Download
1 / 21
280 likes | 573 Views
Toxoplasmosis in twenty minutes. Michael Addidle Clinical Microbiologist Pathlab. Preview. Background knowledge Toxoplasmosis in immunocompetent host Congenital toxoplasmosis Toxoplasmosis in an immunocompromised patient (HIV) Ocular toxoplasmosis Take Home Messages.

E N D
Toxoplasmosisin twenty minutes Michael Addidle Clinical Microbiologist Pathlab
Preview • Background knowledge • Toxoplasmosis in immunocompetent host • Congenital toxoplasmosis • Toxoplasmosis in an immunocompromised patient (HIV) • Ocular toxoplasmosis • Take Home Messages
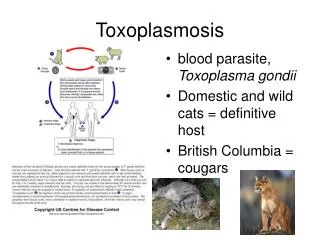
Transmission of toxoplasma to humans Ingestionofcat faeces (litter trays, salads) TOXOPLASMOSIS Ingestion of undercooked meats containing oocysts or bradyzoites
Case vignette: 25 year old male presents with 2 week history of malaise and marked bilateral cervical lymphadenopathy • What is the differential? • What tests should be done? • Relative lymphocytosis, mild transaminitis, Toxo IgM +ve and Toxo IgG positive. EBV(VCA) and CMV IgM negative. HIV negative • Is the diagnosis of toxoplasmosis correct.? • Should the patient be treated? • How long will the toxoplasma IgM be positive for? In immunocompetent individuals acute toxoplasmosis asymptomatic in up to 80% of individuals.
Lymphadenopathy • In toxoplasmosis, lymphadenopathy usually bilateral and mildly tender. Can take 4-6 months to settle completely. • Usually cervical.(posterior), but occasionally axillary or groin • Positive toxoplasma IgM serology results often have a history of lymphadenopathy on the request form.
Pitfalls in toxoplasma serologySummary • Beware cross reactive Toxoplasma IgMs from strong positive EBV or CMV IgMs • A toxoplasma IgM may hang around for anything up to 2 years • Unusual to get a IgM positive IgG negative toxo result.
Case Vignette: 29 yr old pregnant(13/40) lady with cervical lympadenopathy and fever. She has just got a kitten for the impending new arrival. • What tests would you order? • FBC, LFTs, EBV, CMV, Toxo serology, HIV. • Toxoplasma IgM positive, Toxoplasma IgG positive. HIV, CMV and EBV serology negative.
Is the foetus at risk? • Yes • Risk of toxoplasma transmission from mother to baby increases with gestational age. 6% at 13 weeks to 72% at 36 weeks. • Risk of serious symptoms/foetal damage resulting from congenital infection is highest in early pregnancy and decreases with gestational age.
What further investigations would you carry out? • Ensure EBV and CMV serology is negative. • Go back and check Toxoplasma serology on the booking bloods. • Refer to Obstetrician • Check Toxoplasma IgG avidity (Antibodies gradually become more avid (strength of attachment to antigen) as time from primary infection increases, therefore high avidity more likely to represent remote/distant infection. This is useful because of the length of time that Toxo IgM remains positive for)
Toxoplasma avidity testing in pregnancy • Would you do a Toxoplasma IgG avidity test on this lady? • Probably not , not going to determine whether infection actually happened during pregnancy.
Obstetric follow up • If congenital toxoplasmosis is suspected on basis of serology, obstetrician will monitor by serial ultrasounds and offer amniocentesis at 20-22 wks. • Spiramycin until term for pregnant mother with proven toxoplasma infection… unless • If congenital infection of foetus is confirmed by PCR of amniotic fluid then treatment of mother with pyrimethamine and sulphadiazine instead. (and baby will need treated as well when born)
Clinical presentation of congenital toxoplasmosis • Chorioretinitis, blindness, seizures, hydrocephalus, microcephaly, intracranial calcifications, encephalitis, mental retardation, lympadenopathy, hepatosplenomegaly, anemia and rash. • Congenitally infected infants may be asymptomatic at birth but then develop symptoms during childhood.(chorioretinitis, developmental delays) • PCR may help to confirm diagnosis in neonate. • Toxoplasma IgG negativity or disappearance on serial testing is only way to exclude congenital infection in neonates.
28 year old HIV patient presents with 3 week history of headache, fever and focal seizures of his right arm. Compliance with anti-retrovirals has been poor. • What is the differential diagnosis? Cryptococcal meningitis, TB, cerebral toxoplasmosis, lymphoma • What investigations would you perform? CT Brain CD4 count (usually less than 100 in HIV cerebral toxo), toxoplasma serology. CSF examination including cryptococcal antigen and TB culture. Consider toxoplasma PCR on CSF based on CD4 count and radiological findings.
CT findings • Multiple ring enhancing lesions, often with associated oedema • Main differential is lymphoma, cerebral metastases. • CT may occasionally be negative. MRI is also an option.
Edinburgh in the Early 90’s • HIV rife amongst the IDU population. • Whole ward dedicated to AIDS related illness at the Edinburgh ID hospital (Amongst patients, PCP most common but always a few with cryptococcal meningitis and cerebral toxoplasmosis)
Toxoplasma PCR • Expensive. Discuss with clinical microbiologist at reference lab where sample is going to. • Diagnosing Congenital infection in the Newborn Amniotic fluid 10 mL. (Collect at delivery if possible). Fresh placental biopsy. Cord blood – 1 mL in EDTA tube. • Diagnosing Intrauterine infection in the foetus Amniotic fluid; 10 mL Foetal blood (EDTA tube) Amniotic fluid is the preferred sample. • Heavily Immunocompromised patient Blood – 5 mL EDTA tube CSF – 2 mL CSF Tissue biopsy - Lymph node, cardiac biopsy, brain biopsy etc. • Ocular toxoplasmosis Vitreous fluid
Ocular toxoplasmosis • Diagnosis is usually clinical. • Usually in congenital or immunocompromised cohorts. However can occur occasionally in immunocompetent adults. • Supportive evidence of +ve toxoplasma IgG abs • PCR on vitreous fluid for difficult cases. • Exclude syphilis infection.
Take Home Messages • Toxoplasmosis is not uncommon • Be aware of the relative importance of toxoplasmosis in different clinical scenarios eg immunocompetent, congenital, immunocompromised. • Be aware of the tests that are available for diagnosis, including the IgG avidity test and the PCR test and when they are best utilised. • Be sure a positive Toxoplasma IgM is genuine.