
Is It Possible to Differentiate Pneumocystis jirovecii Pneumonia and Colonization in the Immunocompromised Patients with Pneumonia?

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
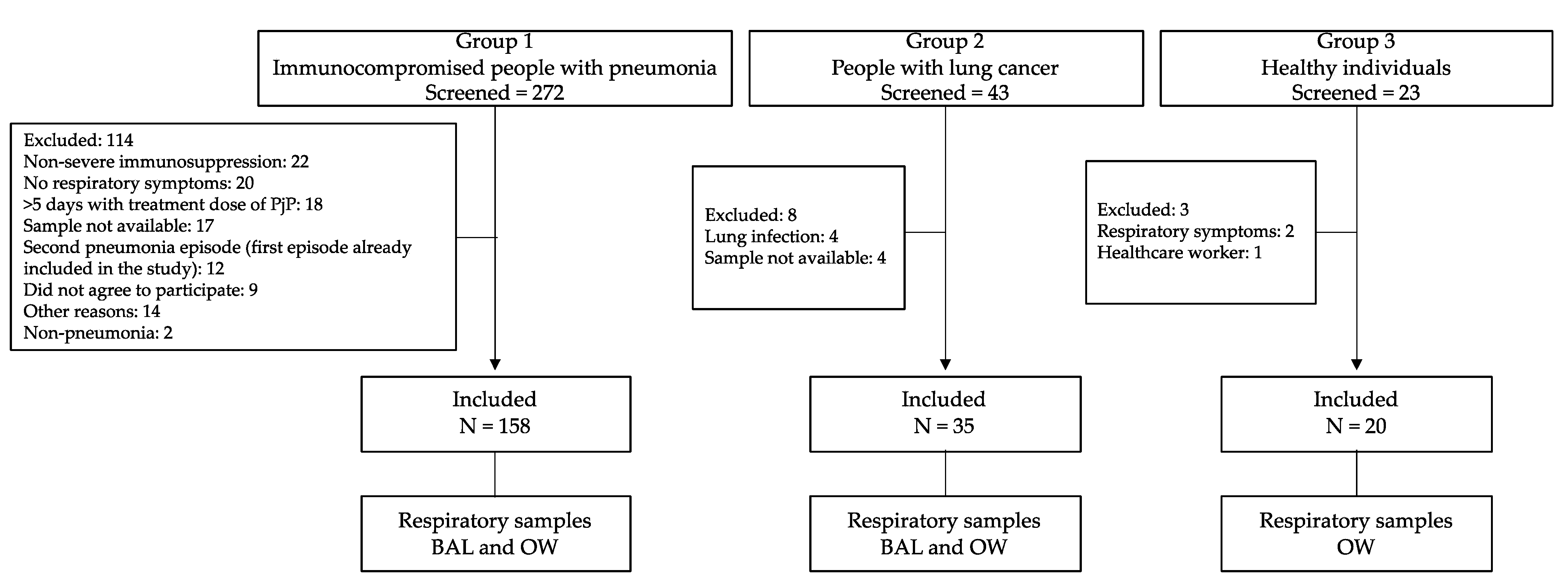
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
- Follow-up: Until discharge or death. During hospitalization, we recorded information on patient demographics, past clinical history, clinical information for the current episode, laboratory parameters, and the presence of mycobacteria, fungi, and pyogenic bacteria, in both BAL and blood samples. After hospitalization, each participant was followed up with at 6 and 12 months by phone call, to ask about new hospitalizations (date(s) and reason for hospitalization(s)), survival, antiretroviral treatment, and prophylaxis with TMS/SMX. We also reviewed the clinical chart to identify if the patient was hospitalized (date(s) and reason for hospitalization(s)) during the year of follow-up and the survival.
2.3. Setting
2.4. Collection of Respiratory Samples and Microscopy
2.5. Definitions
2.6. DNA Extraction Protocol
2.7. qPCR Assay
2.8. Sample Size and Study Population
2.9. Statistical Analysis
3. Results
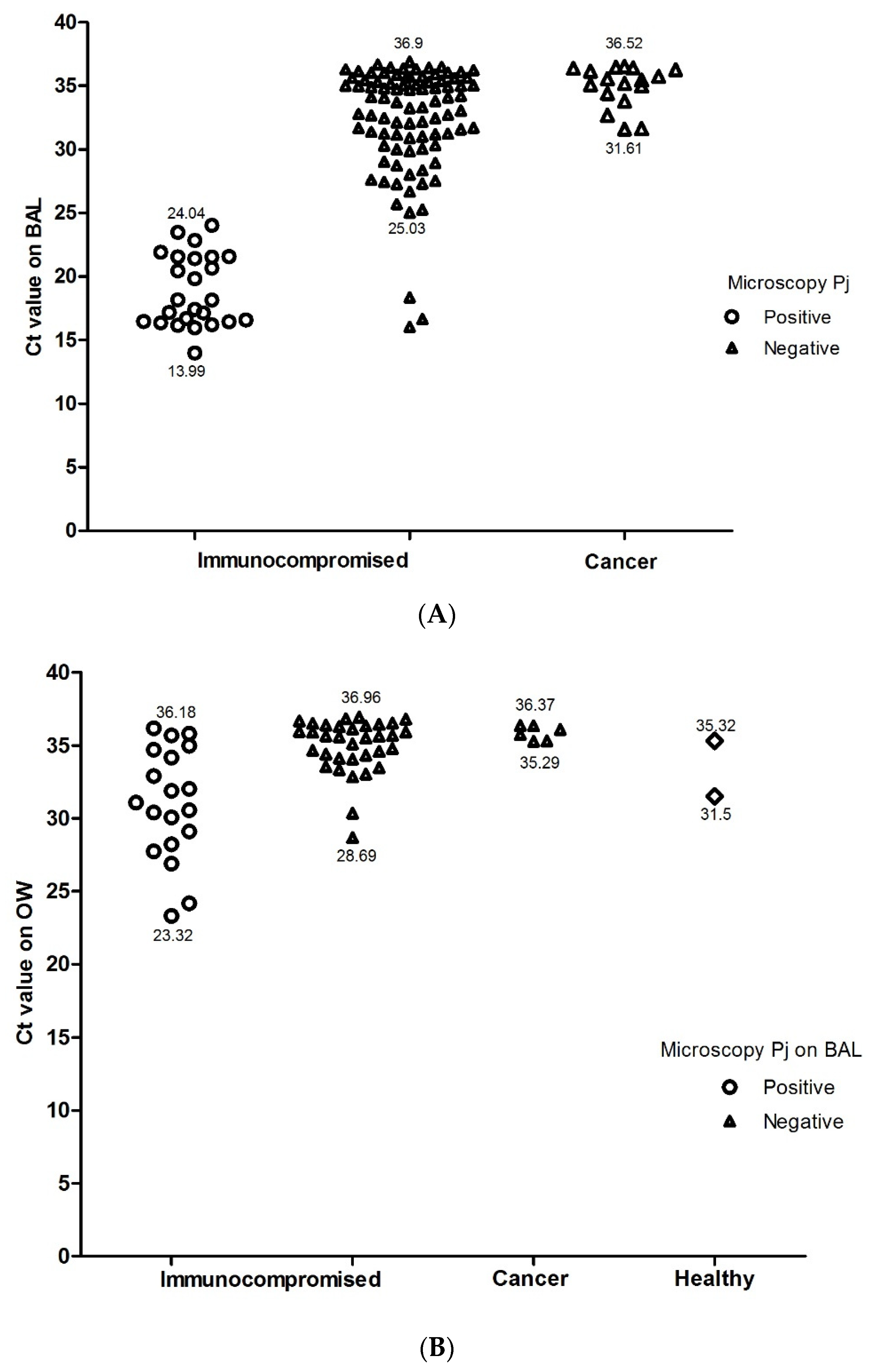
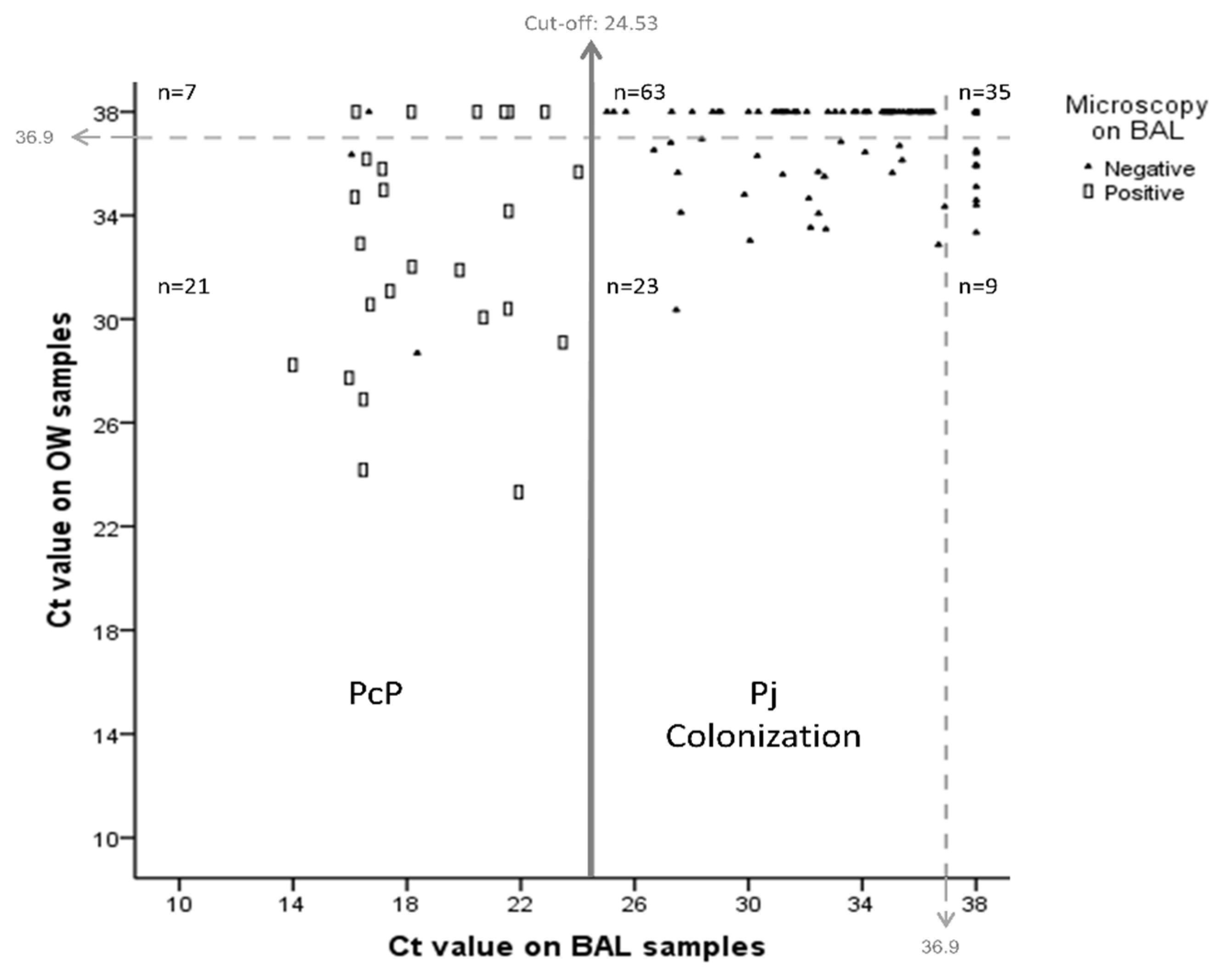
3.1. Diagnostic Validation of qPCR in BAL
3.2. Analysis of qPCR in OW Samples
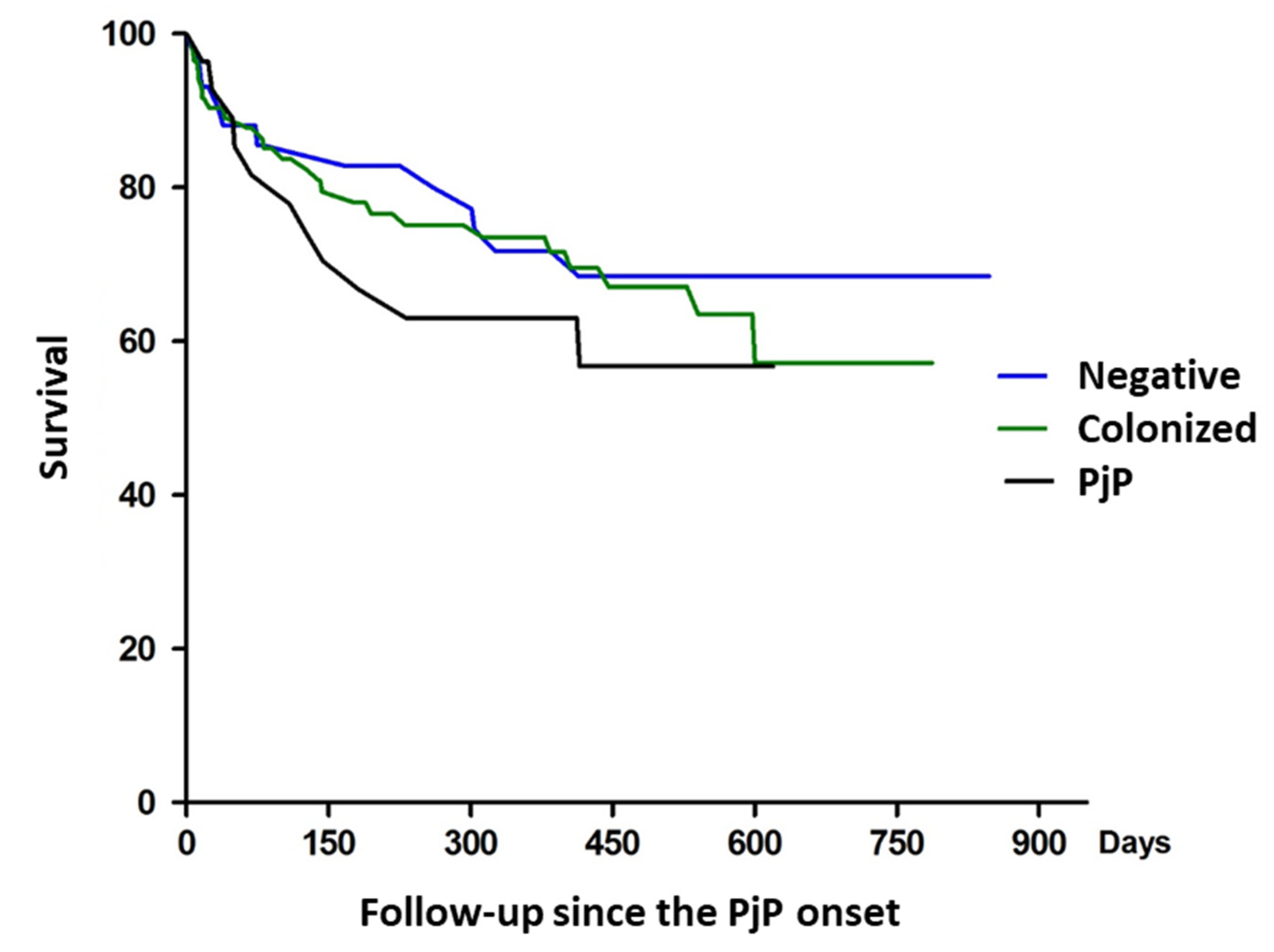
3.3. Clinical Characteristics and Follow-Up of Immunosuppressed Patients, Colonized and Non-Infected Individuals
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tellez, I.; Barragán, M.; Franco-Paredes, C.; Petraro, P.; Nelson, K.; Del Rio, C. Pneumocystis Jiroveci Pneumonia in Patients with AIDS in the Inner City: A Persistent and Deadly Opportunistic Infection. Am. J. Med. Sci. 2008, 335, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Sattler, F.R.; Cowan, R.; Nielsen, D.M.; Ruskin, J. Trimethoprim-Sulfamethoxazole Compared with Pentamidine for Treatment of Pneumocystis Carinii Pneumonia in the Acquired Immunodeficiency Syndrome. A Prospective, Noncrossover Study. Ann. Intern. Med. 1988, 109, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Rath, P.-M.; Steinmann, J. Update on Diagnosis of Pneumocystis Pulmonary Infections. Curr. Fungal Infect. Rep. 2014, 8, 227–234. [Google Scholar] [CrossRef]
- Larsen, H.H.; Masur, H.; Kovacs, J.A.; Gill, V.J.; Silcott, V.A.; Kogulan, P.; Maenza, J.; Smith, M.; Lucey, D.R.; Fischer, S.H. Development and Evaluation of a Quantitative, Touch-down, Real-Time PCR Assay for Diagnosing Pneumocystis Carinii Pneumonia. J. Clin. Microbiol. 2002, 40, 490–494. [Google Scholar] [CrossRef] [Green Version]
- Larsen, H.H.; Huang, L.; Kovacs, J.A.; Crothers, K.; Silcott, V.A.; Morris, A.; Turner, J.R.; Beard, C.B.; Masur, H.; Fischer, S.H. A Prospective, Blinded Study of Quantitative Touch-down Polymerase Chain Reaction Using Oral-Wash Samples for Diagnosis of Pneumocystis Pneumonia in HIV-Infected Patients. J. Infect. Dis. 2004, 189, 1679–1683. [Google Scholar] [CrossRef] [Green Version]
- Hviid, C.J.; Lund, M.; Sørensen, A.; Ellermann-Eriksen, S.; Jespersen, B.; Dam, M.Y.; Dahlerup, J.F.; Benfield, T.; Jespersen, S.; Østergaard, L.J.; et al. Detection of Pneumocystis Jirovecii in Oral Wash from Immunosuppressed Patients as a Diagnostic Tool. PLoS ONE 2017, 12, e0174012. [Google Scholar] [CrossRef] [Green Version]
- Sing, A.; Roggenkamp, A.; Autenrieth, I.B.; Heesemann, J. Pneumocystis Carinii Carriage in Immunocompetent Patients with Primary Pulmonary Disorders as Detected by Single or Nested PCR. J. Clin. Microbiol. 1999, 37, 3409–3410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maskell, N.A.; Waine, D.J.; Lindley, A.; Pepperell, J.C.T.; Wakefield, A.E.; Miller, R.F.; Davies, R.J.O. Asymptomatic Carriage of Pneumocystis Jiroveci in Subjects Undergoing Bronchoscopy: A Prospective Study. Thorax 2003, 58, 594–597. [Google Scholar] [CrossRef] [Green Version]
- Totet, A.; Meliani, L.; Lacube, P.; Pautard, J.C.; Raccurt, C.; Roux, P.; Nevez, G. Immunocompetent Infants as a Human Reservoir for Pneumocystis Jirovecii: Rapid Screening by Non-Invasive Sampling and Real-Time PCR at the Mitochondrial Large Subunit RRNA Gene. J. Eukaryot. Microbiol. 2003, 50, 668–669. [Google Scholar] [CrossRef]
- Qu, J.; Rong, Z.; He, L.; Pan, J.; Chen, X. Relationship between the Burden of Pneumocystis Carinii, the Inflammatory Reaction and Lung Injury in Pneumocystis Carinii Pneumonia. Chin. Med. J. 2000, 113, 1071–1074. [Google Scholar] [PubMed]
- Thomas, C.F.; Limper, A.H. Current Insights into the Biology and Pathogenesis of Pneumocystis Pneumonia. Nat. Rev. Microbiol. 2007, 5, 298–308. [Google Scholar] [CrossRef]
- Hoarau, G.; Le Gal, S.; Zunic, P.; Poubeau, P.; Antok, E.; Jaubert, J.; Nevez, G.; Picot, S. Evaluation of Quantitative FTD-Pneumocystis Jirovecii Kit for Pneumocystis Infection Diagnosis. Diagn. Microbiol. Infect. Dis. 2017, 89, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Moodley, B.; Tempia, S.; Frean, J.A. Comparison of Quantitative Real-Time PCR and Direct Immunofluorescence for the Detection of Pneumocystis Jirovecii. PLoS ONE 2017, 12, e0180589. [Google Scholar] [CrossRef]
- Unnewehr, M.; Friederichs, H.; Bartsch, P.; Schaaf, B. High Diagnostic Value of a New Real-Time Pneumocystis PCR from Bronchoalveolar Lavage in a Real-Life Clinical Setting. Respiration 2016, 92, 144–149. [Google Scholar] [CrossRef]
- Fauchier, T.; Hasseine, L.; Gari-Toussaint, M.; Casanova, V.; Marty, P.M.; Pomares, C. Detection of Pneumocystis Jirovecii by Quantitative PCR To Differentiate Colonization and Pneumonia in Immunocompromised HIV-Positive and HIV-Negative Patients. J. Clin. Microbiol. 2016, 54, 1487–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louis, M.; Guitard, J.; Jodar, M.; Ancelle, T.; Magne, D.; Lascols, O.; Hennequin, C. Impact of HIV Infection Status on Interpretation of Quantitative PCR for Detection of Pneumocystis Jirovecii. J. Clin. Microbiol. 2015, 53, 3870–3875. [Google Scholar] [CrossRef] [Green Version]
- Montesinos, I.; Brancart, F.; Schepers, K.; Jacobs, F.; Denis, O.; Delforge, M.-L. Comparison of 2 Real-Time PCR Assays for Diagnosis of Pneumocystis Jirovecii Pneumonia in Human Immunodeficiency Virus (HIV) and Non-HIV Immunocompromised Patients. Diagn. Microbiol. Infect. Dis. 2015, 82, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Robert-Gangneux, F.; Belaz, S.; Revest, M.; Tattevin, P.; Jouneau, S.; Decaux, O.; Chevrier, S.; Le Tulzo, Y.; Gangneux, J.-P. Diagnosis of Pneumocystis Jirovecii Pneumonia in Immunocompromised Patients by Real-Time PCR: A 4-Year Prospective Study. J. Clin. Microbiol. 2014, 52, 3370–3376. [Google Scholar] [CrossRef] [Green Version]
- Maillet, M.; Maubon, D.; Brion, J.P.; François, P.; Molina, L.; Stahl, J.P.; Epaulard, O.; Bosseray, A.; Pavese, P. Pneumocystis Jirovecii (Pj) Quantitative PCR to Differentiate Pj Pneumonia from Pj Colonization in Immunocompromised Patients. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 331–336. [Google Scholar] [CrossRef]
- Damiani, C.; Le Gal, S.; Da Costa, C.; Virmaux, M.; Nevez, G.; Totet, A. Combined Quantification of Pulmonary Pneumocystis Jirovecii DNA and Serum (1->3)-β-D-Glucan for Differential Diagnosis of Pneumocystis Pneumonia and Pneumocystis Colonization. J. Clin. Microbiol. 2013, 51, 3380–3388. [Google Scholar] [CrossRef] [Green Version]
- Matsumura, Y.; Ito, Y.; Iinuma, Y.; Yasuma, K.; Yamamoto, M.; Matsushima, A.; Nagao, M.; Takakura, S.; Ichiyama, S. Quantitative Real-Time PCR and the (1→3)-β-D-Glucan Assay for Differentiation between Pneumocystis Jirovecii Pneumonia and Colonization. Clin. Microbiol. Infect. 2012, 18, 591–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mühlethaler, K.; Bögli-Stuber, K.; Wasmer, S.; von Garnier, C.; Dumont, P.; Rauch, A.; Mühlemann, K.; Garzoni, C. Quantitative PCR to Diagnose Pneumocystis Pneumonia in Immunocompromised Non-HIV Patients. Eur. Respir. J. 2012, 39, 971–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alanio, A.; Desoubeaux, G.; Sarfati, C.; Hamane, S.; Bergeron, A.; Azoulay, E.; Molina, J.M.; Derouin, F.; Menotti, J. Real-Time PCR Assay-Based Strategy for Differentiation between Active Pneumocystis Jirovecii Pneumonia and Colonization in Immunocompromised Patients. Clin. Microbiol. Infect. 2011, 17, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Fillaux, J.; Malvy, S.; Alvarez, M.; Fabre, R.; Cassaing, S.; Marchou, B.; Linas, M.-D.; Berry, A. Accuracy of a Routine Real-Time PCR Assay for the Diagnosis of Pneumocystis Jirovecii Pneumonia. J. Microbiol. Methods 2008, 75, 258–261. [Google Scholar] [CrossRef]
- Flori, P.; Bellete, B.; Durand, F.; Raberin, H.; Cazorla, C.; Hafid, J.; Lucht, F.; Sung, R.T.M. Comparison between Real-Time PCR, Conventional PCR and Different Staining Techniques for Diagnosing Pneumocystis Jiroveci Pneumonia from Bronchoalveolar Lavage Specimens. J. Med. Microbiol. 2004, 53, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Church, D.L.; Ambasta, A.; Wilmer, A.; Williscroft, H.; Ritchie, G.; Pillai, D.R.; Champagne, S.; Gregson, D.G. Development and Validation of a Pneumocystis Jirovecii Real-Time Polymerase Chain Reaction Assay for Diagnosis of Pneumocystis Pneumonia. Can. J. Infect. Dis. Med. Microbiol. 2015, 26, 263–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, A.; Wei, K.; Afshar, K.; Huang, L. Epidemiology and Clinical Significance of Pneumocystis Colonization. J. Infect. Dis. 2008, 197, 10–17. [Google Scholar] [CrossRef] [Green Version]
- De la Horra, C.; Varela, J.M.; Fernández-Alonso, J.; Medrano, F.J.; Respaldiza, N.; Montes-Cano, M.A.; Calderón, E.J. Association between Human-Pneumocystis Infection and Small-Cell Lung Carcinoma. Eur. J. Clin. Investig. 2004, 34, 229–235. [Google Scholar] [CrossRef]
- Nevez, G.; Magois, E.; Duwat, H.; Gouilleux, V.; Jounieaux, V.; Totet, A. Apparent Absence of Pneumocystis Jirovecii in Healthy Subjects. Clin. Infect. Dis. 2006, 42, e99–e101. [Google Scholar] [CrossRef] [Green Version]
- Mori, S.; Cho, I.; Sugimoto, M. A Followup Study of Asymptomatic Carriers of Pneumocystis Jiroveci during Immunosuppressive Therapy for Rheumatoid Arthritis. J. Rheumatol. 2009, 36, 1600–1605. [Google Scholar] [CrossRef] [Green Version]
- Vargas, S.L.; Pizarro, P.; López-Vieyra, M.; Neira-Avilés, P.; Bustamante, R.; Ponce, C.A. Pneumocystis Colonization in Older Adults and Diagnostic Yield of Single versus Paired Noninvasive Respiratory Sampling. Clin. Infect. Dis. 2010, 50, e19–e21. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.F.; Ambrose, H.E.; Wakefield, A.E. Pneumocystis Carinii f. Sp. Hominis DNA in Immunocompetent Health Care Workers in Contact with Patients with P. Carinii Pneumonia. J. Clin. Microbiol. 2001, 39, 3877–3882. [Google Scholar] [CrossRef] [Green Version]
- Vélez, L.; Correa, L.T.; Maya, M.A.; Mejía, P.; Ortega, J.; Bedoya, V.; Ortega, H. Diagnostic Accuracy of Bronchoalveolar Lavage Samples in Immunosuppressed Patients with Suspected Pneumonia: Analysis of a Protocol. Respir. Med. 2007, 101, 2160–2167. [Google Scholar] [CrossRef] [Green Version]
- Helweg-Larsen, J.; Jensen, J.S.; Benfield, T.; Svendsen, U.G.; Lundgren, J.D.; Lundgren, B. Diagnostic Use of PCR for Detection of Pneumocystis Carinii in Oral Wash Samples. J. Clin. Microbiol. 1998, 36, 2068–2072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodiño, J.; Rincón, N.; Aguilar, Y.A.; Rueda, Z.V.; Herrera, M.; Vélez, L.A. [Microscopic diagnosis of Pneumocystis jirovecii pneumonia in bronchoalveolar lavage and oropharyngeal wash samples of immunocompromised patients with pneumonia]. Biomedica 2011, 31, 222–231. [Google Scholar] [CrossRef] [Green Version]
- Robberts, F.J.L.; Liebowitz, L.D.; Chalkley, L.J. Polymerase Chain Reaction Detection of Pneumocystis Jiroveci: Evaluation of 9 Assays. Diagn. Microbiol. Infect. Dis. 2007, 58, 385–392. [Google Scholar] [CrossRef]
- Ruijter, J.M.; Ramakers, C.; Hoogaars, W.M.H.; Karlen, Y.; Bakker, O.; van den Hoff, M.J.B.; Moorman, A.F.M. Amplification Efficiency: Linking Baseline and Bias in the Analysis of Quantitative PCR Data. Nucleic Acids Res. 2009, 37, e45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MM19A: Molecular Testing in Clinical Lab Environments. Available online: https://clsi.org/standards/products/molecular-diagnostics/documents/mm19/ (accessed on 5 November 2021).
- MM06A2E: Quantitative Molecular Methods for Diseases. Available online: https://clsi.org/standards/products/molecular-diagnostics/documents/mm06/ (accessed on 5 November 2021).
- MM03Ed3: Molecular Diagnostic Methods for Diseases. Available online: https://clsi.org/standards/products/molecular-diagnostics/documents/mm03/ (accessed on 5 November 2021).
- Singh, J. International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use. J. Pharmacol. Pharmacother. 2015, 6, 185–187. [Google Scholar] [CrossRef] [Green Version]
- Montesinos, I.; Delforge, M.-L.; Ajjaham, F.; Brancart, F.; Hites, M.; Jacobs, F.; Denis, O. Evaluation of a New Commercial Real-Time PCR Assay for Diagnosis of Pneumocystis Jirovecii Pneumonia and Identification of Dihydropteroate Synthase (DHPS) Mutations. Diagn. Microbiol. Infect. Dis. 2017, 87, 32–36. [Google Scholar] [CrossRef]
- Botterel, F.; Cabaret, O.; Foulet, F.; Cordonnier, C.; Costa, J.-M.; Bretagne, S. Clinical Significance of Quantifying Pneumocystis Jirovecii DNA by Using Real-Time PCR in Bronchoalveolar Lavage Fluid from Immunocompromised Patients. J. Clin. Microbiol. 2012, 50, 227–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudramurthy, S.M.; Sharma, M.; Sharma, M.; Rawat, P.; Ghosh, A.; Venkatesan, L.; Aggarwal, R.; Singh, M.; Chakrabarti, A. Reliable Differentiation of Pneumocystis Pneumonia from Pneumocystis Colonisation by Quantification of Major Surface Glycoprotein Gene Using Real-Time Polymerase Chain Reaction. Mycoses 2018, 61, 96–103. [Google Scholar] [CrossRef]
- Fujisawa, T.; Suda, T.; Matsuda, H.; Inui, N.; Nakamura, Y.; Sato, J.; Toyoshima, M.; Nakano, Y.; Yasuda, K.; Gemma, H.; et al. Real-Time PCR Is More Specific than Conventional PCR for Induced Sputum Diagnosis of Pneumocystis Pneumonia in Immunocompromised Patients without HIV Infection. Respirology 2009, 14, 203–209. [Google Scholar] [CrossRef]
- Rohner, P.; Jacomo, V.; Studer, R.; Schrenzel, J.; Graf, J.-D. Detection of Pneumocystis Jirovecii by Two Staining Methods and Two Quantitative PCR Assays. Infection 2009, 37, 261–265. [Google Scholar] [CrossRef]
- Orsi, C.F.; Bettua, C.; Pini, P.; Venturelli, C.; La Regina, A.; Morace, G.; Luppi, M.; Forghieri, F.; Bigliardi, S.; Luppi, F.; et al. Detection of Pneumocystis Jirovecii and Aspergillus Spp. DNa in Bronchoalveolar Lavage Fluids by Commercial Real-Time PCr Assays: Comparison with Conventional Diagnostic Tests. New Microbiol. 2015, 38, 75–84. [Google Scholar] [PubMed]
- Orsi, C.F.; Gennari, W.; Venturelli, C.; La Regina, A.; Pecorari, M.; Righi, E.; Machetti, M.; Blasi, E. Performance of 2 Commercial Real-Time Polymerase Chain Reaction Assays for the Detection of Aspergillus and Pneumocystis DNA in Bronchoalveolar Lavage Fluid Samples from Critical Care Patients. Diagn. Microbiol. Infect. Dis. 2012, 73, 138–143. [Google Scholar] [CrossRef]
- Issa, N.; Gabriel, F.; Baulier, G.; Mourissoux, G.; Accoceberry, I.; Guisset, O.; Camou, F. Pneumocystosis and Quantitative PCR. Med. Mal. Infect. 2018, 48, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Bandt, D.; Monecke, S. Development and Evaluation of a Real-Time PCR Assay for Detection of Pneumocystis Jiroveci. Transpl. Infect. Dis. 2007, 9, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Guillaud-Saumur, T.; Nevez, G.; Bazire, A.; Virmaux, M.; Papon, N.; Le Gal, S. Comparison of a Commercial Real-Time PCR Assay, RealCycler® PJIR Kit, Progenie Molecular, to an in-House Real-Time PCR Assay for the Diagnosis of Pneumocystis Jirovecii Infections. Diagn. Microbiol. Infect. Dis. 2017, 87, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Huggett, J.F.; Taylor, M.S.; Kocjan, G.; Evans, H.E.; Morris-Jones, S.; Gant, V.; Novak, T.; Costello, A.M.; Zumla, A.; Miller, R.F. Development and Evaluation of a Real-Time PCR Assay for Detection of Pneumocystis Jirovecii DNA in Bronchoalveolar Lavage Fluid of HIV-Infected Patients. Thorax 2008, 63, 154–159. [Google Scholar] [CrossRef] [Green Version]
- McTaggart, L.R.; Wengenack, N.L.; Richardson, S.E. Validation of the MycAssay Pneumocystis Kit for Detection of Pneumocystis Jirovecii in Bronchoalveolar Lavage Specimens by Comparison to a Laboratory Standard of Direct Immunofluorescence Microscopy, Real-Time PCR, or Conventional PCR. J. Clin. Microbiol. 2012, 50, 1856–1859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalpke, A.H.; Hofko, M.; Zimmermann, S. Development and Evaluation of a Real-Time PCR Assay for Detection of Pneumocystis Jirovecii on the Fully Automated BD MAX Platform. J. Clin. Microbiol. 2013, 51, 2337–2343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chien, J.-Y.; Liu, C.-J.; Chuang, P.-C.; Lee, T.-F.; Huang, Y.-T.; Liao, C.-H.; Hung, C.-C.; Sheng, W.-H.; Yu, C.-J.; Hsueh, P.-R. Evaluation of the Automated Becton Dickinson MAX Real-Time PCR Platform for Detection of Pneumocystis Jirovecii. Future Microbiol. 2017, 12, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.F.; Limper, A.H. Pneumocystis Pneumonia. N. Engl. J. Med. 2004, 350, 2487–2498. [Google Scholar] [CrossRef]
- Pereira, R.M.; Müller, A.L.; Zimerman, R.A.; Antunes, D.B.; Zinn, V.F.; Friaza, V.; de la Horra, C.; Calderón, E.J.; Wissmann, G. High Prevalence of Pneumocystis Jirovecii Colonization among HIV-Positive Patients in Southern Brazil. Med. Mycol. 2014, 52, 804–809. [Google Scholar] [CrossRef]
- Le Gal, S.; Damiani, C.; Rouillé, A.; Grall, A.; Tréguer, L.; Virmaux, M.; Moalic, E.; Quinio, D.; Moal, M.-C.; Berthou, C.; et al. A Cluster of Pneumocystis Infections among Renal Transplant Recipients: Molecular Evidence of Colonized Patients as Potential Infectious Sources of Pneumocystis Jirovecii. Clin. Infect. Dis. 2012, 54, e62–e71. [Google Scholar] [CrossRef]
- Samuel, C.M.; Whitelaw, A.; Corcoran, C.; Morrow, B.; Hsiao, N.-Y.; Zampoli, M.; Zar, H.J. Improved Detection of Pneumocystis Jirovecii in Upper and Lower Respiratory Tract Specimens from Children with Suspected Pneumocystis Pneumonia Using Real-Time PCR: A Prospective Study. BMC Infect. Dis. 2011, 11, 329. [Google Scholar] [CrossRef] [Green Version]
- Pennington, K.; Wilson, J.; Limper, A.H.; Escalante, P. Positive Pneumocystis Jirovecii Sputum PCR Results with Negative Bronchoscopic PCR Results in Suspected Pneumocystis Pneumonia. Can. Respir. J. 2018, 2018, 6283935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, M.; Rashid, F.A.; Sabri, F.S.A.H.; Jamil, N.N.; Zain, R.; Hashim, R.; Amran, F.; Kok, H.T.; Samad, M.A.A.; Ahmad, N. Comparing Nasopharyngeal Swab and Early Morning Saliva for the Identification of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2021, 72, e352–e356. [Google Scholar] [CrossRef]
- Medrano, F.J.; Montes-Cano, M.; Conde, M.; de la Horra, C.; Respaldiza, N.; Gasch, A.; Perez-Lozano, M.J.; Varela, J.M.; Calderon, E.J. Pneumocystis Jirovecii in General Population. Emerg. Infect. Dis. 2005, 11, 245–250. [Google Scholar] [CrossRef]
- Respaldiza, N.; Montes-Cano, M.A.; Friaza, V.; Muñoz-Lobato, F.; Medrano, F.J.; Varela, J.M.; Calderon, E.; De la Horra, C. Usefulness of Oropharyngeal Washings for Identifying Pneumocystis Jirovecii Carriers. J. Eukaryot. Microbiol. 2006, 53 (Suppl. 1), S100–S101. [Google Scholar] [CrossRef]
- Matos, O.; Costa, M.C.; Lundgren, B.; Caldeira, L.; Aguiar, P.; Antunes, F. Effect of Oral Washes on the Diagnosis of Pneumocystis Carinii Pneumonia with a Low Parasite Burden and on Detection of Organisms in Subclinical Infections. Eur. J. Clin. Microbiol. Infect. Dis. 2001, 20, 573–575. [Google Scholar] [CrossRef] [PubMed]
- Vera, C.; Aguilar, Y.A.; Vélez, L.A.; Rueda, Z.V. High Transient Colonization by Pneumocystis Jirovecii between Mothers and Newborn. Eur. J. Pediatr. 2017, 176, 1619–1627. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 Immunocompromised People with Pneumonia | Group 2 People with Suspicion of Lung Cancer without Pneumonia | Group 3 Healthy Blood Donors | |
|---|---|---|---|
| Inclusion criteria | Individuals must have met all of the following criteria:
| Individuals must have met all of the following criteria:
| Individuals must have met all of the following criteria:
|
| Exclusion criteria |
|
| Those who had been in a hospital in the past month for more than 4 h/day |
| Characteristics | Group 1: Immunocompromised Patients with Pneumonia n = 158 | Group 2: Individuals with Lung Cancer n = 35 | Group 3: Healthy Individuals n = 20 |
|---|---|---|---|
| Male sex, n (%) | 113 (71.5) | 26/35 (74.3) | 11 (55) |
| Age in years, median (IQR) | 37 (29–45) | 63 (58–70) | 39 (21–50) |
| Respiratory symptoms, n (%) | 0 | ||
| Cough | 118 (75.2) | 24 (70.6) | |
| Dyspnea | 63 (40.1) | 19 (55.9) | |
| Pleuritic pain | 27 (17.2) | 6 (17.6) | |
| Hemoptysis | 14 (8.9) | 9 (26.5) | |
| Fever ≥ 38 °C | 121 (77) | 13 (38.2) | |
| Pleural effusion | 24 (15.3) | 14 (41.2) | |
| Past medical history (clinical condition at baseline), n (%) | 158 (100) | 0 | 0 |
| AIDS | 126 (79.7) | ||
| CD4, cells/mm3, median (IQR) | 53 (16–126) | ||
| CD4 < 200, cells/mm3, n (%) | 85 (88.5) | ||
| Transplanted | 22 (13.9) | ||
| Connective tissue disease | 5 (3.2) | ||
| Hematologic malignancies | 5 (3.2) | ||
| Total leukocytes cell/mm3, median (IQR) | 5760 (3700–7800) | 11,860 (8300–14,800) | |
| PMN | 4117 (2300–6175) | 8449 (5218–10,962) | |
| Lymphocyte | 835 (490–1460) | 2075 (1540–2772) | |
| Pulmonary lung infection | ** | 0 | N/A |
| Pneumocystis jirovecii | 25 (16) | ||
| Mycobacterium tuberculosis | 30 (19) | ||
| Cryptococcus neoformans | 6 (4) | ||
| Histoplasma capsulatum | 4 (2.5) | ||
| Bacteria | 11 (7) | ||
| Unknown | 84 (53) | ||
| ICU admission | 24 (15) | 0 | N/A |
| In-hospital mortality | 18 (11) | 1 (2.9) | N/A |
| Characteristics | PjP Ct < 24.5 N= 28 | Colonized Ct 24.5–37 N= 86 | Non-Infected Ct > 37 N= 44 | PjP vs. Colonized Individuals * PR; (CI 95%) | PjP vs. Non-Infected Individuals ** PR; (CI 95%) | Colonized vs. Non-Infected Individuals ** PR; (CI 95%) |
|---|---|---|---|---|---|---|
| Males, n (%) | 20 (71.4) | 62 (72.1) | 31 (70.5) | 0.976 (0.479–1.99) | 1.01; (0.75–1.37) | 1.02; (0.81–1.29) |
| Past medical history (clinical condition at baseline) | ||||||
| AIDS, n (%) | 27 (96.4) | 64 (74.4) | 35 (79.5) | 6.82 (0.98–47.62) | 1.212; (1.03–1.43) | 0.94; (0.77–1.14) |
| Prior ART treatment, n (%) | 2/13 (15.4) | 19/45 (42.2) | 17/30 (56.7) | 2.92 (0.71–12.06) | 0.27; (0.07–1.01) | 0.74; (0.47–1.18) |
| CD4 < 200, cells/mm3, n (%) | 20/20 (100) | 41/46 (89.1) | 24/29 (82.8) | NE | 1.21; (1.02–1.43) | 1.08; (0.89–1.31) |
| HIV viral load > 50.000, n (%) | 9/13 (69.2) | 21/32 (65.6) | 18/22 (81.8) | 1.13 (0.41–3.06) | 0.85; (0.56–1.28) | 0.80; (0.58–1.10) |
| Transplanted, n (%) | 1 (3.6) | 17 (19.8) | 4 (9.1) | 0.23 (0.03–1.54) | 0.39; (0.05–3.34) | 2.17; (0.78–6.07) |
| Hematologic malignancies, n (%) | 0 | 3 (3.5) | 2 (4.5) | NE | 0 | 0.77; (0.13–4.43) |
| Systematic lupus erythematosus, n (%) | 0 | 2 (2.3) | 3 (6.8) | NE | 0 | 0.34; (0.06–1.97) |
| Prior corticosteroid therapy n/N (%) | 0/1 | 5/18 (27.8) | 4/5 (80) | 0.18 (0.02–1.27) | 0 | 0.35; (0.15–0.82) |
| Neutrophils < 1500 cells/mm3 | 0/1 | 2/21 (9.5) | 2/9 (22.2) | 0.39 (0.06–2.54) | 0 | 0.43; (0.07–2.59) |
| No history of prophylaxis with trimethoprim/sulfamethoxazole for >12 weeks | 28/28 (100) | 70/85 (82.4) | 33/44 (75) | NE | 1.33; (1.12–1.58) | 1.09; (0.91–1.34) |
| Respiratory symptoms, n (%) | ||||||
| Cough | 27/28 (96.4) | 59/85 (69.4) | 32/44 (72.7) | 8.47; (1.20–59.49) | 1.33; (1.09–1.61) | 0.95; (0.76–1.20) |
| Dyspnea | 24/28 (85.7) | 26/85 (30.6) | 13/44 (29.5) | 7.56; (2.80–20.37) | 2.90; (1.79–4.69) | 1.03; (0.59–1.81) |
| Pleuritic pain | 3/28 (10.7) | 5/85 (5.9) | 7/44 (15.9) | 1.58; (0.60–4.10) | 0.67; (0.19–2.39) | 0.37; (0.12–1.10) |
| Chest pain | 7/28 (25) | 12/85 (14.1) | 8/44 (18.2) | 1.65; (0.82–3.32) | 1.38; (0.56–3.37) | 0.78; (0.34–1.76) |
| Hemoptysis | 1/28 (3.6) | 7/85 (8.2) | 6/44 (13.6) | 0.49; (0.08–3.13) | 0.26; (0.03–2.06) | 0.60; (0.22–1.69) |
| Fever ≥ 38 °C | 23/28 (82.1) | 65/85 (76.5) | 33/44 (75) | 1.31; (0.55–3.09) | 1.09; (0.86–1.39) | 1.02; (0.83–1.26) |
| Pulse oximetry < 90 | 12/21 (57.1) | 8/60 (13.3) | 6/30 (20) | 4.07; (2.02–8.2) | 2.85; (1.28–6.39) | 0.67; (0.25–1.75) |
| Respiratory frequency > 20 breaths/min | 22/28 (78.6) | 26/85 (30.6) | 18/43 (41.8) | 4.97; (2.18–11.3) | 1.88; (1.26–2.81) | 0.73; (0.45–1.18) |
| Tachycardia | 17/28 (60.7) | 31/85 (36.5) | 13/44 (70.6) | 2.09; (1.08–4.05) | 2.05; (1.19–3.54) | 1.23; (0.72–2.11) |
| Lymphocytes < 750 cells/mm3 | 15/28 (53.6) | 39/84 (46.4) | 15/44 (34.1) | 1.239 (0.65–2.36) | 1.57; (0.91–2.69) | 1.36; (0.85–2.18) |
| LDH > 450 UI/L (n = 118) | 16/24 (66.7) | 19/62 (30.6) | 10/32 (31.2) | 2.91 (1.40–6.06) | 2.13; (1.19–3.84) | 0.98; (0.52–1.85) |
| Radiographic features, n (%) | ||||||
| Normal radiographic | 4/28 (14.3) | 26/81 (32.1) | 12/44 (27.3) | 0.44; (0.166–1.16) | 0.53; (0.188–1.46) | 1.18; (0.66–2.10) |
| Interstitial opacities | 23/28 (82.1) | 39/81 (48.2) | 21/44 (47.7) | 3.49; (1.43–8.49) | 1.72; (1.21–2.45) | 1.01; (0.69–1.48) |
| Pleural effusion | 2/28 (7.1) | 15/85 (17.6) | 7/44 (15.9) | 0.43; (0.11–1.66) | 0.45; (0.10–2.01) | 1.11; (0.49–2.52) |
| Ground-glass pattern | 13/16 (81.3) | 11/53 (20.8) | 5/31 (16.1) | 8.13; (2.56–25.75) | 5.04; (2.18–11.63) | 1.29; (0.49–3.36) |
| Complications and clinical outcomes | ||||||
| Acute respiratory distress syndrome | 9/28 (32.1) | 7/85 (8.2) | 2/44 ((4.6) | 2.87; (1.59–5.19) | 7.07; (1.65–30.36) | 1.81; (0.39–8.36) |
| Pneumothorax | 0/28 (0) | 2/85 (2.4) | 1/44 (2.3) | NE | 0 | 1.04; (0.09–11.11) |
| ICU admission | 9/28 (32.1) | 11/85 (12.9) | 4/44 (9.1) | 2.20; (1.17–1.13) | 3.54; (1.20–10.39) | 1.42; (0.48–4.213) |
| Mechanical ventilation required | 6/28 (21.4) | 10/85 (11.8) | 4/44 (9.1) | 2.20; (1.17–4.13) | 2.36; (0.73–7.62) | 1.29; (0.43–3.89) |
| In-hospital mortality | 4/28 (14.3) | 10/86 (11.6) | 4/44 (9.1) | 1.19 (0.49–2.92) | 1.57; (0.43–5.78) | 1.28; (0.43–3.85) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aguilar, Y.A.; Rueda, Z.V.; Maya, M.A.; Vera, C.; Rodiño, J.; Muskus, C.; Vélez, L.A. Is It Possible to Differentiate Pneumocystis jirovecii Pneumonia and Colonization in the Immunocompromised Patients with Pneumonia? J. Fungi 2021, 7, 1036. https://doi.org/10.3390/jof7121036
Aguilar YA, Rueda ZV, Maya MA, Vera C, Rodiño J, Muskus C, Vélez LA. Is It Possible to Differentiate Pneumocystis jirovecii Pneumonia and Colonization in the Immunocompromised Patients with Pneumonia? Journal of Fungi. 2021; 7(12):1036. https://doi.org/10.3390/jof7121036
Chicago/Turabian StyleAguilar, Yudy A., Zulma Vanessa Rueda, María Angélica Maya, Cristian Vera, Jenniffer Rodiño, Carlos Muskus, and Lázaro A. Vélez. 2021. "Is It Possible to Differentiate Pneumocystis jirovecii Pneumonia and Colonization in the Immunocompromised Patients with Pneumonia?" Journal of Fungi 7, no. 12: 1036. https://doi.org/10.3390/jof7121036