ↓ disproportionately | ↓ | ↓ |
| KCO | ↓↓ | N/↓ | ↓ |
| SaO2 following 6 min walk test | ↓↓ | ↓ | ↓ |
Abbreviations: FVC—forced vital capacity, FEV1—forced expiratory volume in the 1st second, FEV1/FVC—Tiffeneau index, TLC—total lung capacity, FRC—functional residual capacity, RV—residual volume, DLCO—diffusion lung capacity for carbon monoxide, KCO—carbon monoxide transfer coefficient, SaO2—oxygen saturation, N—normal, ↓—decreased, ↓↓—very decreased, ↑—increased.
Table 2.
Comparative features of CPFE with COPD and IPF.
| COPD | CPFE | IPF | |
|---|---|---|---|
| Prevalence | ↑↑↑ | ↓↓ | ↓ |
| Smoking history | ↑↑↑ | ↑↑↑/− | ↑ |
| Gender predilection | male predominance | male predominance | male predominance |
| Age of clinical manifestations | 5th–6th decade | 6th–7th decade/earlier in CTD-ILD | 5th–6th decade |
| Spectrum of environmental exposures | Tobacco, air pollution | Tobacco, noxious particles, or gases other than tobacco, asbestos, silica dust, and agrochemical chemicals, organic dust | Organic dust, metal and mineral dust, wood dust, asbestos, and ambient particulate matter |
| Autoimmunity | − | −/+ | − |
| Response to oxidative stress | cellular injury and death and ECM ↓ | cellular injury and death and ECM ↓ in the upper lobes, Activation of fibroblasts, ECM ↑ in the lower lobes | Activation of fibroblasts, ECM ↑ |
| Role of epigenetic factors | |||
| ↓ | ↑ | ↑ |
| ↑ | ↑ | ↓ |
| ↓ | ↑ | ↑ |
| − | ↓ | ↓ |
| Pathology | Small airways remodeling, fibrosis, and destruction of the lung parenchyma with an upper lobe predominance | Emphysema in the upper lobes and patchy fibrosis, fibroblast foci, and honeycombing—UIP/NSIP/DIP pattern—in the lower lobes. Presence of thick-walled cysts on a UIP background | Lung parenchyma and interstitium, with a lower lobe predilection |
| Clinical features | |||
| Cough with sputum production, dyspnea later in the disease course | Dyspnea, dry cough later in the disease course | Dyspnea, dry cough later in the disease course |
| − | + | + |
| Not a typical sign | 50% | 70% |
| Lung function | Obstruction +/− Low DLCO | Normal Low DLCO | Restriction Low DLCO |
| Imaging | Centrilobular and/or bullous emphysema | Coexistence of paraseptal emphysema in the upper zones of the lungs and the UIP/NSIP/DIP in the lower zones, thick-walled cysts in the area of fibrosis | UIP pattern |
| Comorbidities | |||
| ↑ | ↑↑ | ↑ |
| ↑ | ↑↑ | ↑ |
| Treatment options | Bronchodilators +/− ICS +/− Oxygen therapy | Bronchodilators +/− ICS Antifibrotics (pirfenidone, nintedanib) Oxygen therapy | Antifibrotics (pirfenidone, nintedanib) Oxygen therapy |
Abbreviations: ↑increased, ↑↑ - moderately increased, ↑↑↑ - very increased ↓—decreased, ↓↓ - moderately decreased, “+”—present, “−”—absent, ECM—extracellular matrix, UIP—usual interstitial pneumonitis, NSIP—nonspecific interstitial pneumonitis, DIP—desquamative interstitial pneumonitis, ICS—inhaled corticosteroids.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Calaras, D.; Mathioudakis, A.G.; Lazar, Z.; Corlateanu, A. Combined Pulmonary Fibrosis and Emphysema: Comparative Evidence on a Complex Condition. Biomedicines 2023, 11, 1636. https://doi.org/10.3390/biomedicines11061636
AMA Style
Calaras D, Mathioudakis AG, Lazar Z, Corlateanu A. Combined Pulmonary Fibrosis and Emphysema: Comparative Evidence on a Complex Condition. Biomedicines. 2023; 11(6):1636. https://doi.org/10.3390/biomedicines11061636
Chicago/Turabian StyleCalaras, Diana, Alexander G. Mathioudakis, Zsofia Lazar, and Alexandru Corlateanu. 2023. "Combined Pulmonary Fibrosis and Emphysema: Comparative Evidence on a Complex Condition" Biomedicines 11, no. 6: 1636. https://doi.org/10.3390/biomedicines11061636
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.