
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Hydrocele- All types & treatment options
Similar to Hydrocele- All types & treatment options (20)
Recently uploaded
Recently uploaded (20)
Hydrocele- All types & treatment options
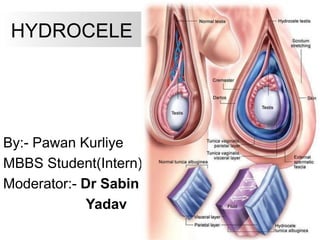
- 1. HYDROCELE By:- Pawan Kurliye MBBS Student(Intern) Moderator:- Dr Sabin Yadav
- 2. Content • What is hydrocele? Definiton? • Developmental Anatomy • Risk factors & Etiology • Classification & Types • Signs & symptoms • Physical assessment & Dx • Complication of Hydrocele • Differential Dx • Management (Surgical Tx & complications) • Mind Map • Clinical case Scenario • Reference
- 3. INTRODUCTION Hydrocele is an abnormal collection of serous fluid between the visceral and parietal layers of the tunica vaginalis.
- 5. Layers of Scrotum SKIN DARTOS MUSCLE EXTERNAL SPERMATIC FASCIA (external oblique) CREMASTRIC MUSCLE (internal oblique) INTERNAL SPERMATIC FASCIA (Facia Transversalis) TUNICA VAGINALIS
- 6. Arteries and veins of testis Testicular Artery • It is a branch of abdominal aorta • Descends on the posterior abdominal wall • It traverses the inguinal canal and supplies the testis and the epididymis Testicular Veins • These are the extensive venous plexus, the pampiniform plexus • Leaves from the posterior border of the testis • As the plexus ascends, it becomes reduced in size so that at about the level of deep inguinal ring, a single testicular vein is formed • Drains into left renal vein on left side and inferior vena cava on right side
- 7. Risk factors Most hydroceles are present at birth (congenital), and babies who are born prematurely have a higher risk of having a hydrocele. Hydrocele generally affects men 40 or older: • Scrotal injury (Traumatic/Iatrogenic), • Infection including sexually transmitted infections, • Tumours & Radiation Therapy
- 8. ETIOLOGY For baby boys, a hydrocele can develop m the womb. Normally, the testicles descend from the developing baby's abdominal cavity into scrotum. A sac (processus vaginalis) accompanies each testicle, allowing fluid to surround the testicles. In most cases, each sac closes and the fluid is absorbed. However, if the fluid remains acer the sac closes, the condition is known as a NONCOMMUNICATING HYDROCELE. Because the sac is closed, fluid can't flow back into the abdomen. Usually the fluid gets absorbed within a year. In some cases, however, the sac remains open. With this condition, known as COMMUNICATING HYDROCELE,the sac can change size or,if the scrotal sac is compressed, fluid can flow back into the abdomen. In older males, a hydrocele can develop as a result of inflammation or injury within the scrotum.Inflammation may be result of infection of the small coiled tube at the back of each testicle (epididymitis) or of the testicle.
- 10. CONGENITAL HYDROCELE NONCOMMUNICATING HYDROCELE - patent processus vaginalis obliterates but fluid remains. COMMUNICATING HYDROCELE - the sac remains open in communication with the peritoneal cavity.
- 11. CONGENITALHYDROCELE: PROCESSUS VAGINALIS COMMUNICATES WITH PERITONEAL CAVITY..... INFANTILE HYDROCELE: TUNICA & PROCESSUS VAGINALIS DISTENDED UPTO INTERNAL RING BUT SACHAS NO CONNECTION WITH PERITONEAL CAVITY
- 12. ENCYSTED HYDROCELE OF CORD: PARTOF FUNICULAR PROCESS PATENT, &IS CLOSED FROM THE TUNICA VAGINALIS BELOW & PERITONEAL CAVITYABOVE. SMOOTH,OVAL SWELLING ASSOCIATED WITH SPERMATIC CORD. TRACTION TEST +ve
- 13. HYDROCELE EN BISSAC TWO INTERCOMMUNICATING SACS ABOVE & BELOW NECK OF SCROTUM Operated at Midnapur Medical College, West Bengal (2008)
- 14. HYDROCELE OF CANALOF NUCK: • OCCURS IN FEMALES • IN THE INGUINALCANAL • THE CYST LIES IN RELATION ROUND LIGAMENT • SIMILAR TO HHYDROCELE OF THE CORD(ENCYSTED HYDROCELE)
- 15. HYDROCELE OF HERNIAL SAC: NECK OF THE HERNIAL SAC BECOMES CLOSED BY ADHESIONS OR PLUGGED BY OMENTUM. RESULTS IS RETENTION OF FLUID SECRETED BY PERITONEUM OF HERNIAL SAC
- 16. Primary Hydrocele - Clinical Pictures
- 17. INFECTIONS: FILARIASIS TUBERCULOSIS OF EPIDIDYMIS SYPHILIS INJURY POST HERNIORRHAPHY HYDROCELE POST VARICOCELECTOMYHYDROCELE TRAUMA TUMOUR MALIGNANCY SECONDARYHYDROCELE
- 18. COMMON IN COASTAL/TROPICAL REGIONS , ACCOUNTS FOR 80 % OF ALL HYDROCELES IN TROPICAL REGIONS, CAUSED BY Wucheria bancrofti REPEATED ATTACKS OF FILARIAL EPIDIDYMITIS SIZE- LARGE SIZE WITH THICKENED SAC OCCASIONALLY CONTAINS CHOLESTEROL RICH FLUID – CHYLOCELE DUE TO RUPTURED LYPMH VARIX WITH DISCHARGE OF CHYLE IN TO THE HYDROCELE RESEMBLES PRIMARY HYDROCELE MAY BE ASSOCIATED WITH FILARIAL ELEPHANTIASIS. FILARIAL HYDROCELE
- 19. 1. INFECTION 2. PYOCELE,HEMATOCELE/CLOTTED HEMATOCELE 3. CALCIFICATION OF SAC 4. ATROPHY OF TESTIS 5. HERNIATION OF HYDROCELE SAC (rare)pure scrotal swelling 6. RUPTURE (rare) 7. INFERTILITY (rare) COMPLICATIONS OF HYDROCELE:
- 20. SIGNS & SYMPTOMS In the early stages hydroceles are usually asymptomatic. As they enlarge they bulge out and can become a cosmetic problem. Symptoms can develop, as the swelling increases in size, which include: Heaviness, fullness, or dragging sensations due to an enlarged scrotum. There may be mild discomfort radiating along the inguinal area to the mid portion of the back. If pain develops in a Hydrocele it is usually an indication of acute epididymal infection or due to overstretched scrotal skin in huge hydroceles. The size may decrease with recumbency or increase in the upright position. Fever, chills, nausea, or vomiting indicate an infection of a hydrocele.
- 21. PHYSICAL ASSESSMENT Smooth, cystic mass completely surrounding the testis and not involving the spermatic cord(Possible to get above the swelling) is characteristic of a hydrocele. The consistency of hydroceles can vary with position. Sometimes a hydrocele can become smaller and softer on lying down and become larger and tenser after prolonged standing. Getting above theSwelling When the fluid in the hydrocele is clear, Transillumination is positive. Transillumination may be negative in filarial hydrocele due to prescence of chyle, calcification or in complicated hematocele/pyocele
- 22. Getting above the swelling positve Transillumination positive Fluctuation positive Non reducible swelling Impulse on coughing negative (positive in congenital hydrocele) Testis cannot be palpated separately. (exception - funicular hydrocele a.k.a encysted hydrocele) Why is it Hydrocele?
- 23. IMAGING STUDIES Uncomplicated hydroceles do not require radiographic studies. Findings from USG can help evaluate for an underlying process, such as a tumour or torsion. Composition of Hydrocele Fluid • Color -Straw or amber colored. • Composition Water, fibrinogen, inorganic salts, albumin and cholesterol crystals • Hydrocele fluid normally won't clot if it is drained into a container but will clot immediately even if it comes into contact with a drop of blood
- 24. 1. TESTICULAR TUMOUR 2. EPIDIDYMAL CYST 3. SPERMATOCELE 4. EPIDIDYMO-ORCHITIS 5. TESTICULAR CARCINOMA DIFFERENTIAL DIAGNOSIS
- 25. In Children(congenital hydrocele), A Non-communicating Hydrocele usually resolves spontaneously by the time the child reaches the age of 1 year. A hydrocele that persists longer than 12 to 18 months is usually a Communicating Hydrocele & requires inguinal Herniotomy...... In Adults, Treatment depends upon the age of the patient and the degree of discomfort caused by the hydrocele. Surgical excision forms the definitive therapy for hydroceles. When they are small and asymptomatic, hydroceles require no treatment other than reassurance. Indications for surgery – Scrotal discomfort or pain Cosmetic - disfigurement due to the sheer size of the hydrocele. TREATMENT
- 26. Techniques include LORDS PLICATION used for small to medium hydroceles with thin sac. Benefits - reduced risk of hematoma.. Some articles suggest a slight incidence of recurrence of the hydrocele following this procedure. JABOULAYS OPERATION used for large size hydrocele,after I & D,the sac is everted and sutured behind the testis, associated with a reduced risk of recurrence, may have an increased risk of hematoma. SHARMA & JHAWERS TECHNIQUE after evacuation, the sac with the testis is placed in a neewly creatd pocket between the fascial layers of the scrotum Encysted Hydrocele- Inguinal herniotmy + Incision & drainage of the encysted hydrocele
- 28. Primary Hydrocele -Operative pics
- 29. INJURY TO VAS DEFERENS INJURY TO URETHRA INJURY TO TESTIS/EPIDIDYMIS REACTIONARY HAEMORRHAGE - Hematocele INFECTION - Pyocele SINUS FORMATION between layers RECURRENT HYDROCELE COMPLICATIONS OF SURGERY
- 30. Mind map
- 31. Classic Clinical case of Hydrocele • A 42-year-old male patient presents with right sided scrotal swelling of two years duration. It is a progressively increasing painless swelling. • O/E: the right side of the scrotum shows a swelling of 15 x 10 cm size which is confined to the scrotum (can get above the swelling). The surface of the swelling is smooth and borders are well-defined. There is no local rise of temperature. The swelling is fluctuant and transilluminant. It is not reducible.There is no cough pulse. The right testis is not felt separately. • The spermatic cord is felt above the swelling and is tender. • The contralateral testis and genitalia are normal. There is no evidence of any mass or lymph nodes in the abdomen
- 32. Reference • Bailey and Love-Short Practice of Surgery • Manual on Clinical Surgery -Somen.Das
Editor's Notes
- Testis descends from the posterolateral genitourinary ridge at the beginning of the third trimester of fetal gestation, a saclike extension of peritoneum descends in concert with the testis. As descent progresses, the sac envelops the testis and epididymis. The result is a serosal-lined tubular communication between the abdomen and the tunica vaginalis of the scrotum. The peritoneum-derived serosal communication is the processus vaginalis, and the serosa of the hemiscrotum becomes the tunica vaginalis. At term, or within the first 1-2 years of life, the processus vaginalis of the spermatic cord fuses, obliterating the communication between the abdomen and the scrotum. The processus fuses distally as far as the lower epididymal pole and anteriorly to the upper epididymal pole. Failure of complete fusion may result in communicating hydroceles, indirect inguinal hernias, and the bell- clapper deformity of abnormal testicular fixation in the scrotum.
- A hydrocele can be produced in four ways: -by excessive production of fluid within the sac, e.g. secondary hydrocele -through defective absorption of fluid -by interference with lymphatic drainage of scrotal structures as in case of elephantiasis -by connection with a hernia of the peritoneal cavity in the congenital variety, which presents as hydrocele of the cord
- Most common type of hydrocele is Vaginal hydrocele in which the process is obliterated & there is accumulation of fluid between the layers of tunica vaginalis ,there is called vaginal hydrocele
- Congenital hydrocele: in simple words there is communincation betweeen scrotal sac & peritoneal cavity. Characteristics feature of communicating hydrocele is Diural Variation i.e when a baby gets up early in morning , there won't be any swelling bcz throught the night baby was lying down as the DAY goes on, slowly the fluid in the peritoneal cavity will come down into the scrotum,baby will develop swelling towards afternoon or evening.
- Traction test +ve which means when we pull down particular testis,along with testis the encysted hydrocele will also come down
- Bilocular Hydrocele(rare): there will be cyst in the scrotum & another cyst in between muscles of ant. abd.wall musculature & this two cyst will be interconnected, so if we press one cyst, we can see movement in other cyst also which we can call cross fluctation test is +ve in this case.
- 1st pic(top left): Boy with right side hydrocele,if a baby is born with this type of swelling we should not do any surgery immediately,we can wait upto 2 years & then procede with any surgical option bcz we can assume in this case it's a communicating hydrocele in which there is connection between scrotal sca & peritoneal cavity,it will reside by its own over the time or whe need to do herniotmy to repair. 2nd pic: Adult hydrocele Bilateral variety(big size) penis is also buried in scrotum & it is an surgical emergency bcz patient will have problem in voiding urine and also At the time of urination,some urine will fall on skin & it can cause alkaline dermatitis. 3rd pic(top right): Doctor is trying to get above the swelling & try to feel the spermatic cord there so that he can conclude swelling is confined to scratal region only. 4th pic(bottom left):Doctor is performing transillumination test. we can do this test lateral to medial or medial to lateral but not psoterior bczit will give false negative result due to inteference of testis. 5th pic: Doctor is performing Traction test- in this test when we pull the testis, along with testis encysted hydrocele will also come down. Last pic(bottom right): Filarial hydrocele very biz in size.
- 1st pic: Hematocele 2nd pic: Pyocele Last pic: Hernia of the hydrocele sac, hydrocele sac will burrow through layers of scrotum including dartos muscles & it will just lie benath the skin
- EXAMINATION OF HYDROCELE Position : standing Exposure : from the abdomen till both knees INSPECTION Side . Unilateral or bilateral . Inguinal , scrotal or inguino-scrotal . Testis: included or separate . Penis : Normal or pushed or buried Shape : Pyriform or Globular Size: Approximate size eg: potato Skin over . Edema , redness . sloughing or gangrene . Dilated veins . Ulcer , sinus (Post.: T.B , Ant. : tumor) . Scars PALPATION Superficial: for hotness , tenderness Deep :- . Scrotal neck test . Surface . Reducibility . Consistency . Cough impulse or thrill . Relation to testis (within or can be felt separate) . Relation to the cord (Hydrocele of the cord & Mobility when testis is pulled down) Healthy testis , cord General : Abdominal mass , PALN , Wirchow LN , Prostate , spines
- Getting above the swelling -ve : Infantile & encysted hydrocele. Transillumination test -ve: Hematocele,pyocele,chylocele,thickened sac
- Laboratory evaluation is generally not essential to the evaluation of hydrocele & hernias Leukocytosis may be sign of strangulated hernia. Leukocytosis with higher perceantage of neutrophils suggests an infection and/or inflammatory process(eg.epidydymo-orchitis)
- congenital hydrocele: there is connection between hydrocele sac & peritoneal cavity,we have to disconnect that patent process vaginalis ,so we have to do inguinal herniotomy
- 1st pic(top left corner): Adult hydrocele-incision over the scrotum which is seperating different layers of the scrotum. 2nd pic: Tuninca vaginalis is completely seperated,then would have made a nick incision & fluid is coming out. 3rd pic(top right corner): There is lot of fluid in kidney tray & still there is lot a fluid in sac . 4th pic : We can clearly see it's Jabouley's procedure in which fluid is evacuated, the sac is everted & sutured behind the testis Last pic: we can see it's a pressured scrotal dressing.