Clinical Characteristics and Prognosis of the Modified Probable Pneumocystis jirovecii Pneumonia in Korean Children, 2001–2021

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Annual Numbers of P. jirovecii Detection and PCP Diagnosis
3.2. Clinical Characteristics of Children with mp-PCP
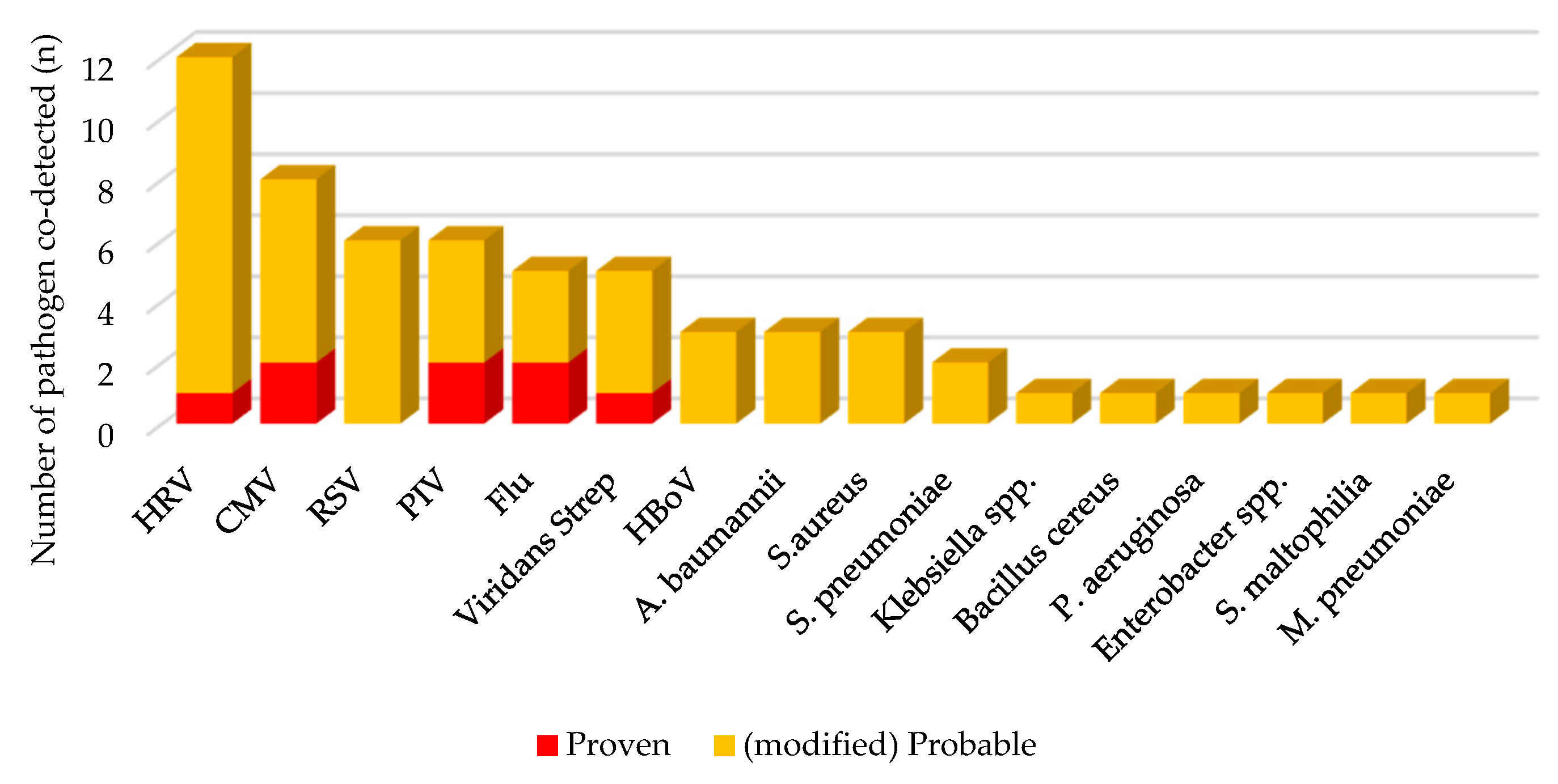
3.3. Co-Detected Respiratory Pathogens in Clinical PCP
3.4. Factors Associated with Death in Clinical PCP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, C.F., Jr.; Limper, A.H. Pneumocystis pneumonia. N. Engl. J. Med. 2004, 350, 2487–2498. [Google Scholar] [CrossRef]
- Pyrgos, V.; Shoham, S.; Roilides, E.; Walsh, T.J. Pneumocystis pneumonia in children. Paediatr. Respir. Rev. 2009, 10, 192–198. [Google Scholar] [CrossRef]
- Kim, S.Y.R.; Sung, H.; Lee, J. Clinical Characteristics, Prognostic Factors and Influence of Prophylaxis in Children with Pneumocystis jirovecii Pneumonia. Pediatr. Infect. Vaccine 2016, 23, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Ling, C.; Qian, S.; Wang, Q.; Zeng, J.; Jia, X.; Liu, J.; Li, Z. Pneumocystis pneumonia in non-HIV children: A 10-year retrospective study. Clin. Respir. J. 2018, 12, 16–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proudfoot, R.H.; Phillips, B. UK paediatric oncology Pneumocystis jirovecii pneumonia surveillance study. Arch. Dis. Child. 2021, 106, 994–998. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagrou, K.; Chen, S.; Masur, H.; Viscoli, C.; Decker, C.F.; Pagano, L.; Groll, A.H. Pneumocystis jirovecii Disease: Basis for the Revised EORTC/MSGERC Invasive Fungal Disease Definitions in Individuals Without Human Immunodeficiency Virus. Clin. Infect. Dis. 2021, 72 (Suppl. 2), S114–S120. [Google Scholar] [CrossRef] [PubMed]
- Choe, P.G.; Kang, Y.M.; Kim, G.; Park, W.B.; Park, S.W.; Kim, H.B.; Oh, M.D.; Kim, E.C.; Kim, N.J. Diagnostic value of direct fluorescence antibody staining for detecting Pneumocystis jirovecii in expectorated sputum from patients with HIV infection. Med. Mycol. 2014, 52, 326–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bateman, M.; Oladele, R.; Kolls, J.K. Diagnosing Pneumocystis jirovecii pneumonia: A review of current methods and novel approaches. Med. Mycol. 2020, 58, 1015–1028. [Google Scholar] [CrossRef] [PubMed]
- Alanio, A.; Desoubeaux, G.; Sarfati, C.; Hamane, S.; Bergeron, A.; Azoulay, E.; Molina, J.M.; Derouin, F.; Menotti, J. Real-time PCR assay-based strategy for differentiation between active Pneumocystis jirovecii pneumonia and colonization in immunocompromised patients. Clin. Microbiol. Infect. 2011, 17, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Perret, T.; Kritikos, A.; Hauser, P.M.; Guiver, M.; Coste, A.T.; Jaton, K.; Lamoth, F. Ability of quantitative PCR to discriminate Pneumocystis jirovecii pneumonia from colonization. J. Med. Microbiol. 2020, 69, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Morjaria, S.; Frame, J.; Franco-Garcia, A.; Geyer, A.; Kamboj, M.; Babady, N.E. Clinical Performance of (1,3) Beta-D Glucan for the Diagnosis of Pneumocystis Pneumonia (PCP) in Cancer Patients Tested With PCP Polymerase Chain Reaction. Clin. Infect. Dis. 2019, 69, 1303–1309. [Google Scholar] [CrossRef] [PubMed]
- Mantadakis, E. Pneumocystis jirovecii Pneumonia in Children with Hematological Malignancies: Diagnosis and Approaches to Management. J. Fungi. 2020, 6, 331. [Google Scholar] [CrossRef] [PubMed]
- Yong, M.K.; Slavin, M.A.; Kontoyiannis, D.P. Invasive fungal disease and cytomegalovirus infection: Is there an association? Curr. Opin. Infect. Dis. 2018, 31, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Jia, P.; Su, L.; Zhao, H.; Que, C. Outcomes and prognostic factors of non-HIV patients with pneumocystis jirovecii pneumonia and pulmonary CMV co-infection: A Retrospective Cohort Study. BMC Infect. Dis. 2017, 17, 392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korkmaz Ekren, P.; Toreyin, Z.N.; Nahid, P.; Doskaya, M.; Caner, A.; Turgay, N.; Zeytinoglu, A.; Toz, S.; Bacakoglu, F.; Guruz, Y.; et al. The association between Cytomegalovirus co-infection with Pneumocystis pneumonia and mortality in immunocompromised non-HIV patients. Clin. Respir. J. 2018, 12, 2590–2597. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.R.; Kim, J.M.; Kang, J.M.; Kim, Y.J. Pneumocystis jirovecii pneumonia in pediatric patients: An analysis of 15 confirmed consecutive cases during 14 years. Korean J. Pediatr. 2016, 59, 252–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.Y.; Lu, C.Y.; Lee, P.I.; Chen, J.M.; Huang, L.M.; Chang, L.Y. Pneumocystis jiroveci pneumonia in Taiwan from 2014 to 2017: Clinical manifestations and outcomes between pediatric and adult patients. J. Microbiol. Immunol. Infect. 2019, 52, 983–990. [Google Scholar] [CrossRef] [PubMed]
- Roblot, F.; Godet, C.; Le Moal, G.; Garo, B.; Souala, M.F.; Dary, M.; de Gentile, L.; Gandji, J.A.; Guimard, Y.; Lacroix, C.; et al. Analysis of underlying diseases and prognosis factors associated with Pneumocystis carinii pneumonia in immunocompromised HIV-negative patients. Eur. J. Clin. Microbiol. Infect. Dis. 2002, 21, 523–531. [Google Scholar] [PubMed]
- Kim, S.J.; Lee, J.; Cho, Y.J.; Park, Y.S.; Lee, C.H.; Yoon, H.I.; Lee, S.M.; Yim, J.J.; Lee, J.H.; Yoo, C.G.; et al. Prognostic factors of Pneumocystis jirovecii pneumonia in patients without HIV infection. J. Infect. 2014, 69, 88–95. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Proven PCP (n = 14) | mp-PCP (n = 65) | Non-PCP (n = 31) | p-Value | ||
|---|---|---|---|---|---|
| Age (y) | Median (IQR) | 5.5 (1.4–11.1) | 7.4 (2.4–12.8) | 4.7 (0.9–12.0) | 0.173 |
| <5 YO | 6 (42.9) | 22 (33.8) | 17 (54.8) | 0.146 | |
| Sex | Female | 6 (42.9) | 31 (47.7) | 17 (54.8) | 0.712 |
| Underlying medical condition | HSCT | 3 (21.4) | 13 (20.0) | 4 (12.9) | 0.662 |
| SOT | 2 (14.3) | 16 (24.6) | 1 (3.2) | 0.033 * | |
| HM | 2 (14.3) | 15 (23.1) | 3 (9.7) | 0.260 | |
| SC | 2 (14.3) | 7 (10.8) | 4 (12.9) | 0.911 | |
| PID | 1 (7.1) | 7 (10.8) | 8 (25.8) | 0.104 | |
| None | 1 (7.1) | 1 (1.5) | 3 (9.7) | 0.178 | |
| Symptom/sign | Fever | 13 (92.9) | 50 (76.9) | 18 (58.1) | 0.026 * |
| Cough | 9 (64.3) | 49 (75.4) | 19 (61.3) | 0.437 | |
| Sputum | 7 (50.0) | 31 (47.7) | 11 (35.5) | 0.527 | |
| Tachypnea | 8 (57.1) | 43 (66.2) | 8 (25.8) | 0.002 * | |
| Dyspnea | 9 (64.3) | 54 (83.1) | 15 (48.4) | 0.004 * | |
| Desaturation | 11(78.6) | 52 (80.0) | 15 (48.4) | 0.006 * | |
| Breath sound | Rale | 4 (28.6) | 19 (29.2) | 11 (35.5) | 0.746 |
| Wheezing | 0 (0.0) | 4 (6.2) | 9 (29.0) | 0.318 | |
| Respiratory pathogen co-detected | CMV culture | 2 (14.3) | 8 (12.3) | 2 (6.5) | 0.695 |
| Virus RT-PCR | 5 (35.7) | 23 (35.4) | 13 (41.9) | 0.638 | |
| Bacterial culture | 1 (7.1) | 15 (23.1) | 11 (35.5) | 0.103 | |
| C-CT findings | Bilateral GGO | 13 (92.9) | 48 (73.8) | 6 (19.4) | <0.001 * |
| Pleural effusion | 2 (14.3) | 5 (7.7) | 3 (9.7) | 0.675 | |
| Onset | Hospital onset | 7 (50.0) | 24 (36.9) | 14 (45.2) | 0.566 |
| PCP Px | Yes | 4 (28.6) | 19 (29.2) | 7 (22.6) | 0.786 |
| PMD | 3 (21.4) | 8 (12.3) | 3 (9.7) | 0.475 | |
| PCP Tx | Yes | 14 (100.0) | 59 (90.8) | 13 (41.9) | <0.001 * |
| TMP/SMX only | 8 (57.1) | 48 (73.8) | 11 (35.5) | 0.119 | |
| TMP/SMX + PMD | 6 (42.9) | 11 (16.9) | 1 (3.2) | 0.060 | |
| Outcome | Death | 6 (42.9) | 18 (27.7) | 8 (25.8) | 0.470 |
| Death (n = 24) | Survival (n = 55) | p-Value | ||
|---|---|---|---|---|
| Age (y) | <5 YO | 13 (54.2) | 15 (27.3) | 0.022 * |
| Sex | Female | 9 (37.5) | 28 (50.9) | 0.272 |
| Underlying medical condition | HCT | 9 (37.5) | 7 (12.7) | 0.012 * |
| SOT | 2 (8.3) | 16 (29.1) | 0.047 * | |
| HM | 5 (20.8) | 12 (21.8) | 1.000 | |
| SC | 3 (12.5) | 6 (10.9) | 1.000 | |
| PID | 2 (8.3) | 6 (10.9) | 1.000 | |
| None | 2 (8.3) | 0 (0.0) | 0.900 | |
| Symptom/sign | Fever | 20 (83.3) | 43 (78.2) | 0.532 |
| Cough | 15 (62.5) | 43 (78.2) | 0.536 | |
| Sputum | 10 (41.7) | 28 (50.9) | 0.549 | |
| Tachypnea | 14 (58.3) | 37 (67.3) | 0.776 | |
| Dyspnea | 19 (79.2) | 44 (80.0) | 0.496 | |
| Desaturation | 22 (91.7) | 41 (74.5) | 0.055 | |
| Breath sound | Rale | 9 (37.5) | 14 (25.5) | 0.197 |
| Wheezing | 3 (12.5) | 6 (10.9) | 0.713 | |
| Respiratory pathogenco-detected | CMV culture | 1 (4.2) | 9 (16.4) | 0.143 |
| Virus RT-PCR | 8 (33.3) | 20 (36.4) | 0.781 | |
| Bacterial culture | 7 (29.2) | 9 (16.4) | 0.291 | |
| C-CT findings | Bilateral GGO | 14 (58.3) | 47 (85.5) | 0.087 |
| Pleural effusion | 4 (16.7) | 3 (5.5) | 0.080 | |
| Onset | Hospital onset | 15 (62.5) | 16 (29.1) | 0.005 * |
| PCP prophylaxis | Yes | 13 (54.2) | 10 (18.2) | 0.001 * |
| PMD | 5 (20.8) | 6 (10.9) | 0.414 | |
| PCP treatment | Yes | 20 (83.3) | 53 (96.4) | 0.066 |
| TMP/SMX only | 11 (45.8) | 45 (81.8) | 0.007 * | |
| TMP/SMX + PMD | 9 (37.5) | 8 (14.5) | 0.007 * |
| Death (n = 24) | Survival (n = 55) | OR | 95% CI | ||
|---|---|---|---|---|---|
| Age (y) | <5 YO | 13 (54.2) | 15 (27.3) | 10.660 * | 1.816–62.570 |
| Underlying condition | HSCT | 9 (37.5) | 7 (12.7) | 5.861 | 0.755–45.524 |
| Onset | Hospital | 15 (62.5) | 16 (29.1) | 6.941 * | 1.491–32.308 |
| Symptom/sign | Desaturation | 22 (91.7) | 41 (74.5) | 63.547 * | 2.454–1645.517 |
| C-CT finding | Bilateral GGO | 14 (58.3) | 47 (85.5) | 0.976 | 0.149–6.406 |
| Pleural effusion | 4 (16.7) | 3 (5.5) | 8.026 | 0.754–85.413 | |
| PCP prophylaxis | Yes | 13 (54.2) | 10 (18.2) | 5.294 | 0.770–36.386 |
| PCP treatment | TMP/SMX + PMD | 9 (37.5) | 8 (14.5) | 3.472 | 0.687–17.533 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yun, K.S.; Anh, B.; Choi, S.H.; Hong, K.T.; Choi, J.Y.; Yun, K.W.; Kang, H.J.; Choi, E.H. Clinical Characteristics and Prognosis of the Modified Probable Pneumocystis jirovecii Pneumonia in Korean Children, 2001–2021. Children 2022, 9, 1596. https://doi.org/10.3390/children9101596
Yun KS, Anh B, Choi SH, Hong KT, Choi JY, Yun KW, Kang HJ, Choi EH. Clinical Characteristics and Prognosis of the Modified Probable Pneumocystis jirovecii Pneumonia in Korean Children, 2001–2021. Children. 2022; 9(10):1596. https://doi.org/10.3390/children9101596
Chicago/Turabian StyleYun, Kyoung Sung, Bin Anh, Sung Hwan Choi, Kyung Taek Hong, Jung Yoon Choi, Ki Wook Yun, Hyoung Jin Kang, and Eun Hwa Choi. 2022. "Clinical Characteristics and Prognosis of the Modified Probable Pneumocystis jirovecii Pneumonia in Korean Children, 2001–2021" Children 9, no. 10: 1596. https://doi.org/10.3390/children9101596