
Herbal- and Dietary-Supplement-Induced Liver Injury: A Review of the Recent Literature
by
 , , , and
, , , and
Palak A. Patel-Rodrigues
1,2,* ,
,
Lindsey Cundra
2,
Dalal Alhaqqan
2,
Daniel T. Gildea
2,
Stephanie M. Woo
2 and
James H. Lewis
2 1
Henry Ford Hospital, 2799 W Grand Blvd, Detroit, MI 48202, USA
2
MedStar Georgetown University Hospital, Washington, DC 20007, USA
*
Author to whom correspondence should be addressed.
Livers 2024, 4(1), 94-118; https://doi.org/10.3390/livers4010008
Submission received: 1 November 2023
/
Revised: 11 December 2023
/
Accepted: 22 January 2024
/
Published: 13 February 2024
Abstract
:Herbal-induced liver injury (HILI) continues to increase in prevalence each year due to the ongoing popularity of herbal supplements and complementary and alternative medicines. A detailed literature review of case reports and clinical studies published from March 2021 to March 2023 was performed. We discuss the epidemiology and diagnosis of HILI as well as the current and proposed laws and regulations. The 2021 ACG guidelines and 2022 AASLD practice guidelines for the diagnosis and management of drug and herbal-induced liver injury are discussed. We describe updates to previously reported etiologies of HILI such as ayurveda, ashwagandha, turmeric, kratom, green tea extract, and garcinia cambogia. Newly described supplements resulting in HILI, such as tinospora cordifolia, horse chestnut, alkaline water, and more, are described. We discuss newly and previously identified hepatoprotective herbal supplements as they have been reported in the study of animal models and human liver cells. This review suggests the need for ongoing research on the causes and mechanisms of HILI to ensure its proper diagnosis, prevention, and treatment in the future. The goal of this review is to provide novice and expert readers with knowledge regarding the possible etiologies of HILI and a general overview.
1. Introduction
The use of herbal supplements and complementary and alternative medicine (CAM) has been increasing in popularity over the past few decades. As a result, an increase in the reported cases of herbal-induced liver injury (HILI) and dietary supplement (HDS)-induced liver injury has been seen, with over 12,000 publications between the years of 2004 and 2020. The World Health Organization (WHO) estimates that 85% of developing countries utilize herbal supplements as part of health care [1]. Overall, the most common indications described for the use of herbal supplements are gastrointestinal symptoms followed by musculoskeletal pain. In the United States and Europe, utilization of herbal supplements for weight loss and psychiatric disorders appears to be more common [2]. Although reporting of HILI has increased, there has been a lack of progress made in standardization of reporting to aid in the diagnosis, risk stratification, and management of this condition.
Updated practice guidelines for herbal and dietary supplements from the American Association for the Study of Liver Diseases (AASLD) were recently published by Fontana et al. [3] It is reported that in 2019 consumers in the United States spent USD 9.6 billion on HDSs, and that multiple studies have found that liver failure secondary to HILI is more likely to result in liver transplantation or death when compared to DILI. The latest data from the Drug-Induced Liver Injury Network (DILIN) registry report that about 20% of liver injury reported is due to HDSs and that many HDSs are mislabeled [3]. The guidelines emphasize the difficulty in diagnosing HILI secondary to HDSs due to the variability of HDSs between each batch, latency of exposure, change in the supplement over time, and likely included ingredients that are not listed. There continues to be poor regulation of these products as well as little awareness of the danger of some of these HDSs. With increasing reports of HDS-induced liver injury, more research is being focused on identifying characteristics or patterns that may lead to HILI. As discussed by Fontana et al. [3], the active component for green tea extract has been identified as the polyphenolic catechins, which are thought to be the main etiology for green-tea-induced hepatocellular liver injury based on multiple case reports that have been published in DILIN. Further analyses have identified that green-tea-extract-induced liver injury, as well as that from Polygonum multiflorum, are associated with genetic marker HLA-B*35:01 [4]. Our review aims to analyze reports of HILI published during the past 2 years, highlighting new data regarding the epidemiology, mechanism, and causes of HILI and HDS, as well as identifying areas for research in the future since our last review on this topic [5].
2. Materials and Methods
All authors performed an extensive literature search utilizing PubMed searching for any clinical case reports, systemic reviews, and meta-analyses from peer-reviewed journals published from March of 2021 to March 2023. Examples of keywords utilized in the search process included “herbal induced drug injury”, “HILI”, “dietary supplement and liver injury”, “herbal and dietary supplement (HDS)-induced liver injury”, and “herbal supplementation and liver injury”. We also reviewed reported new cases and updates on prior HILI cases from the leading gastroenterology and hepatology journals within the time period specified. Cochrane, DILIN, LiverTox, Spanish DILI network, United Kingdom (UK) literature review, the Herbal Medicines Advisory Committee, Latin DILI network, International Regulatory Cooperation for Herbal Medicines (IRCH), and many peer-reviewed journals were reviewed. Our initial search utilized the key words listed above and, in the timeline, resulted in more than 300 articles. We removed duplicate articles and focused on publications specifying new updates or changes related to previously described herbal hepatotoxins, new causes of herbal-induced liver injury, new data on the hepatoprotective effects of herbal supplements, and updates concerning HILI in global registries. Each article was reviewed for its clinical significance and quality. Articles that focused specifically on DILI, were not written in the English language, or did not demonstrate high quality data were excluded. Our review yielded 101 articles that were included and summarized in our review (Figure 1). The impact factor of each journal was taken into account per the Journal Citation Reports. Our goal was to include articles published in journals with an impact factor >1. While not all journals reported an impact factor, if the information was still felt to be of clinical significance, it was included. As with prior reviews, the omission of any particular case report or study in this review should not be construed as lacking importance.
3. Updates in the Epidemiology of HILI
Ballotin and colleagues performed a comprehensive literature review of 5918 publications that associated herbal products with HILI dating back to the 1990s [2]. They reviewed over 900 case reports and 79 individual herbal products were found to be associated with HILI, with the most commonly reported being He-Shou-Wu, green tea extract, herbalife, kava kava, greater celandine, germander, hydroxycut, skullcap, kratom, gynura segetum, garcinia cambogia, senna, aloe vera, ma huang, and charpparall. Gurley et al. published a historical review of many past and current cases of HDS-induced liver jury, noting that most cases of liver injury are caused by multi-extract-containing or adulterated products [6]. Their article discusses the correlation between the rapid growth in the market of dietary supplements with adverse effects, as well as the need for better regulation and clinical assessment of the HDS products prior to entering the market.
Determining the true incidence of HILI is quite challenging due to the majority of cases being underreported and underdiagnosed, often due to limited access to healthcare in areas where herbal supplement use and CAM are more prevalent. There is a lack of consistent and representative data on the use of herbal supplements in the United States (US). The National Health and Nutrition Examination Survey (NHANES) is a survey that collects information from a representative sample of approximately 5000 non-institutionalized residents of the US per year and has been actively collecting data on the use of dietary supplements since 1971. Based on the most recent data from NHANES [7], it is estimated that 49% of the United States population above the age of 1 and over 70% of Americans above the age of 71 use dietary supplements. In the United States, only 23% of dietary supplements were recommended by a health care provider [8]. We postulate there may have been a rise in herbal and dietary supplement use during the past 2 years due to the COVID-19 pandemic, with more people resorting to preventative or protective measures. A recent study conducted in Turkey found that 46.1% of dietitians recommended use of herbal supplements during the pandemic to protect against COVID-19 [9].
4. Diagnosis of HILI
HILI continues to be challenging to diagnose and, as with DILI, largely remains a diagnosis of exclusion. As discussed by Vuppalanchi et al., the current and best approach to diagnosis of liver injury after exposure to an herbal supplement or drug lies in obtaining a thorough history from the patient, establishing symptoms and a timeline, as well as excluding other possible sources of liver injury [10]. Symptomatic patients with HILI typically present with vague symptoms such as fatigue, anorexia, nausea, or jaundice, while some patients may be completely asymptomatic and present with just elevations in aminotransferases and/or a cholestatic pattern of liver injury.
There remains a lack of a validated, unified causality assessment method (CAM) to aid in HILI diagnosis. The Roussel Uclaf Causality Assessment Method (RUCAM), validated in 1993 and updated in 2016, is a scoring system that was developed to assist in diagnosis of drug-induced liver injury (DILI), and has been increasingly used in HILI [11]. The scoring system of RUCAM is defined as the following: a score of zero or less rules out the drug as a cause of liver injury, 1–2 is an “unlikely” cause, 3–5 is a ”possible” cause, 6–8 is a “probable” cause, and greater than 8 is “highly probable”. Although the authors promote the use of RUCAM as part of the causality assessment, it is important to highlight that it does not take into account herb authentication, or components that may be added to or contaminate HDS. Over the years, there has been an active effort to further refine and improve RUCAM, which resulted in the recent development of a computer-assisted, electronic version called the Revised Electronic Causality Assessment Method (RECAM). RECAM uses a computer algorithm that considers the different categories in RUCAM, apart from the risk factors and concomitant drug use categories, and incorporates the information with existing drug databases such as LiverTox and DILIN to provide more accurate results [12]. RECAM was found to be non-inferior to RUCAM and proved to be more effective in the extremes of DILI causality compared to RUCAM. However, validation of RECAM regarding HILI is awaited.
5. Outcomes of HILI
There is substantial evidence demonstrating that the majority (94.5%) of patients diagnosed with HILI fully recover from their liver injury [1]. From 1979 to 2019, in 203 publications that utilized the RUCAM algorithm, 5% of the patients identified with HILI in published cases required a liver transplantation and 2% of cases were fatal [1]. Other analyses have described as many as 6% of 936 cases patients requiring a liver transplant. According to the Drug-Induced Liver Injury Network (DILIN), patients diagnosed with HILI have been found to have a higher probability of a more severe outcome when compared to DILI [1]. The retrospective review by Ballotin et al. [4] also determined that the majority of the patients (82.8%) recovered from HILI; however, 6.6% required liver transplantation, 1.5% developed chronic liver disease, and in 10.4% of cases, death was observed.
6. Current State of Herbal Supplement Laws and Regulations
There continues to be a significant lack of regulatory oversight from the Food and Drug Administration (FDA) when it comes to herbal supplements, a fact that is not consistently recognized outside of the medical community. The most notable movement on this issue in the past year is seen in the Dietary Supplement Listing Act, a bipartisan piece of legislation introduced in April 2022. If passed, this law would mandate that companies provide the FDA with a comprehensive list of their product’s ingredients, potential allergens, and appropriate warnings for those considering using the supplement. The FDA would then publish this information online, allowing consumers to have a fuller picture of the supplements they may be taking (Table 1) [13]. It remains to be seen whether the law will pass, and what its ultimate effect will be, as despite educatory efforts by the FDA to educate consumers on their role in supervising supplements, there does not seem to have been a significant impact [14]. Critics of the bill note that while it makes the impression of a legal impact on the production of supplements, it in fact does not grant the FDA any ability to regulate, approve, or reject products, or otherwise constrain or influence supplement producers [15].
At its core, the act would only allow the FDA to create a publishable database, to which it can mandate the submission of herbal product information. It would not change what can or cannot be placed on pharmacy shelves across the nation, and the onus remains on the consumer to access and utilize this information in whatever way they feel appropriate. It also does not change advertising laws and guidance, which center around the claims that can be made by manufacturers. Current guidance states the supplement cannot be adulterated or misbranded, and any specific claims must be backed by reasonable evidence [16]. However, there are no strict guidelines or pre-approval process, leaving significant leeway when it comes to the statements that are made and how far established science can be extrapolated. Given that any new potential database will have to contend with access issues, lack of public awareness, social media influence, and skeptical consumers, it may be that the act’s impact will ultimately be limited.
In the meantime, and perhaps for the foreseeable future, consumers will be confronted with products that recent studies show vary widely in quality. For instance, Maren et al. evaluated samples of supplements including ginger, valerian root, and St. John’s wort, demonstrating not only inconsistency in antioxidant and flavonoid concentrations, but also evidence of fungal contamination. Samples in this study were compared not only across different companies, but also across pills from within the same bottle—both groups of which demonstrated this worrisome degree of variation [14].
Recent FDA Warnings on HILI/HDS
Throughout 2021 and 2022, the FDA issued at least five sets of warnings to various companies for illegal marketing practices, four of which were for selling herbal supplements without sufficient evidence to support claims to treat diseases including infertility, depression and other mental illnesses, diabetes, and cardiovascular disease (Table 2). One of these warnings was sent to various companies for the illegal adulteration of dietary supplement products, which involved the inclusion of various ingredients that have been shown to cause harm, including to the cardiovascular system [17]. An example of a HDS that has become commonly ingested is kratom. Kratom has been banned in several states and other jurisdictions but remains “legal” in the rest of the United States. Kratom and its regulation will be discussed in further detail in the section below entitled “Updates in Previously Described HILI Etiologies”.
7. Updates of HILI/HDS in Global Registries
7.1. North America
The American College of Gastroenterology (ACG) published an updated guideline on the diagnosis and management of idiosyncratic drug-induced liver injury in 2021 [18]. Based on the most up-to-date DILIN registry data, HDSs constitute the second leading class of compounds causing liver injury, after antibiotics, and now accounting for up to 20% of the total cases [3]. Almost USD 10 billion was spent on HDS in 2019 in the United States. The United States Acute Liver Failure (ALF) Study Group Registry published an update in April 2022, of 2332 ALF cases of all etiologies over the past 20 years. A total of 235 cases were due to DILI (10%) and 42 additional cases were due to HILI (1.8%). Among 41 of 42 of the patients, 70.7% of the patients required transplant and 7 died [19]. There was almost a two-fold need for a liver transplant with HILI and an approximate three times greater transplant-free survival when comparing HDS-induced acute liver failure with non-HDS acute liver failure. The incidence of death was about two times greater in non-HDS ALF cases versus HDS-induced ALF.
The National Library of Medicine’s LiverTox website created five categories that describe the various likelihoods that specific drugs and herbal agents cause liver injury (Table 3). The top herbal supplements, including those resulting in acute liver failure, are listed in the table below along with their LiverTox causality designations (Table 4). Importantly, the table illustrates the fact that not all commonly used herbal agents have a risk of hepatotoxicity, which is consistent with the fact that while use of herbal therapies is commonplace, HILI remains rare.
7.2. Central and South America
In September/October 2021, the Latin American Association for Study of the Liver, with the support and involvement of the Latin DILI registry, published a management position paper for drug- and herbal-induced liver injury [20]. This is a wide-ranging guidance document, touching on many topics including the conduct of research, DILI risk factors, DILI diagnosis and management, prognosis, directions for future studies, and more. In terms of HILI, they touch on several points. One issue addressed is the common inclusion of anabolic steroids as a “dietary supplement”, arguing that this type of medication would be better classified as an “abuse agent” or “hormonal compound [20]”. In general, the paper calls for stricter definitions of HILI. As in other countries, it also notes increasing herbal consumption in Latin America, with a concomitant increase in liver injury risk. Additionally, liver injury due to herbal medications is very likely underreported, an issue that makes better understanding of the risks of these supplements difficult. The authors of the paper call for more countries to join the LatinDILI registry and the encouragement of HILI reporting to fully understand the impact of herbal liver injury in Latin America and beyond. They also call for stricter regulation of herbal drugs, particularly those used for bodybuilding, and an emphasis on individual-level behavioral change away from the usage of these medications [20].
7.3. Europe
A multicentric study from the Prospective European DILI Registry (Pro-Euro-DILI), a registry created for European DILI established in 2016, was published in July 2022 containing data from its inception in 2016 through 2021. Patients prospectively enrolled from the United Kingdom, Spain, Germany, Switzerland, Portugal, and Iceland. While the study, and the registry itself, focuses more on what this paper would term DILI rather than HILI, it subsumes herbal-induced injuries under the DILI heading, noting 18 cases out of the 246 that were caused by herbal and dietary supplements, including anabolic steroids [21]. Unfortunately, there is not much delineation in the way of types of herbs causing injury, but the report does describe one case requiring liver transplantation in a 55-year-old male who took a combination of various Chinese herbs, including Huang Lim, Huang Qin, Huang Bo, Zhi Zi, Sheng Di Huang, Mai Dong, and Xuan Shen. This patient subsequently developed hepatocellular liver injury and was transplanted 72 days after injury onset [21].
7.4. Asia
In Thailand, the Thai Association for the Study of the Liver (THASL), the largest data repository in the country and consisting of academic 12 medical centers, published a June 2022 report assessing drug and herbal-induced liver injury in 200 patients. Of these, there were 41 patients with and 159 without chronic liver disease. They found that complementary and alternative medicines were the most common causes of liver injury in both groups, consisting of 59% of cases of liver injury in the chronic liver disease group and 40% of cases in the non-chronic liver disease group [22]. These herbal medicines were grouped together in the analysis, from locations including China, Singapore, Japan, and India [22].
A prospective, multicenter study spanning more than 9 years in Taiwan compared patients with HILI to those with conventional drug-induced liver injury and found that up to 22% of drug-induced liver injury was attributable to herbal and dietary supplements [23]. Patients with HILI had a higher rate of complications and higher mortality rate compared to patients with conventional drug-induced liver injury (12.6% vs. 8.0%, p = 0.016). The authors identified several factors that were associated with increased mortality in HILI, including elevated liver enzymes at baseline, use of crude or unprocessed herbal supplements, and hepatitis B carrier status.
8. New Reports on Previously Described HILI Etiologies
Herbal supplements that have often been recognized in the past as causes of liver injury worldwide include green tea, aloe vera, kava kava, and, commonly in Asia, traditional Chinese medicine (TCM). A 2021 systematic review defined the most common previously described herbal supplements as Chelidonium majus, Polygonum multiflorum (He-Shou-Wu), Phosphagen, T-bomb II and Cell-tech, TCM, and green as well as black tea [1]. Updates on herbal supplements that have induced liver injury are described in this section.
8.1. Traditional Chinese Medicine
Traditional Chinese medicine (TCM) is a system of medicine drawn from ancient practitioners in China. TCM incorporates a large range of practices based on concepts more than 2000 years old [24]. The philosophical background of the alternative medicinal practice is based on Yinyangism and focuses on life energy, called Qi, and its flow along pathways through the body, called meridians [24]. Today, it is widely used as a complementary alternative medicine (CAM) approach and involves herbal and dietary treatment, moxibustion, acupuncture, acupressure, massage, exercise, and meditation [25]. Common polyherbal Chinese medications implicated in HILI include Gynura japonica (tusanqi), Ba Jiao Lian (Dysosma pleianthum), Bol Gol Zhee (Fructus psoraleae), Chi R Yun (Breynia officinalis), Jin Bu Huan (Lycopodium serratum), Ma Huang (Ephedra), Sho Saiko To, and Shou Wu Pian (Polygonum multiflorum) [11].
8.2. Pyrrolidine Alkaloids
Pyrrolizidine alkaloids (PAs) are hepatotoxic phytotoxins that have been found in various herbal remedies. They can induce liver damage, including hepato-sinusoidal obstruction syndrome (HSOS) or veno-occlusive disease [26]. HSOS is characterized by venous obstruction via damage to the hepatic sinusoidal endothelial cells. Various herbal remedies have been implicated: Tusanqi (Gynura japonica and Gynura segetum), Senecio brasiliensis, Crotalaria, and heliotropes [26,27,28,29,30]. The stems of the Gynura japonica plant have been used in TCM to topically treat trauma injuries and promote blood stasis. The herb has contributed significantly to HILI cases due to the large number of PAs present in the herb.
The hepatotoxic effect of PAs in various herbal supplements was recently evidenced by a review outlining 2214 cases of Tusanqi (G. japonica)-induced HSOS cases in China [26]. While the authors estimated nearly 89% of HSOS in China is due to G. japonica, the review solely comprised case reports and case series from 1980 to 2019, for a total of 2156 cases. The authors note the diagnosis of Tusanqi (G. japonica)-induced HSOS is reliant on the exclusion of other etiologies, and a new blood pyrrole-protein adducts test was used to confirm the diagnosis of 58 additional cases. Limitations of the review include the wide variety of concoctions of the herb, which included powder, tea, liquor concoctions, and steamed root. Further, the duration in symptom onset ranged from 1 day to 20 years.
Other recent case reports have described HSOS after oral ingestion of plants in the same genus of flower, such as Gynura segetum [27,28]. A case study by Barcelos [29] presents a woman who presented with jaundice and signs of portal hypertension with no history or risk factors of liver disease. She reported daily use of Senecio brasiliensis as a homemade tea prescribed for menopause. Senecio brasiliensis is a plant native to the fields of South America and is known to contain PAs. The calculated RUCAM score (Roussel Uclaf Causality Assessment Method) was 6. HSOS diagnosis was confirmed through a liver biopsy.
To establish the diagnosis of PA-induced HSOS, new clinical criteria have been developed by The Hepatobiliary Diseases Committee of the Chinese Society of Gastroenterology [30]. The “Nanjing criteria” are based on the presence of clinical findings (weight gain, hepatomegaly, and ascites) not attributable to any other possible cause. Treatment of PA-induced HSOS is mainly based on avoidance of the agent and anticoagulation and antithrombotic agents. Mortality approaches 40% in those for whom initial therapy fails. Prompt use of Transjugular Intrahepatic Portosystemic Shunt (TIPS) in these patients has been utilized and shown to be effective [31].
8.3. Ayurveda
Ayurvedic medicine is an ancient Indian medical system that originated in India more than 3000 years ago. The primary basis of Ayurvedic medicine centers on ancient writings that designate a holistic approach to physical and mental health [5]. Ayurveda remains a major form of medicine in India today and many consider it to be equivalent to Western medicine. Many Ayurvedic treatments combine products that have not been thoroughly studied. Given the combination of multiple materials and often incomplete labeling, it is difficult to assess HILI due to Ayurvedic compounds. Common HILI ingredients in Ayurveda include Ashwagandha, aloe vera, Guggul, Puncture vine, bakuchi, Indian senna turmeric, Gotu-kola, senna, Noni, Malabar tamarind, brahmi, Gurmar, Indian mulberry, and pyrrolizidine alkaloids. One such material is Withania somnifera (Ashwagandha) [11]. We discuss a few examples of Ayurveda-induced liver injury below.
8.4. Ashwagandha
Ashwagandha is derived from the roots of the Withania somnifera species and is known to have as many as 35 different chemical constituents [32]. Its main active ingredients comprise alkaloids, steroidal lactones, and saponins [33]. Despite causing gastrointestinal side effects, ashwagandha has obtained widespread use. Recently, associations with HILI have been reported.
Weber et al. [34]. described a man with no previous medical history who consumed ashwagandha extract (500 mg) daily for more than a year before he switched to Ashwagandha Now (ashwagandha 450 mg; Now Foods, Bloomingdale, IL, USA) [34]. Twenty days later, he experienced pruritus and jaundice. The HILI was attributed to Ashwagandha Now with a RUCAM score of 6. In reviewing the main websites selling Ashwagandha Now, eleven subjects reported liver damage and 107 reports of severe pruritus were noted [34]. This case was typical of previous cases of ashwagandha-induced liver injury wherein the liver injury presented up to 12 weeks after consuming ashwagandha and generally presented with a cholestatic or mixed picture of injury [35]. One case report described a hepatocellular pattern of liver enzyme abnormality with a liver biopsy that showed an acute cholestatic hepatitis with confluent necrosis [36]. While these authors report that Ashwagandha Now HILI cases are described in reading the website, they are anecdotal self-reported events that have not been assessed via RUCAM score or other causality methods. In the previous case report, the recorded dose was an estimate with the possibility of recall bias, and a toxic dose could not be calculated.
8.5. Turmeric/Curcumin
Curcumin is a bright yellow substance found in turmeric, a member of the ginger family, Zingiberaceae. As a dietary supplement, it has been advertised as being an anti-inflammatory and antioxidant agent due to its potent inhibition of NF-κB activation and inhibition of TNF-mediated actions [37]. Turmeric has been used in Ayurvedic medicine to treat many conditions. Indeed, turmeric and curcumin are under active investigation for a wide variety of disease states, including NASH and hyperlipidemia. The evidence to date indicates, however, that the purported effects of turmeric are not well established, and rigorous studies are lacking [38]. Further, although the safety of turmeric and curcumin has been well established, recent reports of isolated cases of HILI have been noted. Koenig et al. [39] described a 53-year-old woman who developed jaundice after a month-long use of a combination herbal “liver-cleansing” compound and a nightly herbal “sleep aid.” The “Liver Detoxifier and Regenerator” listed turmeric root as one of its many ingredients. The “Restful Sleep” aid listed multiple constituents, including valerian. The patient’s hyperbilirubinemia and liver enzyme elevations were indicative of cholestatic jaundice and resolved after discontinuation of the product. Notably, the amount of turmeric root in the polyherbal supplement was not provided nor was the amount consumed by the patient. Additionally, the concentrations of the other additives or components that could be present in the formulation, such as impurities and contaminants, were not reported.
Notably, certain natural compounds have also been used to increase the bioavailability of curcumin. Piperine, the main component of black pepper, increases the bioavailability of curcumin by increasing its rate of absorption by 2000% at 45 min after co-administering curcumin orally with piperine [40]. The biological activity of formulated curcumin has been postulated to be associated with HILI cases and linked to outbreaks of acute hepatitis in Italy [41]. Although there have been fewer than 40 cases in the literature, a recent case series adds to the numbers. Sohal et al. [42] describe two middle-aged females with no past medical history who developed a hepatocellular pattern of injury after taking turmeric as an over-the-counter medication and as a food supplement. In one case, the patient reported taking the over-the-counter supplement containing turmeric 2000 mg and black pepper daily for three months for back pain [42]. The authors reported the cases had RUCAM scores of 7 and 6, respectively. Another recent turmeric and piperine supplement-induced liver injury case was reported in a 49-year-old woman admitted with elevated aspartate aminotransferase and alanine aminotransferase with no history of liver disease [43]. The authors sent the supplement for mass spectrometry analysis, which confirmed the curcumin component, albeit less than the label-reported amount. Similar to other reports, the patient presented with hepatocellular injury after a latency period of 1–2 months. The authors reported the case had a RUCAM score of 7.
Most recently, Halegoua-DeMarzio and colleagues from the US DILI Network [4] described 10 well-evaluated cases of liver injury associated with turmeric reported to the registry since 2011. Eight patients were female, who had a median age of 56 years, and nine had hepatocellular injury, with one having mixed injury. Liver biopsies were performed in four patients and showed acute hepatitis or mixed injury with eosinophils. Of five patients requiring hospitalization, one died of acute liver failure, indicating that injury can be severe. The authors performed a chemical analysis on the suspected products and confirmed the presence of turmeric in all samples tested. They noted that three products also contained piperine (black pepper). HLA typing was performed and revealed that seven patients carried the HLA-B*35:01 allele (homozygous in two individuals), which appears to be a risk factor for turmeric liver injury as its frequency was more than six times higher than was seen in a control population (0.45 vs. 0.056–0.069). The authors also reported the incidence of liver injury from turmeric may be increasing as most of the cases were enrolled since 2017.
8.6. Kratom
Kratom, or Mitragyna speciosa, has been increasingly described as a cause of HILI and acts on serotonin and opioid receptors [44]. It is derived from the leaves of a native tree found in Southeast Asia and is composed of alkaloids [45]. However, its use has become more prevalent within the United States in the past few decades and it has become a safety concern in the recent years due to its possible severe side effects of hepatotoxicity, seizures, hallucinations, delusions, and even death when used to ameliorate the effects of opioid withdrawal. From 2014 to 2019, approximately 3500 cases of kratom-induced injury were reported to the U.S. Poison Control Centers [46]. Per the United States Drug Enforcement Administration (DEA), the kratom leaves are crushed and then can be consumed by smoking the leaves, ingesting in tea or as powder, or placing into gel capsules. Lower doses are known to cause stimulant-like effects and higher doses are reported to cause sedative effects. It has been identified as an addictive substance and classified as an opiate by the FDA, and is cited by the DEA as a “Drug and Chemical of Concern” [47]. There are various street names synonymous with kratom including thang, kakuam, thom, ketum, and biak.
The two major ingredients are mitragynine and 7-hydroxymytragynine. It is found to be primarily metabolized in the liver and can be tested via a mitragynine urine test [44,45]. Hepatic injury has been reported to have an average latency period of 21 days but has a wide range of onset from the time of ingestion [44]. Kratom is also commonly used for pain management, improving fatigue, and utilized for mood disorders while inducing euphoria. An October 2022 study performed a review of public responses to the US FDA inquiries into kratom in order to provide a more comprehensive understanding of kratom [48]. The results found that any reports of overdoses or deaths related to the consumption of kratom were limited to Western countries and had not been published in Asia.
Indeed, in the United States, one analysis found that concomitant use of kratom with other medications, including sedatives, was more prevalent compared to that in Thailand [46]. Adverse reactions with the use of kratom have been reported to occur at a rate of 21.9% in those over age 60 compared to 12.3% of the time in those who are younger. In the United States, kratom possession, sale, and use have been banned in Alabama, Arkansas, Indiana, Tennessee, Vermont, and Wisconsin. Other states have created regulations for access to kratom, but in the majority of the United States, kratom sale and consumption are unregulated [48]. It has also been banned by several countries worldwide. It is not approved for medical use by the US FDA but remains “legal” in the rest of the United States. The DEA was in the process of listing kratom as a Schedule I Controlled Substance, but it currently remains unregulated and uncontrolled by the US FDA. It is available for purchase online and with individual vendors in states where the law does not prohibit its sale and it can be marketed as having “therapeutic” effects.
Among the more recent reports of kratom-associated liver injury, Khan et al. described a 37-year-old female who was found to have multi-organ injury secondary to kratom use, involving both hepatocellular and cholestatic liver injury confirmed with liver biopsy, along with acute kidney injury and pancolitis. Typically, when described previously, kratom was not commonly observed to cause damage to multiple organs simultaneously, but liver injury and kidney injury have been observed separately. In this case, the patient ultimately required an orthotropic liver transplantation with a Model for End-Stage Liver Disease-Sodium score (MELD-Na) of 36. Another case report by Jensen et.al. discussed a case of a 38-year-old male who had a long history of ingesting kratom along with a history of alcohol and opiate use disorder who was found to have transaminitis 31 days from kratom ingestion in the setting of a positive mitragynine urine test [45]. This case describes new acute liver injury in a patient with extensive prior use of kratom, but no prior history of associated liver injury. However, this case highlights the difficulty of determining an etiology of acute liver injury as this may have been multifactorial in the setting of a known prior alcohol use disorder. In these cases, all other etiologies for liver injury were thoroughly ruled out. Recently, kratom has been reported to be a potential cause of bile duct injury due to damage to bile duct epithelium or cholangiocytes, and should be considered as a precursor when evaluating etiologies of cirrhosis [49].
8.7. Green Tea Extract
Green tea extract has been reported to cause acute liver injury and even liver failure. These cases are typically seen when green tea extracts are taken for weight loss and as dietary supplementation. The extract is used for various other reasons in order to improve overall health, including preventing cancer, decreasing lipid levels, increasing weight loss, and more [50]. In the updated AASLD practice guidelines, Fontana et al. describes that a strong association has been identified between green-tea-extract-induced liver injury and HLA-B*35:01, thought to be due to the polyphenolic catechins, which are the active component [3].
A retrospective study published by Fallah et al. evaluated whether drinking green tea as compared to ingesting green tea extract supplements would lead to abnormal liver tests [51]. Their study determined that there was no statistically significant association between abnormal liver enzymes and consuming green tea and there was even a statistically significant reduction in liver enzymes with consumption of green tea by itself. This study was conducted with a large sample size of approximately 24,000 persons, half of whom consumed green tea extract supplements and the other half green tea itself. However, the authors did not refute the possibility that green tea supplements can lead to cases of HILI and note that there is still a risk, although it was not statistically significant.
8.8. Garcinia cambogia
In the past, multiple reports have described significant liver injury in patients consuming Garcinia cambogia [5]. Hydrocitric acid has been identified as the main active ingredient in Garcinia. Zovi et al. reviewed the use of herbal supplements in association with weight loss [52]. They reviewed reports from the European Food and Drug Administration ranging from 2009 to 2021 and found cases that supported an association between hydrocitric acid and hepatoxicity.
In the US DILIN registry, Vuppalanchi et al. reviewed 1418 cases of liver injury recorded from 2004 to 2018 and 5 cases were identified where Garcinia cambogia alone was implicated in causing liver injury, 16 with Garcinia cambogia combined with green tea, and 1 case with Garcinia cambogia and Ashwagandha [53]. All 22 patients were diagnosed with hepatocellular injury and there no clinically significant differences in the liver injury sustained by Garcinia cambogia alone versus being given in combination with green tea. In addition, the authors observed that those patients with acute liver injury who consumed supplements with Garcinia cambogia had a statistically significant higher probability of having the HLA-B*35:01 allele when compared to those who used other supplements.
8.9. Black Cohosh
Black cohosh (Cimicifuga racemosa) is an herbal supplement known to result in liver injury. A recently reported case by Brar et al. [54] described a 50-year-old female patient who presented with a two-month history of jaundice, malaise, and pruritus and was found to have elevated total bilirubin and alkaline phosphatase, which are concerning for cholestatic liver injury [54]. In this case, she was consuming black cohosh to improve her postmenopausal symptoms. Once the supplement was discontinued, her liver enzymes returned to normal after six months. The mechanism for causing liver injury from this agent has not been confirmed, but immunologic mechanisms are favored, and some cases have presented with autoimmune features (LiverTox). The incidence of overt hepatic injury from black cohosh would appear to be very low based on the findings of Castelo-Branco et al. [55], who did not find any evidence of hepatotoxicity in their literature review of studies containing more than 13,000 women treated with isopropanolic black cohosh extract for neurological and psychological menopausal symptoms. However, the degree to which liver injury was evaluated was not stated.
8.10. Polygonum multiflorum (He-Shou-Wu or Reynoutria multiflora)
Polygonum multiflorum, also known as He-Shou-Wu or in Latin as Reynoutria multiflora, is an herbal supplement that originates in China and has been used for a multitude of proposed health benefits including, but not limited to, kidney health, decreasing lipid levels, slowing of aging, preventing cancer, anti-inflammatory effects, and improving cognitive function [56]. It was first reported to cause liver injury in 1996 in Hong Kong and reports have has since been made worldwide. It has even been utilized to improve liver function [56]. Anthraquinone and stilbene compounds have been identified as the main components of Polygonum multiflorum that result in liver injury. Despite the abundance of cases over the past 25 years, the mechanism of injury is still actively being investigated. In the past year, a study conducted by Hu et.al. identified 2,3,5,4′-tetrahydroxy stilbene glycoside (TSG) and emodin (EM), both compounds found in the dried root of Polygonum multiflorum, as the main causes of Polygonum-multiflorum-induced liver injury [57]. The most widely described pattern of liver injury is hepatocellular, but cases of mixed hepatocellular and cholestatic liver injury have been reported. Further review this past year, as described in Zhai et al., concludes that liver injury from Polygonum multiflorum occurs via multiple simultaneously occurring mechanisms including inflammatory, apoptosis, and bile acid metabolism disorders, and changes in enzymes that metabolize drugs [58]. The main identified risk factors for liver injury are those patients with mild immune stress and/or genetic polymorphisms. Rao and colleagues suggested that the mechanism of liver injury is likely immune-mediated [59].
9. Newly and Recently Described Herbal Hepatotoxins
9.1. Aristolochia and Asarum
Aristolochic acids (AAs), which arise from Aristolochia and Asarum plants, have been implicated previously as a cause of hepatoxicity. This class of compounds is typically known to cause nephrotoxicity and has even been associated with urothelial carcinoma; however, there are increasing investigations into the association of aristolochic acids with liver injury as well as hepatocellular carcinoma. Exposure of this herbal product to humans arises from soil pollutants which can accumulate in the human body over time leading to fibrosis. Aristolochic cids have been studied mostly in animal studies. A prior study by Lu et al. identified a dose-dependent association of AA with the development of liver fibrosis and mutations causing hepatocellular carcinoma in mice [60]. The authors also retrospectively reviewed the AA-mediated mutation in human liver cancers from mainland China, Taiwan, Hong Kong, Singapore, Korea, Japan, and France. They found that 133 of the 510 (26%) samples of HCC from China contained an AA mutation along with 68 of 98 (69%) samples from Taiwan. In Japan and France, less than 1% of the HCC contained AA mutations. The study concluded that Asian patients had a higher chance of an AA-mediation mutation identified in their HCC compared to non-Asian patients.
Although the association between AA and hepatoxicity has been established, there is still a knowledge gap in the mechanism of injury. Luo et al. assessed the potential mechanism of AA-induced hepatoxicity and hepatocellular carcinoma in mice models [61]. Their study was conducted utilizing single-cell RNA sequencing and proteomic techniques and determined that aristolochic acids do cause hepatotoxicity in mice by activating apoptosis pathways.
9.2. Tinospora cordifolia (Giloy)
The COVID-19 pandemic has seen a variety of herbal and complementary therapies promoted as having promising inhibitory effects against coronavirus [62,63]. Polyherbal Ayurvedic compounds and alternative medicine therapies have been widely employed, one of which is Tinospora cordifolia (Giloy), promoted as an “immune booster” and as prophylaxis against COVID-19 [62,63]. T. cordifolia, commonly named “Guduchi”, is a common herb used in the treatment of various diseases in the traditional Ayurvedic literature. However, several reports have recently shown an association between Giloy use and drug-induced autoimmune hepatitis (AIH). In their case series, Nagral et al. described the hepatic injury of Tinospora cordifolia [64]. According to the authors, Tinospora cordifolia may stimulate the immune system to reveal underlying autoimmune liver disease. Tinospora cordifolia may also induce an immune response to a reactive metabolite acting as a hapten, causing an immunoallergic type of HILI. In their published case series, six patients presented with symptoms of acute hepatitis after consumption of Tinospora cordifolia. The average duration of consumption was 90 days. These patients had autoimmune-like injury features on biopsy, and most had underlying chronic liver disease of likely autoimmune etiology. One patient died of liver failure, whereas the others recovered fully.
Several limitations of this study have been cited, including the fact that T. cordifolia (TC) has been consumed extensively in India for general health purposes with a well-documented history of safety [65], RUCAM scoring is not very reliable in chronic liver disease [66], the variety of Tinospora consumed was not specified [67,68], Tinospora cordifolia has been reported to prevent hepatotoxicity (whereas Tinospora crispa may be hepatotoxic) [69], and polyherbal consumption was present [67]. Parikh described two females who consumed Tinospora cordifolia capsules for its alleged immune boosting effect against COVID-19, and who presented with jaundice [70]. A subsequent liver biopsy showed lymphocytic infiltration. Other cases included daily consumption of homemade extract of Tinospora plant stem for 4 weeks prior to the development of jaundice and ascites [71]. Rastogi et al. described the use of Giloy preparations in high doses for the treatment COVID [72]. Similarly, Sahney et al. reported three cases with findings similar to Nagral et al. [73]. Gupta et al. reported two additional cases, one in which a 39-year-old female with no comorbidities presented with jaundice after consuming Tinospora cordifolia plant twigs boiled with water once every three days for one month with subsequent liver biopsy consistent with autoimmune-like HILI [74].
Given the growing number of Giloy cases, others have suggested the need for multicenter studies with this agent [75]. Indeed, a recent Indian multicenter retrospective observational cohort study by Kulkarni et al. [76] reported a total of 43 patients with documented Giloy consumption who demonstrated Giloy-induced liver injury. The authors reported Giloy was ingested as part of a multiherbal concoction or in its pure form. The RUCAM score was used to diagnose HILI with liver injury, which was found to be possible in 14 of the participants and probable in 29. Autoantibodies were found in 30% of patients. Half of the patients underwent liver biopsy with features consistent with a mixed pattern of inflammation with cholestasis. The reported outcomes included four patients who died and two patients who underwent liver transplantation. The rest of the cohort recovered fully within 6 months from presentation. The amount of Giloy was found to be variable, with an unknown quantity in 11 patients and a mean intake in the remaining patients of 40.8 ± 19.7 mL a day. The effect of multiherbal concoctions on liver toxicity in relation to Giloy as a cause is not known, although the authors did conduct an herbal analysis to rule out other known hepatotoxic components on six drug samples. As a result, the authors concluded that their study confirmed a pattern of herb-induced hepatitis with autoimmune features due to Giloy use.
9.3. Horse Chestnut
Horse chestnut (also known as Aesculus hippocastanum) grows on a tree indigenous to Persia and Eastern Asia. The horse chestnut fruit contains seeds that look like a chestnut. However, the raw seeds and flowers of horse chestnut are unsafe due to a toxic component known as escin and its glycoside esculin. In horse chestnut seed extract, the toxic saponin component has been removed. Standardized horse chestnut seed extracts (HCE, escin) are commonly promoted and used for chronic venous insufficiency (CVI), joint pain, and bladder and gastrointestinal problems. The active component of HCE, escin, stimulates release of prostaglandins that promote venoconstriction [77]. Due to this property, HCE has been shown to improve edema in those with CVI and has been studied as an alternative to compression stockings [78]. Few side effects have been reported, along with even rarer instances of HILI. The last prior case reported was in 1996. More recently, however, a case series by Santos et al. described three cases of liver injury attributed to the use of horse chestnut within 4–8 weeks of onset of liver injury [79]. In all three cases there was resolution of symptoms and normalization of biochemical liver abnormalities when the horse chestnut was stopped. However, in one of the cases, the patient presented with jaundice after re-introduction of the horse chestnut supplement. Since the case series did not describe the use of RUCAM or any causality method, it remains difficult to determine any direct causality.
9.4. Tara Flour
Tara is a legume in the bean family grown in Peru and other Latin American countries. Recently, a popular meal kit product containing tara four was recalled from the US market due to hundreds of consumers reporting a gastrointestinal-like illness shortly after consuming the product [80]. The manufacturer, Daily Harvest, voluntarily recalled all French Lentil + Leek Crumbles due to consumer reports, linking the product to nearly 400 reported cases of gastrointestinal illness and impaired liver function. From 28 April to 17 June 2022, approximately 28,000 units of the recalled product were distributed to consumers in the continental United States through online sales and direct delivery. The most recent FDA report on tara flour [80] outlined various symptoms, including a gastrointestinal illness, such as vomiting in 54 out of the 393 illnesses recorded; diarrhea in 24/393; nausea in 99/393; fatigue, body aches, fever, and elevated liver enzymes (in 193/393); jaundice in 23/393; and liver damage. Some adverse event reports also resulted in gallbladder removal. Two cases outlined had liver biopsies. The report noted one liver biopsy showing “liver-mixed portal and lobular inflammation with prominent portal eosinophils in keeping with injury secondary to drug/herbal supplements” and the second liver biopsy showing “bland cholestasis, [with] no evidence of acute cholangitis or significant ductular reaction. The differential includes drug-induced cholestasis” [80].
While the cause of this outbreak is unknown, preliminary investigations have suggested that the tara flour used in this product was the source of the adverse health outcomes. As of 18 October 2022, there were 393 adverse illness reports in 39 states with 133 hospitalizations but no deaths. The product samples tested negative for mycotoxins and microbes including Salmonella spp., Listeria spp., Hepatitis A virus, and norovirus. The FDA report concluded that the tara flour in the Daily Harvest French Lentil and Leek Crumbles was the postulated source of 393 illnesses, “however, a definitive source or single point of contamination was not identified”.
9.5. Alkaline Water
A case series by Berk et al. describes alkaline water as an etiology of liver injury [81]. Alkaline water has a higher pH than regular tap water and is used to reportedly lower acidity levels and improve hydration. Since 2021, 11 probable cases have been reported by the US Food and Drug Administration, Centers for Disease Control, and Southern Nevada Health District [81]. The consumption of alkaline water has become increasingly popular and touted to provide health benefits, and the product is mostly sold through online retailers. Four cases were described in adult patients diagnosed with acute liver failure in the setting of alkaline water use, all with varying degrees of use [81]. Two of the patients had ingested alkaline water for two to three years prior to presentation. Only one of the patients described a history of heavy alcohol, but otherwise none of the other patients had any significant comorbidities.
According to the CDC, five cases of acute liver failure have been reported in children under 5 years of age and the only common consumption identified among the patients was “Real Alkalized Water” brand bottled water [82]. These cases led to an extensive investigation across multiple states within the United States, which uncovered an additional 21 adults with likely cases of acute liver injury or failure secondary to consumption of this supplement. Most of these patients recovered from their liver injury. However, because of these findings, the company overseeing the manufacturing of this bottled alkaline water began a recall on their products in 2021. Nevertheless, these cases bring into question whether it was specifically the brand identified leading to acute liver injury in these patients or whether it was the alkaline water itself. There were also varying degrees of consumption among these reported cases, so it is unclear what volume of alkaline water may have produced these hepatic effects. No RUCAM score or other causality method was reported in the article, so the veracity of the relationship cannot be confirmed at present.
9.6. Elderberry (Sambucus Species)
Elderberry is an herbal supplement that has been described to help treat respiratory illnesses in the past. Studies have found that ingestion of elderberry can increase the body’s production of inflammatory cytokines. A recently published case by Ramachandran et al. described a female patient of middle age who consumed elderberry supplements and was found to have autoimmune hepatitis [83]. The authors concluded that elderberry consumption may have led to an unspecified liver injury through a genetic mechanism and molecular mimicry. However, the article failed to describe the exact mechanism of causality for this presentation and did not report a RUCAM score. There is still much to be understood about the effects of elderberry and whether it may possibly lead to the presentation of autoimmune hepatitis [83].
10. Updates in HILI Biomarkers
Given the widespread usage of a variety of herbal supplements, developing the ability to identify risk factors for herbal-induced liver injury is an important goal. Zhang et al. pursued this with a prospective analysis of Polygonum multiflorum, analyzing 33 serum cytokines before and after polygonum ingestion [84]. There were multiple elevated cytokines in the susceptible group, most significantly TNF-alpha, which correlated with elevated ALT levels. Changes in these biomarkers were compared between the susceptible group (six patients who developed elevated ALT) and the tolerant group (fifteen patients who had no such elevation) [84]. Interestingly, the authors also discussed the application of Polygonum multiflorum to murine models pre-treated with TNF-alpha, which caused hepatoxicity. In mice without this pre-treatment, no hepatoxicity was seen [84]. While these data are of interest, applying this model to other causes of HILI is eagerly awaited.
11. Newly Described Hepatoprotective Herbal Supplements
In addition to identifying products that result in liver injury, significant research is being undertaken to identify cytoprotective and hepatoprotective herbal products that can treat and prevent liver injury. To date, most investigative studies have been conducted in animals, although there are several important human cell culture trials. Tunera diffusa and Baqi Lingmao have been studied in both animal and human liver cells, as discussed below. However, past and current human studies investigating reported hepatoprotective herbal supplements are largely lacking (Table 5).
11.1. Turnera diffusa
Turnera diffusa, also known as Damiana, is a shrub native to Texas, Mexico, the Caribbean, and Central and South America that has been promoted as an aphrodisiac with stimulant and antidepressant qualities. It has recently been found to also possess hepatoprotective properties. Studies have been primarily conducted in animal models. A study by Rodriguez-Rodriguez et al. studied the effect of Tunera diffusa on human stellate cells and determined that the likely mechanism of hepatoprotection arises from apoptosis resulting from SNAI1 expression, which reduces fibrotic and mitochondrial markers [85].
A recent study by Delgado-Montemayor et al. evaluated whether this herbal supplement might be the key to developing a drug that would produce hepatoprotective effects [86]. According to the authors, the methanolic extract of Turnera diffusa from Mexico was found to be hepatoprotective in in vitro models by producing an anti-fibrotic effect. Furthermore, this study identified that the metabolite hepatodamianol produced significantly (p < 0.02) lower AST and ALT elevations in vitro when compared to the control, carbon tetrachloride. Hepatodamianol was found to be responsible for the hepatoprotective effects of Tunera diffusa. When comparing the Turnera diffusa extract to silymarin both in vitro and in vivo, similar hepatoprotective effects were found. While further research is ongoing that may potentially lead to the development of a hepatoprotective drug using this metabolite, much is still left to be understood about the long-term effects of Turnera diffusa in humans.
11.2. Baqi Lingmao Formula
The water extract of Baqi Lingmao formula, which is composed of ten herbal supplements, was investigated this past year for its utility in the management of liver disease. A study by Liu et al. evaluated the effects of this extract on mice models as well as human liver cells [87]. They found that the Baqi Lingmao formula did improve liver function with reductions in the ALT and AST levels by decreasing inflammatory cell infiltration into the liver, as well by blocking inflammatory cytokine secretion of interferon-γ, tumor necrosis factor-α, and interleukin-6. When tested in human liver cells, the formulation resulted in the production of new hepatocytes and the prevention of hepatocyte death. It was also noted that this agent also decreased the secretion of hepatitis B serum antigen and hepatitis B e antigen. Their findings support the conclusion that the use of the water extract of Baqi Lingmao formula may provide protection to the liver both in vitro and in vivo, providing a potentially promising hepatoprotective agent. Additional studies of its effects in human subjects are awaited.
11.3. Zornia diphylla (L.) Pers.
Zornia diphylla (L.) Pers. is an herbal supplement that has been historically consumed in China and is being investigated for its potential hepatoprotective properties. A study by Xie et al. investigated the use of the herb in liver injury caused by carbon tetrachloride [88]. They performed this experiment on mice models, administering a control group versus multiple concentrations of Zornia diphylla (L.) pers for a total of fourteen days. The data revealed that when treating with Zornia diphylla (L.) pers at any concentration, there was evidence of significant hepatoprotection and decreased inflammatory cells. The likely mechanism proposed to prevent liver injury was postulated to be due to antioxidant properties, reduction in release of inflammatory molecules, and promotion of hepatocyte repair, though the exact process was not identified. To date, however, there have been no major studies investigating its effects on human liver cells.
11.4. Herbal Prevention of Acetaminophen and Other Drug Hepatotoxicity
While N-acetylcysteine remains the mainstay of treatment for acute acetaminophen overdose, significant research efforts continue into the prevention of liver injury using natural products, as recently reviewed by Liao and colleagues [89] and Chilvery et al. [90]. Mahmoudi et al. reviewed the recent literature regarding the use of a variety of natural products in the prevention of liver injury from doxorubicin [91] The interested reader is referred to these and other reviews describing efforts in this particular area.
12. Gut Microbiome and Liver Injury
Several investigators have reported the potential hepatoprotective effects of modulating the intestinal microbiome. For example, Meng and colleagues reviewed the strategy of targeting the gut microbiota with a variety of natural products to reduce oxidative stress, suppress inflammation, prevent fibrosis, and decrease apoptosis in the prevention of liver injury [92]. Chu et al. described the ability to reverse dysbiosis and prevent drug-induced liver injury through probiotics, fecal transplant, and other measures [93]. Guo and colleagues examined the hepatoprotective effects of Lactobacillus paracasei CCFM1222 against acute liver injury induced by lipopolysaccharide (LPS) in a mouse model [94]. Mice pre-treated with this strain of lactobacillus showed lower ALT and AST levels and had inhibition of various cytokines associated with hepatotoxicity, including TNF-α, IL-1β, and IL-6 levels. Treated mice saw alterations in their microbiome composition to higher levels of Faecalibaculum and Bifidobacterium and lower levels of Prevotellaceae. Such modulation of the gut microbiome is currently a major area of research to identify natural means of preventing and/or treating HILI as well as DILI.
13. Updates on HILI Treatments
Ongoing research is being conducted to identify improved treatments for cases of acute DILI and HILI that do not recover quickly, apart from emergency liver transplantation for acute liver failure. The 2022 AASLD guidelines note that the mainstay of current treatment for DILI and HILI remains supportive care, such as hydration, antiemetics, and pain medications as needed, and discontinuing use of the offending agent [3]. The 2021 ACG guidelines added that the best approach to management of HDS-induced hepatotoxicity is to have a high index of suspicion for use of HDS when evaluating a patient [18]. However, there are more targeted therapies being utilized for specific drugs and HDSs causing HILI, as described by Fontana et al. in the updated AASLD guidelines. For example, silymarin in combination with dialysis has been used in hospitalized patients with liver injury or in acute liver failure secondary to amanita mushroom toxicity to help remove the associated enterohepatic toxin. N-acetylcysteine (NAC) can also be utilized for a short course in adults with liver injury but may or may not provide a benefit. Corticosteroids have also been described as a possible intervention, but statistically significant efficacy has not been proven due to lack of randomized controlled trials.
Several recent studies have been published reviewing the efficacy of corticosteroids plus glycyrrhizin, traditional Chinese medicine (TCM), and silymarin in the management of HILI/HDS, as discussed in further detail below.
13.1. Corticosteroids with Glycyrrhizin
A randomized study investigated the effectiveness of corticosteroids plus glycyrrhizin (the active ingredient in licorice) for the treatment for chronic DILI or HILI [95]. Eighty participants were identified with a RUCAM score of greater than or equal to 6 (“probable” cause) and were divided into a control group versus a treatment group with a 48-week taper of methylprednisolone and glycyrrhizin. Traditional Chinese medicine (TCM) was the HDS considered casual in this study, including Polygonum multiflorum Thunb. (Heshouwu), Corydalis yanhusuo W. T. Wang (Yanhusuo), Psoralea corylifolia L. (Buguzhi), Bupleuum chinense DC. (Chaihu), Dictamnus dasycarpus Turcz (Baixianpi), and Terminalia chebula Retz. (Hezi). A pre-treatment liver biopsy was obtained in 78 of the initial patients and demonstrated inflammatory necrosis and fibrosis of different degrees. Ultimately, 35 participants were treated with steroid plus glycyrrhizin (treatment group) and 35 were placed in the glycyrrhizin monotherapy group (control). An improved biochemical response was seen in the treated group. A post-treatment liver biopsy was obtained in 32 patients in the steroid plus glycyrrhizin monotherapy group and 12 patients in the glycyrrhizin control group. These results showed a significant improvement in fibrosis in the steroid treatment group compared to the controls, where no improvement in fibrosis was seen.
While this study provides support for the use of corticosteroids with glycyrrhizin for the TCM agents discussed above, it is limited by its relatively small sample size. In addition, it does not describe how this treatment is affected by comorbid conditions or if it would be beneficial in a case of acute liver injury.
Yang and colleagues reported that glycyrrhizin was hepatoprotective in a mouse model when administered with diosbulbin B (DIOB), the purported component of Dioscorea bulbifera L. responsible for liver injury [96]. This herbal agent is used for the treatment of thyroid disorders in China and has been associated with severe liver injury, which has limited its use [97]. Yang et al. postulated that glycyrrhizin protects against the hepatotoxicity of this compound by inhibiting CYP3A4 and subsequently reducing the formation of pyrrole-glutathione conjugates by inhibiting the metabolic activation of DIOB.
13.2. Silymarin (Milk Thistle)
Silymarin, or milk thistle, is a mixture of flavonolignans, and has been previously described as a hepatoprotective agent used to treat liver diseases of varying etiologies, although no definitive clinical effects have been determined according to a recent review [98]. Ongoing studies are being conducted to investigate the mechanisms and long-term effects of silymarin on hepatic injury. The most active ingredient found in silymarin is silybin and, while not regulated or recommended for use by the US FDA, it is described as an antioxidant, anti-inflammatory, and antifibrotic agent. Silymarin has been found to block free radical formation and has been described as an iron chelator. Studies have shown that silymarin can decrease expression of COX-2 and the NF-kb controlled pathway, which are both involved in the production of inflammation. With regard to its antifibrotic properties, silymarin has been found to decrease platelet-derived growth-factor-induced DNA synthesis and TGF-B, thus reducing liver fibrosis and disease progression [98]. It is available in capsule, tablet, or liquid form and comes in various doses. While it has been reported to cause possible gastroenteritis, headaches, pruritis, hives, and rashes, no reports of liver injury have appeared.
Aschufusi et al. described recent studies using varying doses of silymarin in the management of acute and chronic liver diseases, including nonalcoholic fatty liver disease (NAFLD), with improvements in insulin resistance and lowering fasting insulin levels. It has also been reported for use in treatment of liver injury induced by Amanita mushroom toxicity [98,99]. However, specific use of silymarin to treat HILI has not appeared to our knowledge.
14. Conclusions
HILI continues to increase in incidence in the United States and globally. With the rise of social media and its ability to propagate unreviewed information, an ongoing pandemic, and increasing hesitancy when it comes to medical interventions, including well-studied medications and vaccines, many individuals throughout the world are turning to complementary and alternative medicines to treat various ailments and illnesses. Despite the appeal of such “natural product” medications, in reality there is significant risk inherent in their use, a risk that is incompletely understood. While there continues to be a lack of regulation of herbs and HDSs in comparison to other drugs by the US FDA, legislation proposed in April 2022 would require companies to provide the FDA with a list of ingredients, allergens, and any warnings associated with consumption of the supplement. However, this legislation has still not been passed, and even if enacted, it still would not allow the FDA to regulate the sale of any of these products. Nevertheless, it would provide the public with more access to information, allowing them to educate themselves about the potential side effects before use. In the past 2 years alone, the FDA issued at least five warnings to multiple companies for illegally marketing herbal supplements claiming to treat infertility, mental illness, diabetes, and cardiovascular disease, for example. However, states and various jurisdictions can place their own regulations on certain products if deemed appropriate. Kratom, for example, has been banned in six states in the US and is regulated by some, although it remains legal within the rest of the United States despite its questionable safety profile and concerns regarding its addictive properties. The methodology for diagnosing HILI remains challenging, with RUCAM scoring and expert opinion being the most widely utilized. Many herbal and dietary supplements and herbal-derived medications have been shown to cause liver injury, from traditional Chinese medicine and Ayurveda to green tea and black cohosh, though there are select herbs—Turnera diffusa, silymarin, and zornia—that have recently been shown to also potentially have some protective effects, mostly in animal studies. Newly suspected HILI agents continue to be identified, including horse chestnut and tara flour. Alkaline water, widely available and popularized by various forms of media and advertisement, has also now been shown to cause HILI in a few documented cases. A recent study to identify HILI biomarkers demonstrated multiple cytokines, including TNF-alpha, that are associated with herbal injury. HLA-B*35:01 may be an important genetic marker for liver injury due to turmeric. All these areas in the field of HILI deserve further study and investigation, as much remains to be discovered. Regarding treatments for HILI, both ACG and AASLD guidelines recommend removal of the offending agent and provision of supportive care, although more clinically efficacious targeted therapeutic approaches are still being investigated, including the use of NAC and corticosteroids. Indeed, one small study has demonstrated the potential of employing the combination of methylprednisolone and glycyrrhizin in treating HILI. Finally, the role of the gut microbiome in preventing and/or treating HILI (as well as DILI) remains an active area of investigation based on current study results.
Author Contributions
Conceptualization: P.A.P.-R. and J.H.L.; Methodology: P.A.P.-R., L.C. and J.H.L.; Validation: P.A.P.-R. and J.H.L.; Resources: P.A.P.-R., L.C. and J.H.L.; Data curation: All authors; Writing—original draft preparation: P.A.P.-R., L.C., D.A., D.T.G., S.M.W. and J.H.L.; Writing—review and editing: P.A.P.-R. and J.H.L.; Visualization: P.A.P.-R., L.C., D.A. and J.H.L.; Supervision: J.H.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Soares, P.F.; Fernandes, M.T.C.F.; Souza, A.d.S.; Lopes, C.M.; dos Santos, D.A.C.; Oliveira, D.P.R.; Pereira, M.G.; Prado, N.M.D.B.L.; Gomes, G.S.d.S.; Santos, G.; et al. Causality imputation between herbal products and HILI: An algorithm evaluation in a systematic review. Ann. Hepatol. 2021, 25, 100539. [Google Scholar] [CrossRef] [PubMed]
- Ballotin, V.R.; Bigarella, L.G.; Brandão, A.B.d.M.; Balbinot, R.A.; Balbinot, S.S.; Soldera, J. Herb-induced liver injury: Systematic review and meta-analysis. World J. Clin. Cases 2021, 9, 5490–5513. [Google Scholar] [CrossRef] [PubMed]
- Fontana, R.J.; Liou, I.; Reuben, A.; Suzuki, A.; Fiel, M.I.; Lee, W.; Navarro, V. AASLD practice guidance on drug, herbal, and dietary supplement-induced liver injury. Hepatology 2023, 77, 1036–1065. [Google Scholar] [CrossRef] [PubMed]
- Halegoua-DeMarzio, D.; Navarro, V.; Ahmad, J.; Avula, B.; Barnhart, H.; Barritt, A.S.; Bonkovsky, H.L.; Fontana, R.J.; Ghabril, M.S.; Hoofnagle, J.H.; et al. Liver Injury Associated with Turmeric-A Growing Problem: Ten Cases from the Drug-Induced Liver Injury Network [DILIN]. Am. J. Med. 2023, 136, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.M.; Davis, W.D.; Aggarwal, S.; Clinton, J.W.; Kiparizoska, S.; Lewis, J.H. Herbal and dietary supplement induced liver injury: Highlights from the recent literature. World J. Hepatol. 2021, 13, 1019–1041. [Google Scholar] [CrossRef] [PubMed]
- Gurley, B.J.; McGill, M.R.; Koturbash, I. Hepatotoxicity due to herbal dietary supplements: Past, present and the future. Food Chem. Toxicol. 2022, 169, 113445. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Gahche, J.J.; Lentino, C.V.; Dwyer, J.T.; Engel, J.S.; Thomas, P.R.; Betz, J.M.; Sempos, C.T.; Picciano, M.F. Dietary supplement use in the United States, 2003–2006. J. Nutr. 2011, 141, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Gahche, J.J.; Miller, P.E.; Thomas, P.R.; Dwyer, J.T. Why US adults use dietary supplements. JAMA Intern. Med. 2013, 173, 355–361. [Google Scholar] [CrossRef]
- Kamarli Altun, H.; Karacil Ermumcu, M.S.; Seremet Kurklu, N. Evaluation of dietary supplement, functional food and herbal medicine use by dietitians during the COVID-19 pandemic. Public Health Nutr. 2021, 24, 861–869. [Google Scholar] [CrossRef]
- Vuppalanchi, R.; Ghabril, M. Review article: Clinical assessment of suspected drug-induced liver injury and its management. Aliment. Pharmacol. Ther. 2022, 56, 1516–1531. [Google Scholar] [CrossRef]
- Teschke, R.; Eickhoff, A.; Schulze, J.; Danan, G. Herb-induced liver injury (HILI) with 12,068 worldwide cases published with causality assessments by Roussel Uclaf Causality Assessment Method (RUCAM): An overview. Transl. Gastroenterol. Hepatol. 2021, 6, 51. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, P.H.; Lucena, M.I.; Fontana, R.J.; Bjornsson, E.S.; Aithal, G.P.; Barnhart, H.; Gonzalez-Jimenez, A.; Yang, Q.; Gu, J.; Andrade, R.J.; et al. A revised electronic version of RUCAM for the diagnosis of DILI. Hepatology 2022, 76, 18–31. [Google Scholar] [CrossRef] [PubMed]
- The Pew Charitable Trusts. Congress Introduces Dietary Supplement Safety Legislation to Protect Consumers. Available online: https://www.pewtrusts.org/en/research-and-analysis/articles/2022/04/27/congress-introduces-dietary-supplement-safety-legislation-to-protect-consumers (accessed on 1 August 2022).
- Veatch-Blohm, M.E.; Chicas, I.; Margolis, K.; Vanderminden, R.; Gochie, M.; Lila, K. Screening for consistency and contamination within and between bottles of 29 herbal supplements. PLoS ONE 2021, 16, e0260463. [Google Scholar] [CrossRef] [PubMed]
- Hudnall, H. Fact check: False claims about the FDA’s authority over dietary supplements circulate online. USA TODAY, 22 October 2022; 1–4. [Google Scholar]
- FDA. Guidance for Industry: Substantiation for Dietary Supplement Claims Made Under Section 403(r) (6) of the Federal Food, Drug, and Cosmetic Act. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/guidance-industry-substantiation-dietary-supplement-claims-made-under-section-403r-6-federal-food (accessed on 21 April 2023).
- FDA. What’s New in Dietary Supplements. Available online: https://www.fda.gov/food/dietary-supplements/whats-new-dietary-supplements (accessed on 19 January 2023).
- Chalasani, N.P.; Maddur, H.; Russo, M.W.; Wong, R.J.; Reddy, K.R. ACG Clinical Guideline: Diagnosis and Management of Idiosyncratic Drug-Induced Liver Injury. Am. J. Gastroenterol. 2021, 116, 878–898. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Rule, J.A.; Hameed, B.; Ganger, D.; Fontana, R.J.; Lee, W.M. Secular Trends in Severe Idiosyncratic Drug-Induced Liver Injury in North America: An Update From the Acute Liver Failure Study Group Registry. Am. J. Gastroenterol. 2022, 117, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Bessone, F.; Hernandez, N.; Tagle, M.; Arrese, M.; Parana, R.; Méndez-Sánchez, N.; Ridruejo, E.; Mendizabal, M.; Dagher, L.; Contreras, F.; et al. Drug-induced liver injury: A management position paper from the Latin American Association for Study of the liver. Ann. Hepatol. 2021, 24, 100321. [Google Scholar] [CrossRef] [PubMed]
- Björnsson, E.S.; Stephens, C.; Atallah, E.; Robles-Diaz, M.; Alvarez-Alvarez, I.; Gerbes, A.; Weber, S.; Stirnimann, G.; Kullak-Ublick, G.; Cortez-Pinto, H.; et al. A new framework for advancing in drug-induced liver injury research. The Prospective European DILI Registry. Liver Int. 2023, 43, 115–126. [Google Scholar] [CrossRef]
- Chirapongsathorn, S.; Chirapongsathorn, S.; Sukeepaisarnjaroen, W.; Sukeepaisarnjaroen, W.; Treeprasertsuk, S.; Treeprasertsuk, S.; Chaiteerakij, R.; Chaiteerakij, R.; Surawongsin, P.; Surawongsin, P.; et al. Characteristics of Drug-induced Liver Injury in Chronic Liver Disease: Results from the Thai Association for the Study of the Liver (THASL) DILI Registry. J. Clin. Transl. Hepatol. 2023, 11, 88. [Google Scholar] [CrossRef]
- Huang, Y.S.; Chang, T.T.; Peng, C.Y.; Lo, G.H.; Hsu, C.W.; Hu, C.T.; Huang, Y.H. Herbal and dietary supplement-induced liver injury in Taiwan: Comparison with conventional drug-induced liver injury. Hepatol. Int. 2021, 15, 1456–1465. [Google Scholar] [CrossRef]
- Zhao, X.; Tan, X.; Shi, H.; Xia, D. Nutrition and traditional Chinese medicine (TCM): A system’s theoretical perspective. Eur. J. Clin. Nutr. 2021, 75, 267–273. [Google Scholar] [CrossRef]
- Murudkar, P.H.; Tambe, M.S.; Chandrasekar, S.; Boddeda, B.; Pawar, A.T. Common Ayurvedic, Chinese traditional and Unani antidiabetic formulations—A review. Front. Pharmacol. 2022, 13, 991083. [Google Scholar] [CrossRef]
- Zhu, L.; Zhang, C.-Y.; Li, D.-P.; Chen, H.-B.; Ma, J.; Gao, H.; Ye, Y.; Wang, J.-Y.; Fu, P.P.; Lin, G. Tu-San-Qi (Gynura japonica): The culprit behind pyrrolizidine alkaloid-induced liver injury in China. Acta Pharmacol. Sin. 2021, 42, 1212–1222. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Wu, Z.; Wang, F.; Shi, L. Hepatic sinusoidal obstruction syndrome after oral intake of Gynura segetum. Asian J. Surg. 2021, 44, 991–993. [Google Scholar] [CrossRef]
- Cen, P.; Ding, J.; Jin, J. Hepatic sinusoidal obstruction syndrome caused by the ingestion of Gynura segetum in a patient with alcoholic cirrhosis: A case report. J. Int. Med. Res. 2021, 49, 0300060520980649. [Google Scholar] [CrossRef] [PubMed]
- Barcelos, S.T.A.; Dall’oglio, V.M.; de Araújo, A.; Cerski, C.T.S.; Álvares-Da-Silva, M.R. Sinusoidal obstruction syndrome secondary the intake of Senecio brasiliensis: A case report. Ann. Hepatol. 2021, 20, 100138. [Google Scholar] [CrossRef] [PubMed]
- Zhuge, Y.; Liu, Y.; Xie, W.; Zou, X.; Xu, J.; Wang, J. Expert consensus on the clinical management of pyrrolizidine alkaloid-induced hepatic sinusoidal obstruction syndrome. J. Gastroenterol. Hepatol. 2019, 34, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Tu, J.; Zhang, H.; Zhang, F.; Zhang, W.; Xu, H.; Yin, Q.; Yang, J.; Han, H.; Wang, Y.; et al. Risk factors of poor prognosis in patients with pyrrolidine alkaloid-induced hepatic sinusoidal obstruction syndrome after transjugular intrahepatic portosystemic shunt. Hepatol. Int. 2021, 15, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Paramadhas, S.; Alagirisamy, R. Ashwagandha. In Leafy Medicinal Herbs: Botany, Chemistry, Postharvest Technology and Uses; CAB International: Wallingford, UK, 2019; pp. 19–26. [Google Scholar] [CrossRef]
- Murthy, M.V.; Ranjekar, P.K.; Ramassamy, C.; Deshpande, M. Scientific Basis for the Use of Indian Ayurvedic Medicinal Plants in the Treatment of Neurodegenerative Disorders: 1. Ashwagandha. Cent. Nerv. Syst. Agents Med. Chem. 2012, 10, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Weber, S.; Gerbes, A.L. Ashwagandha-Induced Liver Injury: Self-Reports on Commercial Websites as Useful Adjunct Tools for Causality Assessment. Am. J. Gastroenterol. 2021, 116, 2151–2152. [Google Scholar] [CrossRef]
- Ashwagandha—LiverTox—NCBI Bookshelf. Available online: https://www.ncbi.nlm.nih.gov/books/NBK548536/ (accessed on 14 February 2022).
- Ireland, P.J.; Hardy, T.; Burt, A.D.; Donnelly, M.C. Drug-induced hepatocellular injury due to herbal supplement ashwagandha. J. R. Coll. Physicians Edinb. 2021, 51, 363–365. [Google Scholar] [CrossRef]
- Peterson, C.T.; Vaughn, A.R.; Sharma, V.; Chopra, D.; Mills, P.J.; Peterson, S.N.; Sivamani, R.K. Effects of Turmeric and Curcumin Dietary Supplementation on Human Gut Microbiota: A Double-Blind, Randomized, Placebo-Controlled Pilot Study. J. Evid. Based Integr. Med. 2018, 23, 2515690X18790725. [Google Scholar] [CrossRef]
- Turmeric. In LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2021.
- Koenig, G.; Callipari, C.; Smereck, J.A. Acute Liver Injury After Long-Term Herbal “Liver Cleansing” and “Sleep Aid” Supplement Use. J. Emerg. Med. 2021, 60, 610–614. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.; Tyagi, A.K.; Aggarwal, B.B. Recent Developments in Delivery, Bioavailability, Absorption and Metabolism of Curcumin: The Golden Pigment from Golden Spice. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2014, 46, 2. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, N.; Crescioli, G.; Maggini, V.; Ippoliti, I.; Menniti-Ippolito, F.; Gallo, E.; Brilli, V.; Lanzi, C.; Mannaioni, G.; Firenzuoli, F.; et al. Acute liver injury following turmeric use in Tuscany: An analysis of the Italian Phytovigilance database and systematic review of case reports. Br. J. Clin. Pharmacol. 2021, 87, 741–753. [Google Scholar] [CrossRef] [PubMed]
- Sohal, A.; Alhankawi, D.; Sandhu, S.; Chintanaboina, J. Turmeric-Induced Hepatotoxicity: Report of 2 Cases. Int. Med. Case Rep. J. 2021, 14, 849–852. [Google Scholar] [CrossRef] [PubMed]
- Sunagawa, S.W.; Houlihan, C.; Reynolds, B.; Kjerengtroen, S.; Murry, D.J.; Khoury, N. Turmeric-Associated Drug-Induced Liver Injury. ACG Case Rep. J. 2022, 9, e00941. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.Z.; Saleh, M.A.; Alkhayyat, M.; Roberts, D.E.; Lindenmeyer, C.C. Multiorgan Dysfunction Related to Kratom Ingestion. ACG Case Rep. J. 2021, 8, e00647. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.N.; Truong, Q.-N.; Jameson, M.; Nadal, C.N. Kratom-induced transaminitis with subsequent precipitated opioid withdrawal following naltrexone. Ment. Health Clin. 2021, 11, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Qayed, E.; Srinivasan, S.; Shahnavaz, N. Sleisenger and Fordtran’s Gastrointestinal and Liver Disease Review and Assessment; Elsevier: Amsterdam, The Netherlands, 2021; p. 352. [Google Scholar]
- Demick, D.S.; Lee, T.T.; Summers, A.T.; El-Mallakh, R.S. Kratom: A growing substance of abuse in the United States. Ann. Clin. Psychiatry 2020, 32, 275–280. [Google Scholar] [CrossRef]
- Tobacyk, J.; Parks, B.J.; Lovelady, N.; Brents, L.K. Qualitative content analysis of public responses to an FDA inquiry on the impact of scheduling changes to kratom. Int. J. Drug Policy 2022, 108, 103817. [Google Scholar] [CrossRef]
- Dobreva, I.; Karagyozov, P. Drug-induced Bile Duct Injury—A Short Review. Curr. Drug Metab. 2020, 21, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Clinical Course and Diagnosis of Drug Induced Liver Disease. In LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2019.
- Fallah, S.; Musa-Veloso, K.; Cao, J.; Venditti, C.; Lee, H.Y.; Hamamji, S.; Hu, J.; Appelhans, K.; Frankos, V. Liver biomarkers in adults: Evaluation of associations with reported green tea consumption and use of green tea supplements in U.S. NHANES. Regul. Toxicol. Pharmacol. 2022, 129, 105087. [Google Scholar] [CrossRef] [PubMed]
- Zovi, A.; Langella, R.; Nisic, A.; Vitiello, A.; Musazzi, U.M. Liver injury and dietary supplements: Does hydroxycitric acid trigger hepatotoxicity? J. Integr. Med. 2022, 20, 473–475. [Google Scholar] [CrossRef] [PubMed]
- Vuppalanchi, R.; Bonkovsky, H.L.; Ahmad, J.; Barnhart, H.; Durazo, F.; Fontana, R.J.; Gu, J.; Khan, I.; Kleiner, D.E.; Koh, C.; et al. Garcinia cambogia, either Alone or in Combination with Green Tea, Causes Moderate to Severe Liver Injury. Clin. Gastroenterol. Hepatol. 2022, 20, e1416–e1425. [Google Scholar] [CrossRef] [PubMed]
- Brar, H.S.; Marathi, R. Case of cholestatic drug-induced liver injury (DILI) associated with black cohosh. BMJ Case Rep. 2021, 14, e240408. [Google Scholar] [CrossRef] [PubMed]
- Castelo-Branco, C.; Gambacciani, M.; Cano, A.; Minkin, M.J.; Rachoń, D.; Ruan, X.; Beer, A.-M.; Schnitker, J.; Zepelin, H.-H.H.-V.; Pickartz, S. Review & meta-analysis: Isopropanolic black cohosh extract iCR for menopausal symptoms—An update on the evidence. Climacteric 2021, 24, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Teka, T.; Wang, L.; Gao, J.; Mou, J.; Pan, G.; Yu, H.; Gao, X.; Han, L. Polygonum multiflorum: Recent updates on newly isolated compounds, potential hepatotoxic compounds and their mechanisms. J. Ethnopharmacol. 2021, 271, 113864. [Google Scholar] [CrossRef]
- Hu, Y.H.; Li, D.K.; Quan, Z.Y.; Wang, C.Y.; Zhou, M.; Sun, Z.X. Exploration of components and mechanisms of Polygoni Multiflori Radix-induced hepatotoxicity using siRNA -mediated CYP3A4 or UGT1A1 knockdown liver cells. J. Ethnopharmacol. 2021, 270, 113845. [Google Scholar] [CrossRef]
- Zhai, X.R.; Zou, Z.S.; Wang, J.B.; Xiao, X.H. Herb-Induced Liver Injury Related to Reynoutria multiflora (Thunb.) Moldenke: Risk Factors, Molecular and Mechanistic Specifics. Front. Pharmacol. 2021, 12, 738577. [Google Scholar] [CrossRef]
- Rao, T.; Liu, Y.T.; Zeng, X.C.; Li, C.P.; Ou-Yang, D.S. The hepatotoxicity of Polygonum multiflorum: The emerging role of the immune-mediated liver injury. Acta Pharmacol. Sin. 2021, 42, 27–35. [Google Scholar] [CrossRef]
- Lu, Z.; Luo, Q.; Zhao, L.; Shi, Y.; Wang, N.; Wang, L.; Han, Z. The Mutational Features of Aristolochic Acid-Induced Mouse and Human Liver Cancers. Hepatology 2020, 71, 929–942. [Google Scholar] [CrossRef]
- Luo, P.; Chen, J.; Zhang, Q.; Xia, F.; Wang, C.; Bai, Y.; Tang, H.; Liu, D.; Gu, L.; Du, Q.; et al. Dissection of cellular and molecular mechanisms of aristolochic acid-induced hepatotoxicity via single-cell transcriptomics. Precis. Clin. Med. 2022, 5, pbac023. [Google Scholar] [CrossRef]
- Adhikari, B.; Marasini, B.P.; Rayamajhee, B.; Bhattarai, B.R.; Lamichhane, G.; Khadayat, K.; Adhikari, A.; Khanal, S.; Parajuli, N. Potential roles of medicinal plants for the treatment of viral diseases focusing on COVID-19: A review. Phytother. Res. 2021, 35, 1298–1312. [Google Scholar] [CrossRef] [PubMed]
- Vamadevaiah, R.M.; Santhekadur, P.K. Herbal Immunity Booster-Associated Liver Injury During COVID-19 Pandemic and Aflatoxins. J. Clin. Exp. Hepatol. 2021, 12, 252–253. [Google Scholar] [CrossRef] [PubMed]
- Nagral, A.; Adhyaru, K.; Rudra, O.S.; Gharat, A.; Bhandare, S. Herbal Immune Booster-Induced Liver Injury in the COVID-19 Pandemic—A Case Series. J. Clin. Exp. Hepatol. 2021, 11, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Björnsson, E.S.; Navarro, V.J.; Chalasani, N. Liver Injury following Tinospora cordifolia Consumption: Drug-Induced AIH, or de novo AIH? J. Clin. Exp. Hepatol. 2022, 12, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Balkrishna, A.; Bhattacharya, K.; Sinha, S.; Dev, R.; Srivastava, J.; Singh, P.; Haldar, S.; Varshney, A. Apparent Hepatotoxicity of Giloy (Tinospora cordifolia): Far from What Meets the Eyes. J. Clin. Exp. Hepatol. 2022, 12, 239–240. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Prajapati, P.K. Remarks on “Herbal Immune Booster-Induced Liver Injury in the COVID-19 Pandemic—A Case Series”. J. Clin. Exp. Hepatol. 2022, 12, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Philips, C.A.; Abraham, L.; Mission for Ethics and Science in Health Care (MESH). Tinospora cordifolia (Giloy) and Autoimmune-like Liver Injury—A Classic Case of Primum Non Nocere, “First, Do No Harm”. J. Clin. Exp. Hepatol. 2022, 12, 245–246. [Google Scholar] [CrossRef] [PubMed]
- Ruknuddin, G.; Narayanam, S.; Nesari, T.M. Do Tinospora cordifolia Cause Hepatic Damage? J. Clin. Exp. Hepatol. 2022, 12, 244. [Google Scholar] [CrossRef]
- Parikh, P. Knowledge of Herbal Medicines—Is a Reverse Bridge Course an Urgent Necessity? J. Clin. Exp. Hepatol. 2022, 12, 249–251. [Google Scholar] [CrossRef]
- Gupta, S.; Dhankhar, Y.; Har, B.; Agarwal, S.; Singh, S.A.; Gupta, A.K.; Saigal, S.; Jadaun, S.S. Probable Drug-Induced Liver Injury Caused by Tinospora species: A Case Report. J. Clin. Exp. Hepatol. 2022, 12, 232–234. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, M.; Jagdish, R.K.; Vij, V.; Bansal, N. Herbal Immune Booster-Induced Liver Injury in the COVID-19 Pandemic. J. Clin. Exp. Hepatol. 2021, 12, 258–259. [Google Scholar] [CrossRef] [PubMed]
- Sahney, A.; Wadhawan, M.; Kumar, A. Tinospora cordifolia—A Double Edge Sword? J. Clin. Exp. Hepatol. 2022, 12, 230–231. [Google Scholar] [CrossRef] [PubMed]
- Gupta, H.; Nigam, N.; Singh, S.; Roy, A.; Dhiman, R.K. Immune Boosting Gone Wrong? A COVID-Concoction-Conundrum. J. Clin. Exp. Hepatol. 2022, 12, 235–236. [Google Scholar] [CrossRef] [PubMed]
- Nagral, A.; Rudra, O.S.; Adhyaru, K.; Gharat, A.; Bhandare, S. Author Response to Letters on the Manuscript “Herbal Immune Booster-Induced Liver Injury in the COVID-19 Pandemic—A Case Series”. J. Clin. Exp. Hepatol. 2022, 12, 260–262. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, A.V.; Hanchanale, P.; Prakash, V.; Kalal, C.; Sharma, M.; Kumar, K.; Bishnu, S.; Kulkarni, A.V.; Anand, L.; Patwa, A.K.; et al. Tinospora cordifolia (Giloy) induced liver injury during the COVID-19 pandemic—Multicenter nationwide study from India. Hepatol. Commun. 2022, 6, 1289–1300. [Google Scholar] [CrossRef] [PubMed]
- Longiave, D.; Omini, C.; Nicosia, S.; Berti, F. The mode of action of aescin on isolated veins: Relationship with PGF2 alpha. Pharmacol. Res. Commun. 1978, 10, 145–152. [Google Scholar] [CrossRef]
- Rehn, D.; Golden, G.; Nocker, W.; Diebschlag, W.; Lehmacher, W. Comparison between the efficacy and tolerability of oxerutins and troxerutin in the treatment of patients with chronic venous insufficiency. Arzneim.-Forsch. Drug Res. 1993, 43, 1060–1063. [Google Scholar]
- Santos, D.C.; Lérias, G.; Madruga, I. Drug-induced Liver Injury Due to a Horse Chestnut Dietary Supplement. Eur. J. Case Rep. Intern. Med. 2021, 8, 002389. [Google Scholar] [CrossRef]
- FDA. Adverse Illness Event Series/Lentil and Leek Crumbles/Jun 2022 (CARA #1076) Incident Summary Report; FDA: Silver Spring, MD, USA, 2022. [Google Scholar]
- Berk, C.; Ammar, T.; Lee, B.T. Acute Liver Failure due to Manufactured Alkaline Water: A Case Series of “Real Water”-Induced Liver Injury. Am. J. Gastroenterol. 2021, 116, 2476–2477. [Google Scholar] [CrossRef] [PubMed]
- Ruff, J.C.; Zhang, Y.; Bui, D.P.; Therriault, C.; Nogee, D.; Guthery, S.L.; Daniel, J. Notes from the Field: Acute Nonviral Hepatitis Linked to a Brand of Alkaline Bottled Water—Clark County, Nevada and California, 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1617–1619. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, A.; Antala, D.; Pudasainee, P.; Panginikkod, S.; Gupta, H. A Plausible Association Between the Use of Elderberry and Autoimmune Hepatitis. Cureus 2022, 14, e24250. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Niu, M.; Wei, A.-W.; Tang, J.-F.; Li, P.-Y.; Song, D.; Bai, Z.-F.; Liu, Y.-P.; Xiao, X.-H.; Wang, J.-B. Clinical correlation between serum cytokines and the susceptibility to Polygonum multiflorum-induced liver injury and an experimental study. Food Funct. 2022, 13, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rodríguez, D.R.; Lozano-Sepulveda, S.A.; Delgado-Montemayor, C.; Waksman, N.; Cordero-Perez, P.; Rivas-Estilla, A.M. Turnera diffusa extract attenuates profibrotic, extracellular matrix and mitochondrial markers in activated human hepatic stellate cells (HSC). Ann. Hepatol. 2021, 22, 100281. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Montemayor, C.; Cordero-Pérez, P.; Torres-González, L.; Salazar-Cavazos, M.d.l.L.; Saucedo, A.L.; Paniagua-Vega, D.; Waksman-Minsky, N.H. Development of a Hepatoprotective Herbal Drug from Turnera diffusa. Evid. Based Complement. Altern. Med. 2022, 2022, 5114948. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.-L.; Chen, Y.-X.; Liu, L.-L.; Li, M.; Xu, R.; Qu, W.-S.; Yin, J.-Y.; Zhang, X.; Zhou, Z.-H.; Gao, Y.-T.; et al. Chemical characters and protective effect of Baqi Lingmao formula on experimental liver injury. J. Tradit. Chin. Med. 2021, 41, 862–874. [Google Scholar] [CrossRef]
- Xie, S.Z.; Zhai, X.Y.; Xi, S.Y.; Qiu, Y.K.; Zhang, Y.M.; Kong, X.J.; Li, Y.H.; Zhu, L.; Wang, Z.; Zhang, S.G.; et al. The Protective Effects of Zornia diphylla (L.) Pers. Against Acute Liver Injury Induced by Carbon Tetrachloride in Mice. Front. Pharmacol. 2021, 12, 764282. [Google Scholar] [CrossRef]
- Liao, J.; Lu, Q.; Li, Z.; Li, J.; Zhao, Q.; Li, J. Acetaminophen-induced liver injury: Molecular mechanism and treatments from natural products. Front. Pharmacol. 2023, 14, 1122632. [Google Scholar] [CrossRef]
- Chilvery, S.; Yelne, A.; Khurana, A.; Saifi, M.A.; Bansod, S.; Anchi, P.; Godugu, C. Acetaminophen induced hepatotoxicity: An overview of the promising protective effects of natural products and herbal formulations. Phytomedicine 2023, 108, 154510. [Google Scholar] [CrossRef]
- Mahmoudi, F.; Arasteh, O.; Elyasi, S. Preventive and therapeutic use of herbal compounds against doxorubicin induced hepatotoxicity: A comprehensive review. Naunyn-Schmiedeb. Arch. Pharmacol. 2023, 396, 1595–1617. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Li, S.; Li, Y.; Gan, R.Y.; Li, H.B. Gut Microbiota’s Relationship with Liver Disease and Role in Hepatoprotection by Dietary Natural Products and Probiotics. Nutrients 2018, 10, 1457. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.K.; Ai, Y.; Cheng, Z.L.; Yang, L.; Hou, X.H. Contribution of gut microbiota to drug-induced liver injury. Hepatobiliary Pancreat. Dis. Int. 2023, 22, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Cui, S.; Tang, X.; Zhang, Q.; Zhao, J.; Mao, B.; Zhang, H. Intestinal Microbiomics and Metabolomics Insights into the Hepatoprotective Effects of Lactobacillus paracasei CCFM1222 Against the Acute Liver Injury in Mice. Probiotics Antimicrob. Proteins 2023, 15, 1063–1077. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Huang, A.; Wang, Y.; Ji, D.; Liang, Q.; Zhao, J.; Zhou, G.; Liu, S.; Niu, M.; Sun, Y.; et al. Corticosteroid plus glycyrrhizin therapy for chronic drug- or herb-induced liver injury achieves biochemical and histological improvements: A randomised open-label trial. Aliment. Pharmacol. Ther. 2022, 55, 1297–1310. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Liu, J.; Chang, X.; Lin, D. Glycyrrhizin protects against diosbulbin B-induced hepatotoxicity by inhibiting the metabolic activation of diosbulbin B. J. Biochem. Mol. Toxicol. 2023, 38, e23549. [Google Scholar] [CrossRef] [PubMed]
- Tan, R.; Hu, Z.; Zhou, M.; Liu, Y.; Wang, Y.; Zou, Y.; Li, K.; Zhang, S.; Pan, J.; Peng, Y.; et al. Diosbulbin B: An important component responsible for hepatotoxicity and protein covalent binding induced by Dioscorea bulbifera L. Phytomedicine 2022, 102, 154174. [Google Scholar] [CrossRef]
- Achufusi, T.G.O.; Patel, R.K. Milk Thistle. React. Wkly. 1999, 749, 10. [Google Scholar] [CrossRef]
- Horowitz, B.Z. Silibinin: A toxicologist’s herbal medicine? Clin. Toxicol. 2022, 60, 1194–1197. [Google Scholar] [CrossRef]
Figure 1.
Materials and methods.


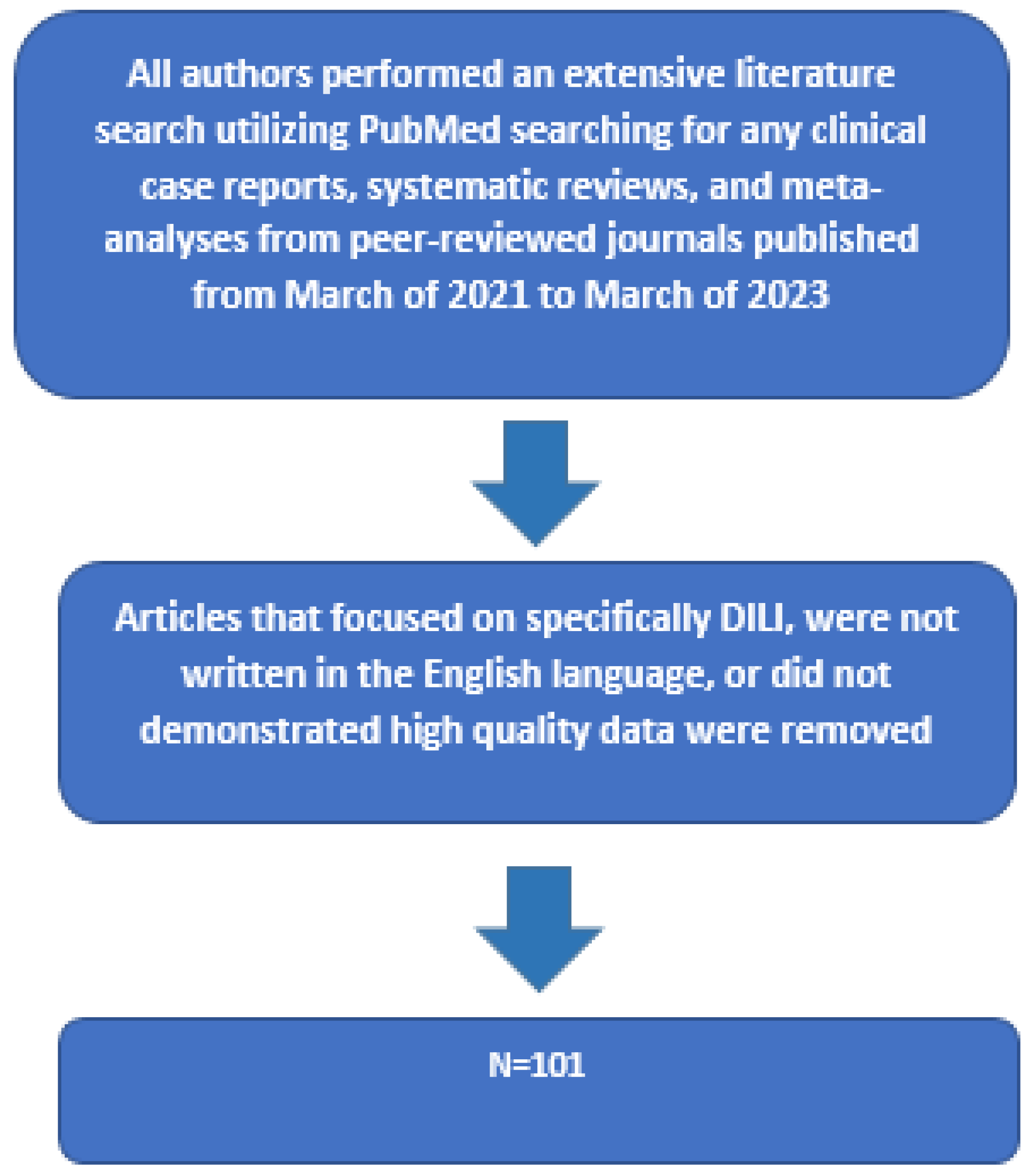{kind=link}
Table 1.
The proposed Dietary Supplement Listing Act of 2022.
| What the Act Implements | What the Act Does Not Implement |
|---|---|
| Publicly Available Database | No Ability to Approve or Reject Products |
| Mandated Ingredient Reporting | No Changes to Manufacturing Rules |
| Potential Allergen Listing | No Increased Regulatory Power |
| Ingredient/Product Warnings | No Changes to Product Advertisement |
Table 2.
Recent FDA warnings.
| Date | Health Area | Illegal Activity | Number of Companies Affected |
|---|---|---|---|
| February 2021 | Depression and Mental Illness | Claiming to cure, treat, mitigate, or prevent disease | 10 |
| May 2021 | Infertility | Claiming to cure, treat, mitigate, or prevent disease | 5 |
| September 2021 | Diabetes | Claiming to cure, treat, mitigate, or prevent disease | 10 |
| May 2022 | Dietary Supplement | Adulterated supplements with potentially dangerous additions, some of which are also (without FDA approval) claiming to cure, treat, mitigate, or prevent disease | 10 (initially 11, with one retraction) |
| November 2022 | Cardiovascular Disease | Claiming to cure, treat, mitigate, or prevent disease | 7 |
Table 3.
National Library of Medicine LiverTox likelihood scale of liver injury definitions.
| Category | Likelihood of Association with Liver Injury |
|---|---|
| A | Drug is well known, well described, and well reported; more than 50 cases have been described including case series |
| B | Drug is reported and known or highly likely; 12–50 cases described including small case series |
| C | Drug probably linked, but reported uncommonly; less than 12 cases without significant case series |
| D | Single case reports, may not be very convincing; fewer than 3 cases have been reported and only said to be possible hepatotoxin or rare cause |
| E | No evidence, single case reports may be published but largely unconvincing; not believed or unlikely to cause livery injury |
Table 4.
Herbal and dietary supplements identified as possible etiologies of liver injury, including those causing acute liver failure, with their likelihood score if listed in LiverTox.
Table 4.
Herbal and dietary supplements identified as possible etiologies of liver injury, including those causing acute liver failure, with their likelihood score if listed in LiverTox.
| HDS | Likelihood Score as Listed in LiverTox as of 2023 |
|---|---|
| Aloe vera | B |
| Apoaequorin | E |
| Ashwaganda | C |
| Astragalus | E |
| Bilberry | E |
| Black cohosh | A |
| Boswellia | E |
| Butterbur | C |
| Cat’s claw | E |
| Chamomile | E |
| Chaparral | B |
| Chaste tree | E |
| Chinese/Asian Herbal Medicines | |
| Ba Jiao Lian | B |
| Chi R Yun (Breynia officinalis) | C |
| Jin Bu Huan | Cannot be assessed |
| Ma Huang (Ephedra sinica) | Not listed |
| Polygonum multiflorum | A |
| Sho-saiko-to and Dai-saiko-to | B |
| Chondroitin (Glucosamine) | D |
| Clenbuterol supplement | Withdrawn from market |
| Comfrey | C |
| Cranberry | E |
| Crofelemer | E |
| Echinacea | D |
| Eugenol | C |
| Fenugreek | E |
| Flavocoxid | C |
| Garcinia cambogia | B |
| Gardenia | Not listed in LiverTox, or listed as unlikely cause of clinically apparent liver injury |
| Germander | A |
| Ginkgo | E |
| Ginseng | E |
| Greater celandine | B |
| Green tea extract | A |
| Guarana | E |
| Hawthorn | E |
| Hoodia | E |
| Hop | E |
| Horny goat weed | E |
| Horse chestnut | D |
| Horsetail | C |
| Hyssop | E |
| Kava Kava | A |
| Khat | B |
| Kombucha tea | C |
| Kratom | B |
| Lavender | E |
| Maca | E |
| Margosa Oil | C |
| Melatonin | E |
| Milk thistle (silymarin or silybin) | E |
| Mistletoe | E |
| Multi-Ingredient Nutritional Supplements Herbalife | A |
| Hydroxycut | B |
| Move Free | C |
| OxyELITE pro | A |
| SLIMQUICK | C |
| Noni | C |
| Passionflower | C |
| Pennyroyal oil | B |
| Quercetin | E |
| Red yeast rice | C |
| Resveratrol | E |
| Reumofan plus | Not listed in LiverTox, or listed as unlikely cause of clinically apparent liver injury |
| Saw palmetto | D |
| Senna (Cassia species) | D |
| Skullcap | B |
| Spirulina | D |
| St. John’s wort | E |
| Tribulus | E |
| Tumeric | B |
| Usnic acid | B |
| Uva ursi | E |
| Valerian | C |
| Yohimbine | E |
Table 5.
Newly described hepatoprotective HDSs.
| Newly Described Hepatoprotective Herbal Supplements | Description |
|---|---|
| Tunera diffusa | Shrub native to southern Texas in the United States, Central America, Mexico, South America, and the Caribbean. It has been shown to impair fibrotic mechanisms in stellate cells. |
| Baqi Lingmao formula | Formula composed of ten herbal supplements, shown to prevent hepatocyte death by blocking inflammatory cytokine secretion of interferon-γ, tumor necrosis factor-α and interleukin-6. |
| Zornia diphylla (L.) Pers. | Herbal supplement shown to inhibit cell injury when hepatocytes were exposed to carbon tetrachloride. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Patel-Rodrigues, P.A.; Cundra, L.; Alhaqqan, D.; Gildea, D.T.; Woo, S.M.; Lewis, J.H. Herbal- and Dietary-Supplement-Induced Liver Injury: A Review of the Recent Literature. Livers 2024, 4, 94-118. https://doi.org/10.3390/livers4010008
AMA Style
Patel-Rodrigues PA, Cundra L, Alhaqqan D, Gildea DT, Woo SM, Lewis JH. Herbal- and Dietary-Supplement-Induced Liver Injury: A Review of the Recent Literature. Livers. 2024; 4(1):94-118. https://doi.org/10.3390/livers4010008
Chicago/Turabian StylePatel-Rodrigues, Palak A., Lindsey Cundra, Dalal Alhaqqan, Daniel T. Gildea, Stephanie M. Woo, and James H. Lewis. 2024. "Herbal- and Dietary-Supplement-Induced Liver Injury: A Review of the Recent Literature" Livers 4, no. 1: 94-118. https://doi.org/10.3390/livers4010008