
A Rare Case of Imported Cutaneous Leishmaniasis Caused by Leishmania infantum in the Republic of Korea, 2021
 , and
, and 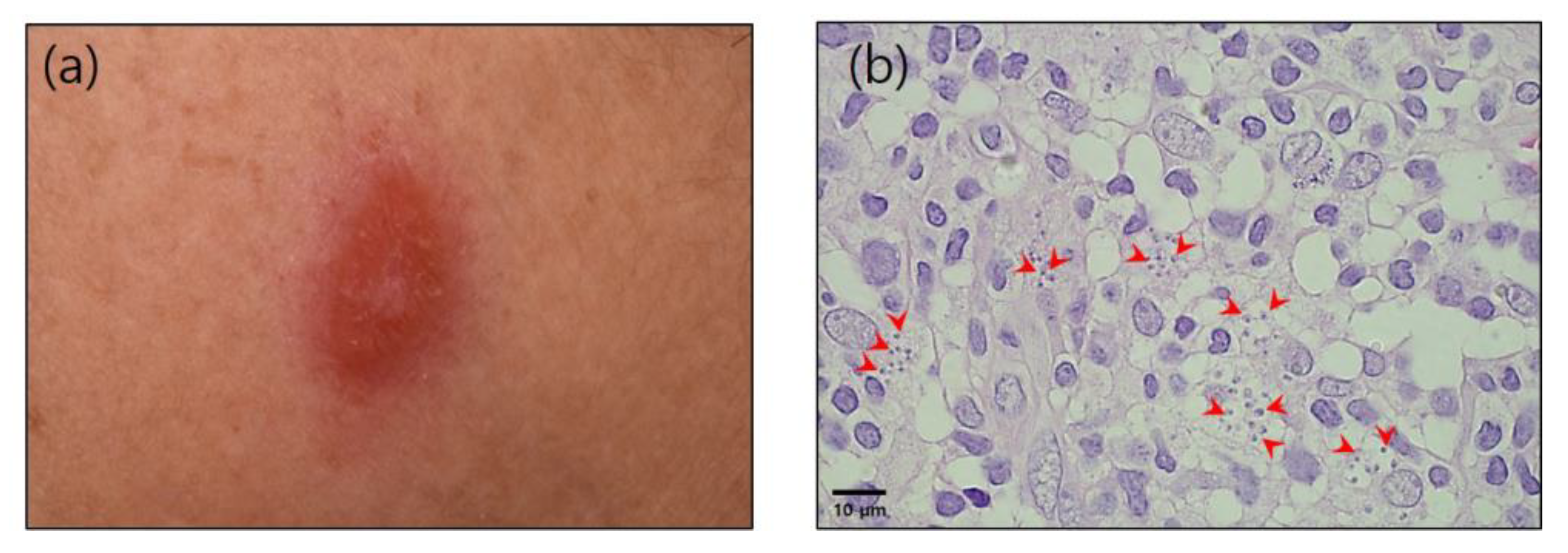{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
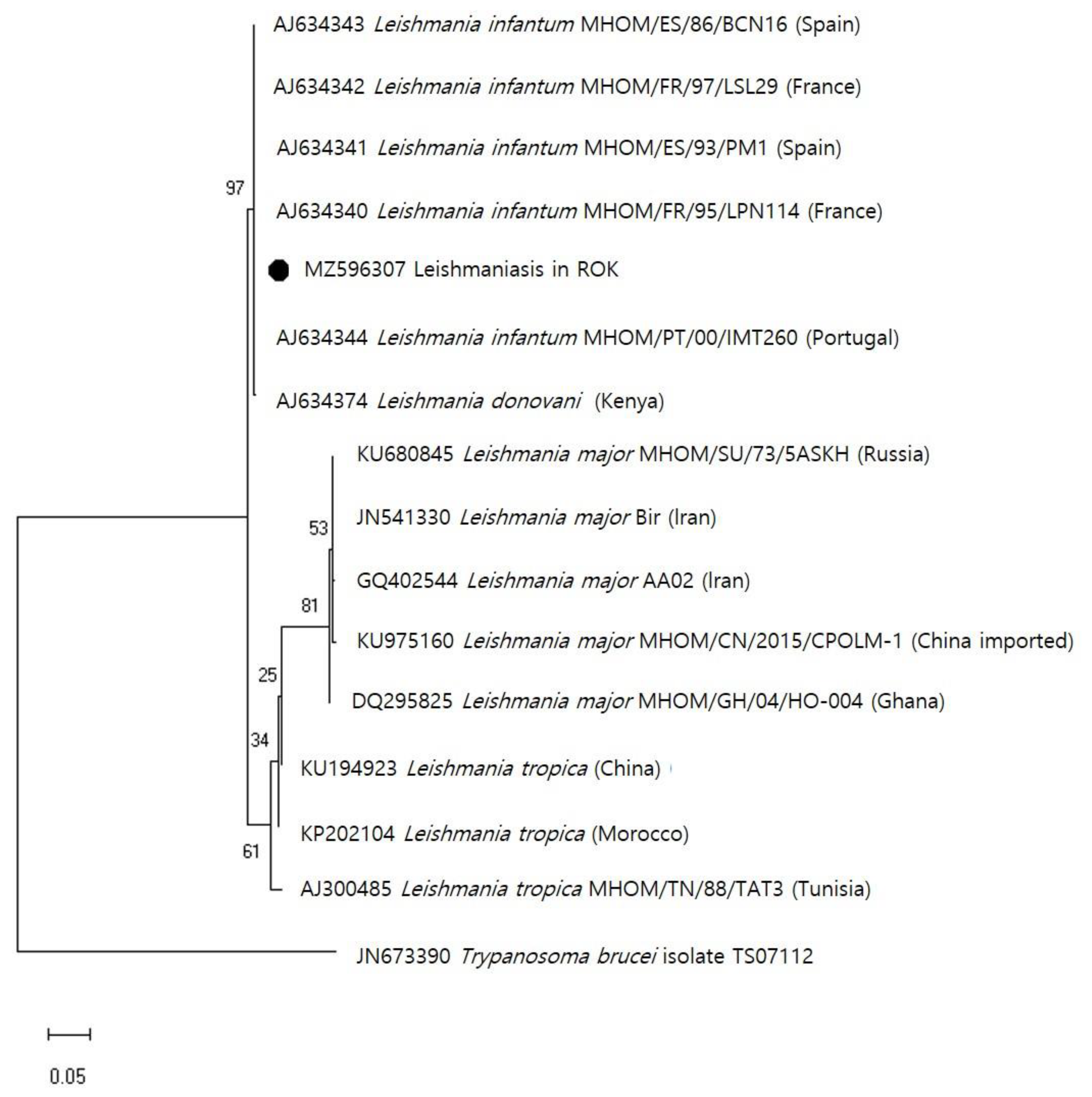
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Leishmaniasis Surveillance. A Baseline for the 2030 Road Map. Available online: https://www.who.int/publications/i/item/who-wer9635-401-419 (accessed on 3 September 2021).
- Nazzaro, G.; Rovaris, M.; Veraldi, S. Leishmaniasis: A disease with many names. JAMA Dermatol. 2014, 150, 1204. [Google Scholar] [CrossRef]
- Torres-Guerrero, E.; Quintanilla-Cedillo, M.R.; Ruiz-Esmenjaud, J.; Arenas, R. Leishmaniasis: A review. F1000Research 2017, 6, 750. [Google Scholar] [CrossRef]
- del Giudice, P.; Marty, P.; Lacour, J.P.; Perrin, C.; Pratlong, F.; Haas, H.; Dellamonica, P.; Le Fichoux, Y. Cutaneous leishmaniasis due to Leishmania infantum. Case reports and literature review. Arch. Dermatol. 1998, 134, 193–198. [Google Scholar] [CrossRef]
- Campino, L.; Pratlong, F.; Abranches, P.; Rioux, J.A.; Santos-Gomes, G.; Alves-Pires, C.; Cortes, S.; Ramada, J.; Cristovão, J.M.; Afonso, M.O.; et al. Leishmaniasis in Portugal: Enzyme polymorphism of Leishmania infantum based on the identification of 213 strains. Trop. Med. Int. Health 2006, 11, 1708–1714. [Google Scholar] [CrossRef] [PubMed]
- Pace, D.; Williams, T.N.; Grochowska, A.; Betts, A.; Attard-Montalto, S.; Boffa, M.J.; Vella, C. Manifestations of paediatric Leishmania infantum infections in Malta. Travel Med. Infect. Dis. 2011, 9, 37–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heu, I.M. Three Cases of Kala-Azar, Especially on the Various Serologic Reaction. Korean J. Intern. Med. 1952, 1, 118–121. [Google Scholar]
- Yoo, T.Y.; Chang, B.K.; Lee, S.H. Two Cases of Cutaneous Leishmaniasis. Korean J. Dermatol. 1978, 16, 447–486. [Google Scholar]
- Kim, H.J.; Shin, D.H.; Kim, Y.W. Five Cases of Cutaneous Leishmaniasis. Korean J. Dermatol. 1984, 22, 60–67. [Google Scholar]
- Yun, T.Y.; Eun, H.C.; Lee, Y.S.; Chi, J.G.; Ham, E.K.; Hong, S.T.; Lee, S.H. Two Cases of Imported Cutaneous Leishmaniasis in Korea. Kisaengchunghak Chapchi 1985, 23, 327–330. [Google Scholar] [CrossRef]
- Park, J.S.; Lee, D.K.; Hong, S.J.; Son, S.J.; Cho, M.K. A Case of Cutaneous Leishmaniasis. Korean J. Dermatol. 2001, 39, 725–727. [Google Scholar]
- Kim, D.Y.; Cho, S.B.; Chung, K.Y. A Case of Cutaneous Leishmaniasis Treated with Intralesional Injection of Meglumine Antimoniate. Korean J. Dermatol. 2006, 44, 113–116. [Google Scholar]
- Chi, J.G.; Shong, Y.K.; Hong, S.T.; Lee, S.H.; Seo, B.S.; Choe, K.W. An Imported Case of Kala-Azar in Korea. Kisaengchunghak Chapchi 1983, 21, 87–94. [Google Scholar] [CrossRef]
- Kim, H.Y.; Jung, S.E.; Park, K.W.; Kim, W.K. Visceral Leishmaniasis in a Child. J. Korean Assoc. Pediatr. Surg. 2004, 10, 35–38. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.Y.; Lee, Y.B.; Cho, B.K.; Park, H.J. New World Cutaneous Leishmaniasis Treated with Intralesional Injection of Pentavalent Antimony. Ann. Dermatol. 2013, 25, 80–83. [Google Scholar] [CrossRef] [Green Version]
- Schönian, G.; Nasereddin, A.; Dinse, N.; Schweynoch, C.; Schallig, H.D.; Presber, W.; Jaffe, C.L. PCR Diagnosis and Characterization of Leishmania in Local and Imported Clinical Samples. Diagn. Microbiol. Infect. Dis. 2003, 47, 349–358. [Google Scholar] [CrossRef]
- Mhaidi, I.; El Kacem, S.; Ait Kbaich, M.; El Hamouchi, A.; Sarih, M.; Akarid, K.; Lemrani, M. Molecular Identification of Leishmania Infection in the Most Relevant Sand Fly Species and in Patient Skin Samples from a Cutaneous Leishmaniasis Focus, in Morocco. PLoS Negl. Trop. Dis. 2018, 12, e0006315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cecílio, P.; Cordeiro-da-Silva, A.; Oliveira, F. Sand flies: Basic information on the vectors of leishmaniasis and their interactions with Leishmania parasites. Commun. Biol. 2022, 5, 305. [Google Scholar] [CrossRef]
- Sharma, U.; Singh, S. Insect Vectors of Leishmania: Distribution, Physiology and Their Control. J. Vector Borne Dis. 2008, 45, 255–272. [Google Scholar]
- González, C.; Wang, O.; Strutz, S.E.; González-Salazar, C.; Sánchez-Cordero, V.; Sarkar, S. Climate Change and Risk of Leishmaniasis in North America: Predictions from Ecological Niche Models of Vector and Reservoir Species. PLoS Negl. Trop. Dis. 2010, 4, e585. [Google Scholar] [CrossRef] [Green Version]
- Cunze, S.; Kochmann, J.; Koch, L.K.; Hasselmann, K.J.Q.; Klimpel, S. Leishmaniasis in Eurasia and Africa: Geographical Distribution of Vector Species and Pathogens. R. Soc. Open Sci. 2019, 6, 190334. [Google Scholar] [CrossRef] [Green Version]
- Díaz-Sáez, V.; Corpas-López, V.; Merino-Espinosa, G.; Morillas-Mancilla, M.J.; Abattouy, N.; Martín-Sánchez, J. Seasonal Dynamics of Phlebotomine Sand Flies and Autochthonous Transmission of Leishmania infantum in High-Altitude Ecosystems in Southern Spain. Acta Trop. 2021, 213, 105749. [Google Scholar] [CrossRef] [PubMed]
- Maroli, M.; Rossi, L.; Baldelli, R.; Capelli, G.; Ferroglio, E.; Genchi, C.; Gramiccia, M.; Mortarino, M.; Pietrobelli, M.; Gradoni, L. The Northward Spread of Leishmaniasis in Italy: Evidence from Retrospective and Ongoing Studies on the Canine Reservoir and Phlebotomine Vectors. Trop. Med. Int. Health 2008, 13, 256–264. [Google Scholar] [CrossRef]
- Barón, S.D.; Morillas-Márquez, F.; Morales-Yuste, M.; Díaz-Sáez, V.; Irigaray, C.; Martín-Sánchez, J. Risk Maps for the Presence and Absence of Phlebotomus Perniciosus in an Endemic Area of Leishmaniasis in Southern Spain: Implications for the Control of the Disease. Parasitology 2011, 138, 1234–1244. [Google Scholar] [CrossRef]
- Pavli, A.; Maltezou, H.C. Leishmaniasis, an Emerging Infection in Travelers. Int. J. Infect. Dis. 2010, 14, e1032–e1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berriatua, E.; Maia, C.; Conceição, C.; Özbel, Y.; Töz, S.; Baneth, G.; Pérez-Cutillas, P.; Ortuño, M.; Muñoz, C.; Jumakanova, Z.; et al. Leishmaniases in the European Union and Neighboring Countries. Emerg. Infect. Dis. 2021, 27, 1723–1727. [Google Scholar] [CrossRef]
- Rocha, R.; Pereira, A.; Maia, C. Non-Endemic Leishmaniases Reported Globally in Humans between 2000 and 2021-A Comprehensive Review. Pathogens. 2022, 11, 921. [Google Scholar] [CrossRef]
- Lederman, E.R.; Weld, L.H.; Elyazar, I.R.; von Sonnenburg, F.; Loutan, L.; Schwartz, E.; Keystone, J.S. Dermatologic conditions of the ill returned traveler: An analysis from the GeoSentinel Surveillance Network. Int. J. Infect. Dis. 2008, 12, 593–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Auwera, G.; Davidsson, L.; Buffet, P.; Ruf, M.T.; Gramiccia, M.; Varani, S.; Chicharro, C.; Bart, A.; Harms, G.; Chiodini, P.L.; et al. LeishMan Surveillance Network members who contributed to this article (in addition to authors above). Surveillance of Leishmaniasis Cases from 15 European Centres, 2014 to 2019: A Retrospective Analysis. Eurosurveillance 2022, 27, 2002028. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.N.; John, L.; Bruceson, A.D.; Lockwood, D.N. Changing pattern of visceral leishmaniasis, United Kingdom, 1985–2004. Emerg. Infect. Dis. 2006, 12, 1257–1259. [Google Scholar] [CrossRef] [PubMed]
- Aissaoui, N.; Hamane, S.; Gits-Muselli, M.; Petit, A.; Benderdouche, M.; Denis, B.; Alanio, A.; Dellière, S.; Bagot, M.; Bretagne, S. Imported Leishmaniasis in Travelers: A 7-Year Retrospective from a Parisian Hospital in France. BMC Infect. Dis. 2021, 21, 953. [Google Scholar] [CrossRef] [PubMed]
- Kitano, H.; Sanjoba, C.; Goto, Y.; Iwamoto, K.; Kitagawa, H.; Nomura, T.; Omori, K.; Shigemoto, N.; Hide, M.; Matsumoto, Y.; et al. Complicated Cutaneous Leishmaniasis Caused by an Imported Case of Leishmania tropica in Japan: A Case Report. Trop. Med. Health 2021, 49, 20. [Google Scholar] [CrossRef] [PubMed]
- Hockmeyer, W.T.; Kager, P.A.; Rees, P.H.; Hendricks, L.D. The culture of Leishmania donovani in Schneider’s insect medium: Its value in the diagnosis and management of patients with visceral leishmaniasis. Trans. R. Soc. Trop. Med. Hyg. 1981, 75, 861–863. [Google Scholar] [CrossRef]
- Markle, W.H.; Makhoul, K. Cutaneous leishmaniasis: Recognition and treatment. Am. Fam. Physician 2004, 69, 1455–1460. [Google Scholar]
- Aviles, H.; Belli, A.; Armijos, R.; Monroy, F.P.; Harris, E. PCR detection and identification of Leishmania parasites in clinical specimens in Ecuador: A comparison with classical diagnostic methods. J. Parasitol. 1999, 85, 181–187. [Google Scholar] [CrossRef]
- Goto, H.; Lindoso, J.A. Current diagnosis and treatment of cutaneous and mucocutaneous leishmaniasis. Expert Rev. Anti-Infect. Ther. 2010, 8, 419–433. [Google Scholar] [CrossRef]
- Maia, C.; Campino, L. Methods for Diagnosis of Canine Leishmaniasis and Immune Response to Infection. Vet. Parasitol. 2008, 158, 274–287. [Google Scholar] [CrossRef] [PubMed]
- Reimão, J.Q.; Coser, E.M.; Lee, M.R.; Coelho, A.C. Laboratory Diagnosis of Cutaneous and Visceral Leishmaniasis: Current and Future Methods. Microorganisms 2020, 8, 1632. [Google Scholar] [CrossRef] [PubMed]
- Gow, I.; Smith, N.C.; Stark, D. Laboratory diagnostics for human Leishmania infections: A polymerase chain reaction-focussed review of detection and identification methods. Parasit. Vectors 2022, 15, 412. [Google Scholar] [CrossRef] [PubMed]
- De Ruiter, C.M.; Van Der Veer, C.; Leeflang, M.M.G.; Deborggraeve, S.; Lucas, C.; Adams, E.R. Molecular tools for diagnosis of visceral leishmaniasis: Systematic review and meta-analysis of diagnostic test accuracy. J. Clin. Microbiol. 2014, 52, 3147–3155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castelli, G.; Bruno, F.; Reale, S.; Catanzaro, S.; Valenza, V.; Vitale, F. Molecular Diagnosis of Leishmaniasis: Quantification of Parasite Load by a Real-Time PCR Assay with High Sensitivity. Pathogens 2021, 10, 865. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.; Isles, N.S.; Seemann, T. Case Report: Confirmation by Metagenomic Sequencing of Visceral Leishmaniasis in an Immunosuppressed Returned Traveler. Am. J. Trop. Med. Hyg. 2020, 103, 1930–1933. [Google Scholar] [CrossRef]
- Domagalska, M.A.; Imamura, H.; Sanders, M.; Van den Broeck, F.; Bhattarai, N.R.; Vanaerschot, M.; Maes, I.; D’Haenens, E.; Rai, K.; Rijal, S. Genomes of Leishmania parasites directly sequenced from patients with visceral leishmaniasis in the Indian subcontinent. PLoS Negl. Trop. Dis. 2019, 13, e0007900. [Google Scholar] [CrossRef] [Green Version]
- Mann, S.; Frasca, K.; Scherrer, S.; Henao-Martínez, A.F.; Newman, S.; Ramanan, P.; Suarez, J.A. A Review of Leishmaniasis: Current Knowledge and Future Directions. Curr. Trop. Med. Rep. 2021, 8, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Yadav, P.; Azam, M.; Ramesh, V.; Singh, R. Unusual Observations in Leishmaniasis—An Overview. Pathogens 2023, 12, 297. [Google Scholar] [CrossRef]
- Rioux, J.A.; Lanotte, G.; Maazoun, R.; Perello, R.; Pratlong, F. Leishmania infantum Nicolle, 1908, agent du bouton d’Orient autochtone. A propos de l’identification biochimique de deus souches isolées dans les Pyrénées-Orientales [Leishmania infantum Nicolle, 1908, the agent of the autochthonous oriental sore. Apropos of the biochemical identification of 2 strains isolated in the eastern Pyrenees]. C. R. Seances Acad. Sci. D. 1980, 291, 701–703. [Google Scholar] [PubMed]
- Elmazini, S.; Ejghal, R.; Bekhti, K.; Lemrani, M. The Sporadic cutaneous leishmaniasis due to Leishmania infantum in Morocco: A presumably trend towards endemicity. Acta Trop. 2021, 227, 106288. [Google Scholar] [CrossRef] [PubMed]
- Thakur, L.; Singh, K.K.; Shanker, V.; Negi, A.; Jain, A.; Matlashewski, G.; Jain, M. Atypical leishmaniasis: A global perspective with emphasis on the Indian subcontinent. PLoS Negl. Trop. Dis. 2018, 12, e0006659. [Google Scholar] [CrossRef] [Green Version]
- Adamczick, C.; Dierig, A.; Welzel, T.; Schifferli, A.; Blum, I.; Ritz, N. Double trouble: Visceral leishmaniasis in twins after traveling to Tuscany—A case report. BMC Infect. Dis. 2018, 18, 495. [Google Scholar] [CrossRef]
- Crowe, A.; Slavin, J.; Sark, D.; Aboltins, C. A case of imported Leishmania infantum cutaneous leishmaniasis; an unusual presentation occurring 19 years after travel. BMC Infect. Dis. 2014, 14, 597. [Google Scholar] [CrossRef] [Green Version]
- Veraldi, S.; Gianotti, R.; Sala, F.; Coggi, A.; Venegoni, L.; Persico, M.C.; Berti, E. Latency time in cutaneous leishmaniasis. G Ital. Dermatol. Venereol. 2011, 146, 159–161. [Google Scholar]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.J.; Kim, E.J.; Choi, J.W.; Kim, Y.C.; Lee, H.-I.; Shin, H.-I. A Rare Case of Imported Cutaneous Leishmaniasis Caused by Leishmania infantum in the Republic of Korea, 2021. Trop. Med. Infect. Dis. 2023, 8, 223. https://doi.org/10.3390/tropicalmed8040223
Kim HJ, Kim EJ, Choi JW, Kim YC, Lee H-I, Shin H-I. A Rare Case of Imported Cutaneous Leishmaniasis Caused by Leishmania infantum in the Republic of Korea, 2021. Tropical Medicine and Infectious Disease. 2023; 8(4):223. https://doi.org/10.3390/tropicalmed8040223
Chicago/Turabian StyleKim, Hyun Jung, Eun Jin Kim, Jee Woong Choi, You Chan Kim, Hee-Il Lee, and Hyun-Il Shin. 2023. "A Rare Case of Imported Cutaneous Leishmaniasis Caused by Leishmania infantum in the Republic of Korea, 2021" Tropical Medicine and Infectious Disease 8, no. 4: 223. https://doi.org/10.3390/tropicalmed8040223