
Prevalence, Risk Factors, Prognosis, and Management of Pericardial Effusion in COVID-19
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
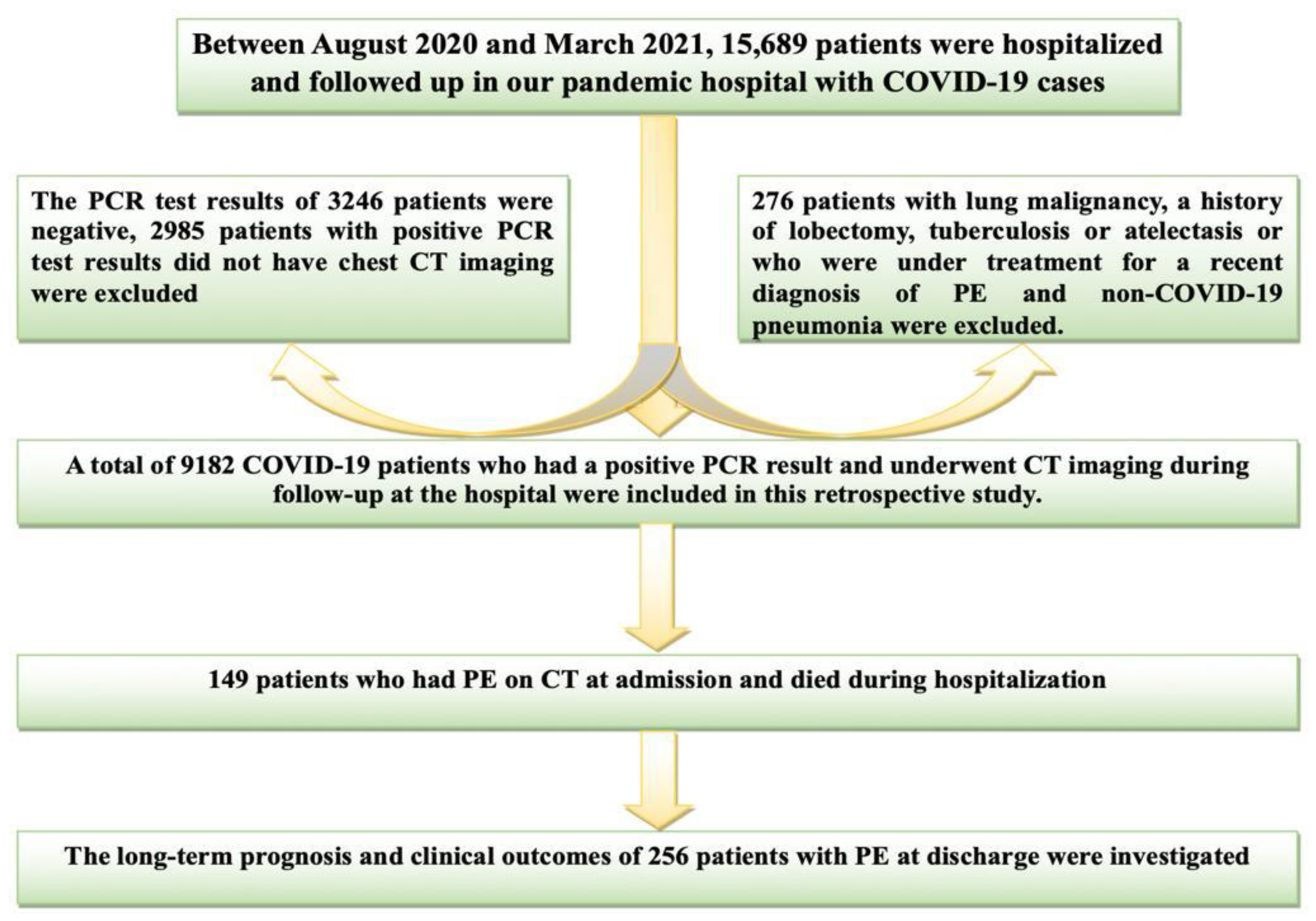
2.1. Study Population
2.2. The Treatment and Management of the Patient
2.3. Pericardial Effusion (CT and TTE)
2.4. Pulmonary Involvement and Total Severity Score
2.5. Chest CT Scan
2.6. Statistical Analysis
3. Result
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ochani, R.; Asad, A.; Yasmin, F.; Shaikh, S.; Khalid, H.; Batra, S.; Sohail, M.R.; Mahmood, S.F.; Ochani, R.; Hussham Arshad, M. COVID-19 pandemic: From origins to outcomes. A comprehensive review of viral pathogenesis, clinical manifestations, diagnostic evaluation, and management. Infez. Med. 2021, 29, 20–36. [Google Scholar] [PubMed]
- El-Shabasy, R.M.; Nayel, M.A.; Taher, M.M.; Abdelmonem, R.; Shoueir, K.R. Three waves changes, new variant strains, and vaccination effect against COVID-19 pandemic. Int. J. Biol. Macromol. 2022, 204, 161–168. [Google Scholar]
- Elrobaa, I.H.; New, K.J. COVID-19: Pulmonary and extra pulmonary manifestations. Front. Public Health 2021, 9, 711616. [Google Scholar]
- Kermani-Alghoraishi, M.; Pouramini, A.; Kafi, F.; Khosravi, A. Coronavirus disease 2019 (COVID-19) and severe pericardial effusion: From pathogenesis to management: A case report based systematic review. Curr. Probl. Cardiol. 2022, 47, 100933. [Google Scholar] [CrossRef]
- Saraç, İ.; Tonkaz, G.; Aksakal, E.; Aydinyilmaz, F.; Alisar, K.; Aydin, S.S.; Aydemir, S.; Dogan, R.; Gülcü, O.; Kalkan, K. The relationship between pericardial effusion and pulmonary involvement, prognosis, mortality in COVID-19 patients. Kardiologiia 2022, 62, 67–73. [Google Scholar] [CrossRef]
- Cobilinschi, C.; Melente, O.M.; Bologa, C.; Cotae, A.-M.; Constantinescu, L.; Bacruban, S.; Grinţescu, I.M. Cardiac tamponade—An unexpected “long COVID-19” complication. Germs 2022, 12, 112. [Google Scholar] [CrossRef]
- Adler, Y.; Charron, P.; Imazio, M.; Badano, L.; Barón-Esquivias, G.; Bogaert, J.; Brucato, A.; Gueret, P.; Klingel, K.; Lionis, C. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Kardiol. Pol. 2015, 73, 1028–1091. [Google Scholar] [CrossRef]
- Artika, I.M.; Dewi, Y.P.; Nainggolan, I.M.; Siregar, J.E.; Antonjaya, U. Real-time polymerase chain reaction: Current techniques, applications, and role in COVID-19 diagnosis. Genes 2022, 13, 2387. [Google Scholar] [PubMed]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.-J.; Martin, I.B. The role of chest imaging in patient management during the COVID-19 pandemic: A multinational consensus statement from the Fleischner Society. Radiology 2020, 296, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Bakanliği, T.C. COVID-19 (SARS-CoV-2 Enfeksiyonu) Genel Bilgiler, Epidemiyoloji Ve Tani: 2020, Ankara, Turkey. Available online: https://covid19.saglik.gov.tr/Eklenti/39551/0/covid-19rehberigenelbilgilerepidemiyolojivetanipdf.pdf (accessed on 3 June 2023).
- Bakanlığı, T.S. Halk Sağlığı Genel Müdürlüğü, COVİD-19 (SARS-CoV-2) Rehberi (Bilim Kurulu Çalışması). 2020, Ankara, Turkey. Available online: https://covid19.saglik.gov.tr/Eklenti/39296/0/covid-19rehberiantisitokin-antiinflamatuartedavilerkoagulopatiyonetimipdf.pdf (accessed on 3 June 2023).
- Imazio, M.; Brucato, A.; Lazaros, G.; Andreis, A.; Scarsi, M.; Klein, A.; De Ferrari, G.M.; Adler, Y. Anti-inflammatory therapies for pericardial diseases in the COVID-19 pandemic: Safety and potentiality. J. Cardiovasc. Med. 2020, 21, 625–629. [Google Scholar] [CrossRef]
- Kirkpatrick, J.N.; Mitchell, C.; Taub, C.; Kort, S.; Hung, J.; Swaminathan, M. ASE statement on protection of patients and echocardiography service providers during the 2019 novel coronavirus outbreak: Endorsed by the American College of Cardiology. J. Am. Coll. Cardiol. 2020, 75, 3078–3084. [Google Scholar] [CrossRef] [PubMed]
- Ovchinnikov, V. Computerized tomography of pericardial diseases. Vestn. Rentgenol. Radiol. 1996, 1, 10–15. [Google Scholar]
- Lazaros, G.; Vlachopoulos, C.; Lazarou, E.; Tsioufis, K. New approaches to management of pericardial effusions. Curr. Cardiol. Rep. 2021, 23, 106. [Google Scholar] [CrossRef]
- Li, K.; Fang, Y.; Li, W.; Pan, C.; Qin, P.; Zhong, Y.; Liu, X.; Huang, M.; Liao, Y.; Li, S. CT image visual quantitative evaluation and clinical classification of coronavirus disease (COVID-19). Eur. Radiol. 2020, 30, 4407–4416. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.-T.; Toh, H.S.; Liao, C.-T.; Yu, W.-L. Cardiac involvement of COVID-19: A comprehensive review. Am. J. Med. Sci. 2021, 361, 14–22. [Google Scholar] [PubMed]
- Al-Tarbsheh, A.H.; Leamon, A.; Chong, W.H.; Chung, J.K.; Oweis, J.; Vamshek, S.; Dawani, O.; Chopra, A. Pericardial effusion in COVID-19 patients. Am. J. Med. Sci. 2022, 364, 129–130. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M. Outcomes of cardiovascular magnetic resonance imaging in patients recently recovered from coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265–1273. [Google Scholar] [CrossRef]
- Izzo, C.; Visco, V.; Gambardella, J.; Ferruzzi, G.J.; Rispoli, A.; Rusciano, M.R.; Toni, A.L.; Virtuoso, N.; Carrizzo, A.; Di Pietro, P. Cardiovascular implications of microRNAs in coronavirus disease 2019. J. Pharmacol. Exp. Ther. 2023, 384, 102–108. [Google Scholar] [CrossRef]
- Kotecha, T.; Knight, D.S.; Razvi, Y.; Kumar, K.; Vimalesvaran, K.; Thornton, G.; Patel, R.; Chacko, L.; Brown, J.T.; Coyle, C. Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance. Eur. Heart J. 2021, 42, 1866–1878. [Google Scholar]
- Mitrani, R.D.; Dabas, N.; Alfadhli, J.; Lowery, M.H.; Best, T.M.; Hare, J.M.; Myerburg, R.J.; Goldberger, J.J. Long-term cardiac surveillance and outcomes of COVID-19 patients. Trends Cardiovasc. Med. 2022, 32, 465–475. [Google Scholar]
- Sauer, F.; Dagrenat, C.; Couppie, P.; Jochum, G.; Leddet, P. Pericardial effusion in patients with COVID-19: Case series. Eur. Heart J. Case Rep. 2020, 4, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.Z.; Kumar, S.A.; Patel, A.A. Myocarditis and pericarditis in patients with COVID-19. Heart Views Off. J. Gulf Heart Assoc. 2020, 21, 209. [Google Scholar]
- Imazio, M.; Spodick, D.H.; Brucato, A.; Trinchero, R.; Adler, Y. Controversial issues in the management of pericardial diseases. Circulation 2010, 121, 916–928. [Google Scholar] [CrossRef] [PubMed]
- Carubbi, F.; Alunno, A.; Leone, S.; Di Gregorio, N.; Mancini, B.; Viscido, A.; Del Pinto, R.; Cicogna, S.; Grassi, D.; Ferri, C. Pericarditis after SARS-CoV-2 infection: Another pebble in the mosaic of long COVID? Viruses 2021, 13, 1997. [Google Scholar] [CrossRef]
- Sagristà-Sauleda, J.; Angel, J.; Permanyer-Miralda, G.; Soler-Soler, J. Long-term follow-up of idiopathic chronic pericardial effusion. N. Engl. J. Med. 1999, 341, 2054–2059. [Google Scholar] [CrossRef] [PubMed]
- Lazaros, G.; Antonopoulos, A.S.; Lazarou, E.; Vlachopoulos, C.; Foukarakis, E.; Androulakis, A.; Manginas, A.; Theodoros, K.; Karavidas, A.; Tousoulis, D. Long-term outcome of pericardial drainage in cases of chronic, large, hemodynamically insignificant, C-reactive protein negative, idiopathic pericardial effusions. Am. J. Cardiol. 2020, 126, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Imazio, M.; Lazaros, G.; Valenti, A.; De Carlini, C.C.; Maggiolini, S.; Pivetta, E.; Giustetto, C.; Tousoulis, D.; Adler, Y.; Rinaldi, M. Outcomes of idiopathic chronic large pericardial effusion. Heart 2019, 105, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Imazio, M.; Cecchi, E.; Demichelis, B.; Ierna, S.; Demarie, D.; Ghisio, A.; Pomari, F.; Coda, L.; Belli, R.; Trinchero, R. Indicators of poor prognosis of acute pericarditis. Circulation 2007, 115, 2739–2744. [Google Scholar] [CrossRef]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.-J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef]
- Graña, C.; Ghosn, L.; Evrenoglou, T.; Jarde, A.; Minozzi, S.; Bergman, H.; Buckley, B.S.; Probyn, K.; Villanueva, G.; Henschke, N.; et al. Efficacy and safety of COVID-19 vaccines. Cochrane Database Syst. Rev. 2022, 12, CD015477. [Google Scholar] [CrossRef]
- Lazaros, G.; Lazarou, E.; Tsioufis, P.; Soulaidopoulos, S.; Iliakis, P.; Vlachopoulos, C.; Tsioufis, C. Chronic pericardial effusion: Current concepts and emerging trends. Expert Rev. Cardiovasc. Ther. 2022, 20, 363–376. [Google Scholar] [CrossRef] [PubMed]
- Blanco, J.-R.; Cobos-Ceballos, M.-J.; Navarro, F.; Sanjoaquin, I.; de Las Revillas, F.A.; Bernal, E.; Buzon-Martin, L.; Viribay, M.; Romero, L.; Espejo-Perez, S. Pulmonary long-term consequences of COVID-19 infections after hospital discharge. Clin. Microbiol. Infect. 2021, 27, 892–896. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| PE in CT (Group): MILD:0, MODERATE:1, LARGE:2 | p Value | Posthoc | ||||||
|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | ||||||
| N | Mean ± SD | N | Mean ± SD | N | Mean ± SD | |||
| TSS | 137 | 6.42 ± 5.03 | 78 | 9.53 ± 4.49 | 41 | 14.63 ± 3.34 | 0.000 | ALL |
| Age (years) | 137 | 62.17 ± 16.34 | 78 | 69.12 ± 12.52 | 41 | 72.44 ± 15.26 | 0.000 | ALL |
| CHA2DS2VASCs | 137 | 2.12 ± 1.69 | 78 | 3.13 ± 1.72 | 41 | 4.51 ± 2.04 | 0.000 | ALL |
| Duration of Hospitalizations/days | 137 | 8.69 ± 5.084 | 78 | 13.23 ± 6.877 | 41 | 20.93 ± 16.015 | 0.000 | ALL |
| Albumin (g/dL) | 129 | 44.88 ± 5.20 | 72 | 41.30 ± 7.17 | 34 | 39.78 ± 5.51 | 0.000 | 0–1, 0–2 |
| Creatinine (mg/dL) | 115 | 88.17 ± 29.38 | 65 | 81.59 ± 45.37 | 34 | 74.23 ± 38.39 | 0.029 | 0–1 |
| CRP (mg/L) | 137 | 17.77 ± 29.18 | 78 | 45.20 ± 56.64 | 41 | 80.81 ± 80.60 | 0.000 | ALL |
| Troponin I (ng/mL) | 137 | 0.22 ± 0.39 | 78 | 1.30 ± 2.37 | 41 | 2.38 ± 7.75 | 0.000 | 0–1, 0–2 |
| SO2 (pulse oximeter,%) | 137 | 84.68 ± 6.14 | 78 | 81.72 ± 8.54 | 41 | 76.78 ± 8.74 | 0.000 | ALL |
| Hb (g/dL) | 132 | 14.18 ± 2.04 | 77 | 13.75 ± 2.17 | 36 | 13.14 ± 2.02 | 0.041 | 0–2 |
| Lymphocyte count (103/μL) | 126 | 1.80 ± 1.83 | 77 | 1.08 ± 0.45 | 36 | 0.83 ± 0.29 | 0.000 | ALL |
| Ferritin (ng/mL) | 137 | 408.45 ± 583.93 | 78 | 588.67 ± 983.52 | 41 | 889.59 ± 1470.30 | 0.033 | 0–2 |
| D-dimer (μg/mL) | 137 | 728.96 ± 602.37 | 78 | 1810.94 ± 2269.93 | 39 | 2243.38 ± 4187.28 | 0.000 | 0–1, 0–2 |
| Wbc (103/μL) | 132 | 7.40 ± 3.42 | 77 | 10.66 ± 5.26 | 37 | 12.89 ± 7.23 | 0.000 | 0–1, 0–2 |
| Platelet count (103/μL) | 132 | 126.12 ± 83.06 | 78 | 118.71 ± 67.11 | 36 | 112.50 ± 94.57 | 0.340 | |
| Average long-term follow-up (month) | 137 | 25.28 ± 4.56 | 78 | 25.94 ± 4.62 | 41 | 23.49 ± 7.34 | ||
| Mean 3rd-month LVEF | 128 | 54.87 ± 4.68 | 71 | 52.56 ± 7.34 | 36 | 50.73 ± 9.63 | 0.000 | 0–1, 0–2 |
| Long-term mean LVEF | 119 | 54.76 ± 5.16 | 59 | 52.19 ± 7.77 | 23 | 48.11 ± 10.43 | 0.000 | 0–1, 0–2 |
| PE in CT (Group): MILD:0, MODERATE:1, LARGE:2 | p Value | |||
|---|---|---|---|---|
| 0 N: 137 | 1 N: 78 | 2 N: 41 | ||
| N % | N % | N % | ||
| Need for ICU, n (%) | 9 (6.57%) | 22 (28.21%) | 32 (78.05%) | <0.001 |
| MABs, n (%) | 1 (0.73%) | 1 (1.28%) | 5 (12.20%) | 0.002 |
| Pulse Steroid, n (%) | 6 (4.38%) | 5 (6.41%) | 10 (24.39%) | 0.001 |
| Gender/Male, n (%) | 76 (55.47%) | 45 (57.69%) | 25 (60.98%) | 0.817 |
| DM, n (%) | 26 (18.98%) | 26 (33.33%) | 21 (51.22%) | <0.001 |
| HT, n (%) | 52 (37.96%) | 51 (65.38%) | 28 (68.29%) | <0.001 |
| CAD, n (%) | 19 (13.87%) | 22 (28.21%) | 23 (56.10%) | <0.001 |
| HF, n (%) | 8 (5.84%) | 14 (17.95%) | 18 (43.90%) | <0.001 |
| COPD, n (%) | 21 (15.33%) | 17 (21.79%) | 20 (48.78%) | <0.001 |
| CVD, n (%) | 3 (2.19%) | 5 (6.41%) | 6 (14.63%) | 0.008 |
| AF, n (%) | 16 (11.68%) | 13 (16.67%) | 11 (26.83%) | 0.063 |
| CRF, n (%) | 11 (8.03%) | 15 (19.23%) | 12 (29.27%) | 0.001 |
| PAD, n (%) | 8 (5.84%) | 4 (5.13%) | 4 (9.76%) | 0.568 |
| ASA, n (%) | 20 (14.60%) | 23 (29.49%) | 17 (41.46%) | 0.001 |
| Statin, n (%) | 13 (9.49%) | 11 (14.10%) | 14 (34.15%) | 0.001 |
| Clopidogrel, n (%) | 4 (2.92%) | 8 (10.26%) | 8 (19.51%) | 0.001 |
| BB, n (%) | 35 (25.55%) | 32 (41.03%) | 28 (68.29%) | <0.001 |
| Furosemide, n (%) | 7 (5.11%) | 11 (14.10%) | 12 (29.27%) | <0.001 |
| CCB, n (%) | 9 (6.57%) | 16 (20.51%) | 6 (14.63%) | 0.007 |
| ACEI-ARB | 42 (30.66%) | 40 (51.28%) | 24 (58.54%) | 0.001 |
| Spirinolactone, n (%) | 4 (2.94%) | 8 (10.26%) | 9 (21.95%) | <0.001 |
| OAC, n (%) | 9 (6.57%) | 10 (12.82%) | 7 (17.07%) | 0.08 |
| non-medicated, n (%) | 68 (49.64%) | 11 (14.10%) | 6 (14.63%) | <0.001 |
| PE Size | Medications at Admission or Discharge | PE Size at Mean 3rd Month | p Value | ||||
|---|---|---|---|---|---|---|---|
| Mild/n | Moderate/n | Large/n | No PE/n | ||||
| Mild | NSAIDs/n | 49 | 23 | 2 | 1 | 23 | 0.209 |
| Colchıum + Steroid/n | 15 | 6 | 2 | 1 | 6 | ||
| Only Steroid/n | 65 | 20 | 7 | 0 | 38 | ||
| Moderate | NSAIDs/n | 15 | 6 | 9 | 0 | 0 | 0.104 |
| Colchıum + Steroid/n | 23 | 10 | 6 | 1 | 6 | ||
| Only Steroid/n | 40 | 19 | 18 | 0 | 3 | ||
| Large | NSAIDs/n | 5 | 0 | 3 | 2 | 0 | 0.368 |
| Colchıum + Steroid/n | 29 | 0 | 10 | 19 | 0 | ||
| Only Steroid/n | 7 | 0 | 4 | 3 | 0 | ||
| Hospitalization | PE in CT (Group): MILD:0, MODERATE:1, LARGE:2 | p Value | |||
|---|---|---|---|---|---|
| 0 | 1 | 2 | |||
| N % | N % | N % | |||
| Cardiac etiology | No Hospitalization | 113 (82.48%) | 47 (60.26%) | 8 (19.51%) | NA |
| AF | 10 (7.30%) | 10 (12.82%) | 9 (21.95%) | ||
| HF | 5 (3.65%) | 11 (14.10%) | 10 (24.39%) | ||
| ACS | 7 (5.11%) | 8 (10.26%) | 8 (19.51%) | ||
| Other | 2 (1.46%) | 2 (2.56%) | 6 (14.64%) | ||
| Noncardiac etiology | No Hospitalization | 109 (79.56%) | 50 (64.10%) | 9 (21.95%) | <0.001 |
| Pneumonia, RF | 17 (12.41%) | 21 (26.92%) | 25(60.98%) | ||
| Other | 11 (8.03%) | 7 (8.97%) | 7 (17.07%) | ||
| A patient who has received at least two doses of the vaccıne | 89 (64.96%) | 50 (64.10%) | 24 (58.54%) | 0.756 | |
| Inactivated vaccines | 53 (38.69%) | 33 (42.31%) | 20 (48.78%) | 0.509 | |
| mRNA-based vaccine | 60 (43.80%) | 29 (37.18%) | 8 (19.51%) | 0.019 | |
| Tamponade | 1 (0.07%) | 3(3.84%) | 5 (12.19%) | 0.001 | |
| Cardiac Mortality. | 3 (2.19%) | 6 (7.69%) | 9 (21.95%) | <0.001 | |
| Noncardiac Mortality | 5 (3.65%) | 7 (8.97%) | 7 (17.07%) | 0.014 | |
| Total Mortality | 8 (5.84%) | 13 (16.67%) | 16 (39.02%) | <0.001 | |
| Symptoms in Outpatient Clinic Controls | No Symptoms | 33 (24.09%) | 19 (24.68%) | 0 (0.00%) | NA |
| Palpitation | 18 (13.14%) | 6 (7.79%) | 4 (10.26%) | ||
| Dyspnea | 30 (21.90%) | 30 (38.96%) | 29 (74.36%) | ||
| Chest Pain | 38 (27.74%) | 21 (27.27%) | 6 (15.38%) | ||
| Other | 18 (13.14%) | 1 (1.30%) | 0 (0.00%) | ||
| Association of at least two doses of vaccination and mortality in patients who survived and died during the total follow-up | |||||
| Alive: 219 | Death: 37 | p Value | |||
| Inactivated vaccines/n (%) | 99 (45.2%) | 7 (18.9%) | 0.003 | ||
| mRNA-based vaccine/n (%) | 94 (42.9%) | 3 (8.1%) | 0.000 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saraç, İ.; Aydın, S.Ş.; Özmen, M.; Doru, H.İ.; Tonkaz, G.; Çırçır, M.N.; Akpınar, F.; Zengin, O.; Delice, O.; Aydınyılmaz, F. Prevalence, Risk Factors, Prognosis, and Management of Pericardial Effusion in COVID-19. J. Cardiovasc. Dev. Dis. 2023, 10, 368. https://doi.org/10.3390/jcdd10090368
Saraç İ, Aydın SŞ, Özmen M, Doru Hİ, Tonkaz G, Çırçır MN, Akpınar F, Zengin O, Delice O, Aydınyılmaz F. Prevalence, Risk Factors, Prognosis, and Management of Pericardial Effusion in COVID-19. Journal of Cardiovascular Development and Disease. 2023; 10(9):368. https://doi.org/10.3390/jcdd10090368
Chicago/Turabian StyleSaraç, İbrahim, Sidar Şiyar Aydın, Murat Özmen, Halil İbrahim Doru, Gökhan Tonkaz, Melike Nur Çırçır, Furkan Akpınar, Onur Zengin, Orhan Delice, and Faruk Aydınyılmaz. 2023. "Prevalence, Risk Factors, Prognosis, and Management of Pericardial Effusion in COVID-19" Journal of Cardiovascular Development and Disease 10, no. 9: 368. https://doi.org/10.3390/jcdd10090368