You might also like
- heng2017Document6 pagesheng2017CLINICA VETERINARIA DE MEDELLINNo ratings yet
- Lung Lobe Torsion in Seven Juvenile DogsDocument7 pagesLung Lobe Torsion in Seven Juvenile DogsKelvinSueyzyNo ratings yet
- tmp55D7 TMPDocument7 pagestmp55D7 TMPFrontiersNo ratings yet
- tmpEC6D TMPDocument7 pagestmpEC6D TMPFrontiersNo ratings yet
- Pulmonary Oedema in A Hunting Dog: A Case Report: C.F. Agudelo, P. SchanilecDocument4 pagesPulmonary Oedema in A Hunting Dog: A Case Report: C.F. Agudelo, P. SchanilecErlangga ReeNo ratings yet
- Case Report: Surgical Removal of A Canine Aortic Thromboembolism Secondary To PancreatitisDocument8 pagesCase Report: Surgical Removal of A Canine Aortic Thromboembolism Secondary To PancreatitisIvan RisnaNo ratings yet
- Case Report: Rapport de CasDocument6 pagesCase Report: Rapport de CasWidya KartikaNo ratings yet
- Tetralogía en Hurón - CASODocument6 pagesTetralogía en Hurón - CASOLAURA AILED LOPEZ LOZANo ratings yet
- Aortic Dissection Associated With Aortic Aneurysms and Posterior Paresis in A DogDocument7 pagesAortic Dissection Associated With Aortic Aneurysms and Posterior Paresis in A DogMuhamad Abdul MubdiNo ratings yet
- Uptake of Fluorine-18-Fluorodeoxyglucose in Sarcoidosis: J Nucl MedDocument4 pagesUptake of Fluorine-18-Fluorodeoxyglucose in Sarcoidosis: J Nucl Medangelica barrazaNo ratings yet
- Case Report Primary Mycoplasma Pneumonia Associated With Reversible Respiratory Failure in A CatDocument5 pagesCase Report Primary Mycoplasma Pneumonia Associated With Reversible Respiratory Failure in A CatrianperoNo ratings yet
- Cholinergic Control of Rabbit Tracheal Transepithelial Potential Difference in VivoDocument5 pagesCholinergic Control of Rabbit Tracheal Transepithelial Potential Difference in VivoSyeni Tisna Rahma AtikaNo ratings yet
- Lowe Et Al. - 1986 - Facial Morphology and Obstructive Sleep ApneaDocument8 pagesLowe Et Al. - 1986 - Facial Morphology and Obstructive Sleep ApnealinhhkngNo ratings yet
- Successful Treatment of Pneumothorax in A Dog With Sterile Pleural Fibrosis Caused by ChylothoraxDocument9 pagesSuccessful Treatment of Pneumothorax in A Dog With Sterile Pleural Fibrosis Caused by Chylothoraxnatalia figueroaNo ratings yet
- Characterization of Primary Pulmonary Adenosquamous Carcinoma-Associated Pleural EffusionDocument5 pagesCharacterization of Primary Pulmonary Adenosquamous Carcinoma-Associated Pleural EffusionIoana SanduNo ratings yet
- CT Features of Extrahepatic Arterioportal Fistula in Two CatsDocument4 pagesCT Features of Extrahepatic Arterioportal Fistula in Two CatsVennaOktaviaAnggrainiNo ratings yet
- A Case Report of Feline Pituitary Carcinoma With HypercortisolismDocument6 pagesA Case Report of Feline Pituitary Carcinoma With HypercortisolismSatriaNo ratings yet
- Ascites With Right Heart Failure in A Dog: Diagnosis and ManagementDocument5 pagesAscites With Right Heart Failure in A Dog: Diagnosis and ManagementairaNo ratings yet
- JTD 06 06 E77Document4 pagesJTD 06 06 E77jamieNo ratings yet
- CVJ 49 PG 583Document4 pagesCVJ 49 PG 583paula gonzalezNo ratings yet
- CVJ - 09 - 845 Jurnal Kanker Hati Pada Anjing Muda PDFDocument4 pagesCVJ - 09 - 845 Jurnal Kanker Hati Pada Anjing Muda PDFtia hyunjoongNo ratings yet
- Ventilatory Management of Severe Tracheal Stenosis: Rakesh Lodha, Lokesh Guglani, S.C. Sharma and S.K. KabraDocument4 pagesVentilatory Management of Severe Tracheal Stenosis: Rakesh Lodha, Lokesh Guglani, S.C. Sharma and S.K. KabraPcrNo ratings yet
- A Case of Primary Papillary Disseminated Adenocarcinoma of Canine LungDocument5 pagesA Case of Primary Papillary Disseminated Adenocarcinoma of Canine LungStéfano Celis ConsiglieriNo ratings yet
- Ultrasound Diagnosis: Phiwipha KamonratDocument3 pagesUltrasound Diagnosis: Phiwipha KamonratVanessa Hidalgo PincheiraNo ratings yet
- JDVAR-12-00319 nothingDocument5 pagesJDVAR-12-00319 nothingazomamungpi2No ratings yet
- Comparison of Time To Desaturation BetweenDocument6 pagesComparison of Time To Desaturation BetweenBruna Gonçalves FerreiraNo ratings yet
- Case Report AbdomenDocument5 pagesCase Report Abdomensigario hutamaNo ratings yet
- Human Exposure To Heavy Metals: EarthDocument4 pagesHuman Exposure To Heavy Metals: EarthLukas J TangguhNo ratings yet
- Accepted Manuscript: Topics in Companion Animal MedicineDocument21 pagesAccepted Manuscript: Topics in Companion Animal MedicinedanielleclimacoNo ratings yet
- Lung Ring-Down Artifact As A Sign of Pulmonary Alveolar-Interstitial DiseaseDocument5 pagesLung Ring-Down Artifact As A Sign of Pulmonary Alveolar-Interstitial DiseaseashaNo ratings yet
- 380 FullDocument3 pages380 FulltiaraNo ratings yet
- Iwamoto 1985Document6 pagesIwamoto 1985Casp ianNo ratings yet
- Hipertensão PulmonarDocument10 pagesHipertensão PulmonarAnnelise GretherNo ratings yet
- ECG findings in a dog with pericardial effusion and cardiac tamponadeDocument5 pagesECG findings in a dog with pericardial effusion and cardiac tamponadeDewa Aix61No ratings yet
- Airway-Centered Fibroelastosis 2016Document8 pagesAirway-Centered Fibroelastosis 2016Edoardo CavigliNo ratings yet
- Thrombocytopathia and Light-Chain Proteinuria in A Dog Naturally Infected WithDocument3 pagesThrombocytopathia and Light-Chain Proteinuria in A Dog Naturally Infected WithDiana GranadaNo ratings yet
- Amjpathol00193 0017Document10 pagesAmjpathol00193 0017AniteiFlorinAlexandruNo ratings yet
- Progression of Pulmonary Lesions in Cat with ParagonimosisDocument5 pagesProgression of Pulmonary Lesions in Cat with ParagonimosisMahdawwNo ratings yet
- Suspected Relative Adrenal Insufficiency in A Critically Ill CatDocument5 pagesSuspected Relative Adrenal Insufficiency in A Critically Ill CatdenisegmeloNo ratings yet
- Studies On Feline Hepatic Lipidosis: Egypt. J. Comp. Path. & Clinic. Path. Vol. 22 No. 3 (July) 2009 77 - 95Document19 pagesStudies On Feline Hepatic Lipidosis: Egypt. J. Comp. Path. & Clinic. Path. Vol. 22 No. 3 (July) 2009 77 - 95Firman HasanNo ratings yet
- Tobacco Exposure Increased Airway Limitation in Dogs With Chronic CoughDocument4 pagesTobacco Exposure Increased Airway Limitation in Dogs With Chronic CoughBrandoNo ratings yet
- Case Report: Rapport de CasDocument4 pagesCase Report: Rapport de CasSastra NopiNo ratings yet
- Ijvm June 2011 FinalDocument64 pagesIjvm June 2011 FinalAmitesh DubeyNo ratings yet
- Prognostic Value of Desaturation During A 6-Minute Walk Test in Idiopathic Interstitial PneumoniaDocument7 pagesPrognostic Value of Desaturation During A 6-Minute Walk Test in Idiopathic Interstitial PneumoniaVh TRNo ratings yet
- Advances in Respiratory Monitoring: Pulse Oximetry Accuracy and Clinical UseDocument10 pagesAdvances in Respiratory Monitoring: Pulse Oximetry Accuracy and Clinical Useindra muhammadNo ratings yet
- Neurohormonal Activation in Severe Scorpion Envenomation: Correlation With Hemodynamics and Circulating ToxinDocument6 pagesNeurohormonal Activation in Severe Scorpion Envenomation: Correlation With Hemodynamics and Circulating ToxinDaniela SalamancaNo ratings yet
- Basic Arterial Blood Gas (Abg) Interpretation: By: Jesus Mario A Lopez JR., R.T.,R.NDocument36 pagesBasic Arterial Blood Gas (Abg) Interpretation: By: Jesus Mario A Lopez JR., R.T.,R.NJesus Mario LopezNo ratings yet
- Tmp9e41 TMPDocument3 pagesTmp9e41 TMPFrontiersNo ratings yet
- 1564 Full PDFDocument10 pages1564 Full PDFBruno Henrique BispoNo ratings yet
- 1564 Full PDFDocument10 pages1564 Full PDFBruno Henrique BispoNo ratings yet
- Proton-Nuclear-Magnetic-Resonance Studies of Serum, Plasma and Urine From Fasting Normal Diabetic SubjectsDocument11 pagesProton-Nuclear-Magnetic-Resonance Studies of Serum, Plasma and Urine From Fasting Normal Diabetic SubjectsKeyla MaydeeNo ratings yet
- 3Document7 pages3soledadDC329No ratings yet
- Journals Javma 217 2 Javma.2000.217.231-PreviewDocument2 pagesJournals Javma 217 2 Javma.2000.217.231-PreviewJasna IsovićNo ratings yet
- Original ArticleDocument11 pagesOriginal ArticlePablo Tapia BatallaNo ratings yet
- Javma 237 3 299Document5 pagesJavma 237 3 299tcvhNo ratings yet
- Effects of Butorphanol and Carprofen On The Minimal Alveolar Concentration of Isoflurane in DogsDocument4 pagesEffects of Butorphanol and Carprofen On The Minimal Alveolar Concentration of Isoflurane in DogsjohacasbrugesNo ratings yet
- Cardiovascular Parameter in A Mixed-Sex Swine Study of Severe Dcs Sickness Treated With The Emulsified Perfluorocarbon OxycyteDocument9 pagesCardiovascular Parameter in A Mixed-Sex Swine Study of Severe Dcs Sickness Treated With The Emulsified Perfluorocarbon OxycyteVenansius Ratno KurniawanNo ratings yet
- Respiratory Monitoring Arterial Blood Gas Analysis Pulse Oximetry and End Tida Carbon Dioxide AnalysisDocument4 pagesRespiratory Monitoring Arterial Blood Gas Analysis Pulse Oximetry and End Tida Carbon Dioxide AnalysiskradoNo ratings yet
- CO Inhalation at Dose Corresponding To Tobacco Smoke Worsens Cardiac Remodeling After Experimental Myocardial Infarction in RatsDocument7 pagesCO Inhalation at Dose Corresponding To Tobacco Smoke Worsens Cardiac Remodeling After Experimental Myocardial Infarction in RatsGael ROCHEFORTNo ratings yet
- Formulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy CatsDocument8 pagesFormulation of A Standardized Protocol and Determination of The Size and Appearance of The Spleen in Healthy Catsludiegues752No ratings yet
- Small Animal Abdominal Ultrasonography - The SpleenDocument9 pagesSmall Animal Abdominal Ultrasonography - The Spleenludiegues752No ratings yet
- Top 5 Causes of Splenomegaly in Dogs - Clinicians BriefDocument5 pagesTop 5 Causes of Splenomegaly in Dogs - Clinicians Briefludiegues752No ratings yet
- Radiology Packet 7 Congenital Cardiac DiseaseDocument27 pagesRadiology Packet 7 Congenital Cardiac Diseaseludiegues752No ratings yet
- Imaging Intestinal ObstructionDocument5 pagesImaging Intestinal Obstructionludiegues752No ratings yet
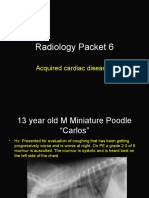
- Radiology Packet 6 Acquired Cardiac DiseasesDocument25 pagesRadiology Packet 6 Acquired Cardiac Diseasesludiegues752No ratings yet
- US Artifacts - University of ChicagoDocument101 pagesUS Artifacts - University of Chicagoludiegues752No ratings yet
- (2012) Investigation and Management of Splenic Disease in DogsDocument8 pages(2012) Investigation and Management of Splenic Disease in Dogsludiegues752No ratings yet
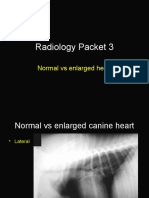
- Radiology Packet 3 Normal Vs Enlarged HeartDocument11 pagesRadiology Packet 3 Normal Vs Enlarged Heartludiegues752No ratings yet
- (2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary MedicineDocument3 pages(2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary Medicineludiegues752No ratings yet
- (2012) Investigation and Management of Splenic Disease in DogsDocument8 pages(2012) Investigation and Management of Splenic Disease in Dogsludiegues752No ratings yet
- (1997) Ultrasonographic Adrenal Gland Measurements in Dogs Without Evidence of Adrenal DiseaseDocument7 pages(1997) Ultrasonographic Adrenal Gland Measurements in Dogs Without Evidence of Adrenal Diseaseludiegues752No ratings yet
- (2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary MedicineDocument3 pages(2004) Ultrasonographic Evaluation of Abdominal Organs in Veterinary Medicineludiegues752No ratings yet
- Radiology Packet 4 Cardiac CasesDocument28 pagesRadiology Packet 4 Cardiac Casesludiegues752No ratings yet
- Radiology Packet 5: Heart Failure CasesDocument25 pagesRadiology Packet 5: Heart Failure Casesludiegues752No ratings yet
- Ultrasonographic Evaluation of Adrenal Gland Size Compared To Body Weight in Normal DogsDocument10 pagesUltrasonographic Evaluation of Adrenal Gland Size Compared To Body Weight in Normal Dogsludiegues752No ratings yet
- (2016) Associations Between Sex, Body Weight, Age, and US Determined Adrenal Thickness in Dogs With Non-Adrenal Gland IllnessDocument9 pages(2016) Associations Between Sex, Body Weight, Age, and US Determined Adrenal Thickness in Dogs With Non-Adrenal Gland Illnessludiegues752No ratings yet
- (2010) Ultrasonographic Evaluation of Adrenal Glands in Dogs With Primary Hypoadrenocorticism or Mimicking DiseasesDocument5 pages(2010) Ultrasonographic Evaluation of Adrenal Glands in Dogs With Primary Hypoadrenocorticism or Mimicking Diseasesludiegues752No ratings yet
- (2016) Retrospective Study of Adrenal Gland US in Dogs With Normal and Abnormal ACTH Stimulation Test - Eric Lindquist PDFDocument6 pages(2016) Retrospective Study of Adrenal Gland US in Dogs With Normal and Abnormal ACTH Stimulation Test - Eric Lindquist PDFludiegues752No ratings yet
- (2017) Repetitive Ultrasonographic Assessment of Adrenal Size and Shape Changes - A Clue For An Asymptomatic Sex Hormone-Secreting AdenomaDocument5 pages(2017) Repetitive Ultrasonographic Assessment of Adrenal Size and Shape Changes - A Clue For An Asymptomatic Sex Hormone-Secreting Adenomaludiegues752No ratings yet
- Dermatology History FormDocument1 pageDermatology History Formludiegues752No ratings yet
- The IntegumentDocument15 pagesThe Integumentludiegues752No ratings yet
- (2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in DogsDocument5 pages(2016) Prevalence of Adrenal Gland Masses As Incidental Findings During Abdominal Computed Tomography in Dogsludiegues752No ratings yet
- (2016) Ultrasonographic Features of Adrenal Gland Lesions in Dogs Can Aid in DiagnosisDocument9 pages(2016) Ultrasonographic Features of Adrenal Gland Lesions in Dogs Can Aid in Diagnosisludiegues752No ratings yet
- Alterations in The SkinDocument9 pagesAlterations in The Skinludiegues752No ratings yet
- (2012) Emerging Skin Conditions in CattleDocument9 pages(2012) Emerging Skin Conditions in Cattleludiegues752No ratings yet
- Spleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical EhrlichiosisDocument5 pagesSpleen Evaluation Using Contrast Enhanced Ultrasonography and Doppler in Dogs With Subclinical Ehrlichiosisludiegues752No ratings yet
- Small Animal Abdominal Ultrasonography Liver & GallBladder - Part 2Document8 pagesSmall Animal Abdominal Ultrasonography Liver & GallBladder - Part 2ludiegues752100% (1)
- (2015) Basics of Equine DermatologyDocument10 pages(2015) Basics of Equine Dermatologyludiegues752No ratings yet
- Pedia 3.1 Pediatric PulmoDocument8 pagesPedia 3.1 Pediatric PulmoAswanth ThisaiveeranNo ratings yet
- Nursing Care PlansDocument48 pagesNursing Care PlansJuliantiMamangkey86% (7)
- ARDS Case PresentationDocument80 pagesARDS Case Presentationsupladitasha_750% (3)
- NP4 Nursing Board ExamDocument7 pagesNP4 Nursing Board ExamNewb TobikkoNo ratings yet
- Manual de SH300-20190109 - V - 19-01Document71 pagesManual de SH300-20190109 - V - 19-01Rigoberto Urquijo Garcia0% (1)
- Form 4 - Biology NotesDocument61 pagesForm 4 - Biology NotesZikri SabaruddinNo ratings yet
- 1st PT in Science 9 With TOS 2022 2023Document7 pages1st PT in Science 9 With TOS 2022 2023paulyn espino100% (1)
- Calabadion A New Agent To Reverse The Effects Of.18Document9 pagesCalabadion A New Agent To Reverse The Effects Of.18Hilton EmilNo ratings yet
- Pathophysiology PneumoniaDocument2 pagesPathophysiology PneumoniaChiro Rouy Malaluan100% (2)
- True PDFDocument306 pagesTrue PDFMarwan Zeidan100% (1)
- What Is Bronchitis 2Document3 pagesWhat Is Bronchitis 2lea jumawanNo ratings yet
- Physical Examination Head Neck Chest Breast and AbdomenDocument116 pagesPhysical Examination Head Neck Chest Breast and AbdomenSiva RamanNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document86 pagesChronic Obstructive Pulmonary Disease (COPD)physio43No ratings yet
- Noninvasive Strategies For Management of Respiratory Problems in NeonatesDocument12 pagesNoninvasive Strategies For Management of Respiratory Problems in NeonatesGaby RiveraNo ratings yet
- BurnsDocument9 pagesBurnsVincentus BinNo ratings yet
- Hyaline Membrane DiseaseDocument31 pagesHyaline Membrane DiseaseWeng RamojalNo ratings yet
- Pediatric Emergencies 1Document101 pagesPediatric Emergencies 1VIPIN V NAIR100% (1)
- SPIROMETRYDocument9 pagesSPIROMETRYaeyousefNo ratings yet
- Mechanism Of Swallowing: Stages And CoordinationDocument6 pagesMechanism Of Swallowing: Stages And CoordinationLittle MummutNo ratings yet
- Administering O2 TherapyDocument22 pagesAdministering O2 TherapyWilbert Andrew FlojemonNo ratings yet
- Unit:11 (Burn Injury)Document6 pagesUnit:11 (Burn Injury)Surkhali BipanaNo ratings yet
- Part One Applied Science Review Guide: Volume TwoDocument537 pagesPart One Applied Science Review Guide: Volume TwoAashay PatelNo ratings yet
- Deep Breathing, Coughing & Legs ExercisesDocument15 pagesDeep Breathing, Coughing & Legs Exercisesjoel david knda mj100% (5)
- University of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisDocument3 pagesUniversity of Cordilleras College of Nursing NCP: Mycobacterium TuberculosisLyn MhoreNo ratings yet
- Breathe In: Write Your Answer On These Activity SheetDocument4 pagesBreathe In: Write Your Answer On These Activity Sheetirah jane valentinoNo ratings yet
- Physiological changes in pregnancy: Respiratory, nervous, and musculoskeletal systemsDocument9 pagesPhysiological changes in pregnancy: Respiratory, nervous, and musculoskeletal systemsAyazNo ratings yet
- Fundamental Critical Care Support (FCCS) EditionDocument468 pagesFundamental Critical Care Support (FCCS) Editionruth Yoka100% (2)
- Matias - PEX 07 03Document7 pagesMatias - PEX 07 03Mae MatiasNo ratings yet
- Sputum Induction in Children2Document3 pagesSputum Induction in Children2Asri RachmawatiNo ratings yet
- Askep ARDSDocument23 pagesAskep ARDSnovitanurkamilahNo ratings yet