
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Actinomycosis
Similar to Actinomycosis (20)
Recently uploaded
Recently uploaded (20)
Actinomycosis
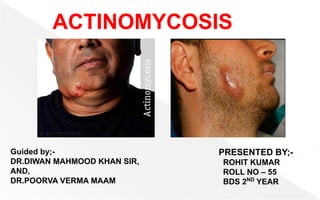
- 1. ACTINOMYCOSIS Guided by;- DR.DIWAN MAHMOOD KHAN SIR, AND, DR.POORVA VERMA MAAM PRESENTED BY;- ROHIT KUMAR ROLL NO – 55 BDS 2ND YEAR
- 2. CONTENTS ⦿ Introduction ⦿ Morphology ⦿ Pathogenesis and Immunity ⦿ Clinical Syndromes(ACTINOMYCOSIS) ⦿ TYPES OF ACTINOMYCOSIS ⦿ Epidemiology ⦿ Laboratory Diagnosis ⦿ Treatment ⦿ Prevention and Control
- 3. INTRODUCTION ⦿ Actinomycosis is caused by Actinomyces. ⦿ Which are considered to be a transitional forms between bacteria and fungi. ⦿ Actinomyces israeli is the most common Actinomyces causing human infection. ⦿ In human, Actinomyces species uasually cause diseases like;- -Cervicofacial actinomycosis -Thoracic actinomycosis, -and, Actinomycosis of the abdomen and pelvis.
- 4. MORPHOLOGY Actinomyces show the following features:- ■ Actinomyces organisms are Gram-positive, nonmotile, nonsporing,and non–acid-fast bacilli. ■ They measure 0.5–1 mm in diameter. ■ They often grow in filaments that separate into bacillary and coccoid filaments.
- 5. PATHOGENESIS & IMMUNITY ⦿ Actinomyces species are present as normal flora of the oral cavity and also in the lower gastrointestinal tract and female genital tract of human hosts. ⦿ Establishment of human infection by Actinomyces always requires the presence of companion bacteria. ⦿ These companion bacteria help in initiation of infection by producing a toxin or enzyme or by inhibiting host immunity. ⦿ Infection by Actinomyces typically spreads contiguously and invades surrounding tissues and organs.
- 6. • Finally, the infection results in the production of draining sinus tracts, which contain lot of damaged tissue. • And the Bacteria from this site may disseminate through blood circulation to distant organs. Continues…
- 7. CLINICAL SYNDROME (ACTINOMYCOSIS) - Actinomyces causes actinomycosis. ❑ ACTINOMYCOSIS- - Actinomycosis is a subacute and chronic bacterial infection characterized by contiguous spread and suppurative and granulomatous inflammation. Figure - Actinomycosis, sites and routes of infection
- 8. -Actinomycosis may manifest as (a)cervicofacial actinomycosis, (b) thoracic actinomycosis, and (c) actinomycosis of the abdomen and pelvis. - The condition is associated with the formation of multiple abscesses and development of sinus tracts discharging white to yellowish granules, known as sulphur granules.
- 9. TYPES OF ACTINOMYCOSIS ⦿ CERVICOFACIAL ACTINOMYCOSIS- - It is the most common manifestation in humans comprising about two-thirds of reported cases. - The infection occurs in the cervicofacial region, which typically occurs following oral surgery in patients with poor oral hygiene. Fig- cervicofacial actinomycosis
- 10. -Initially, the condition manifests as a swelling of the soft tissue of the perimandibular area. -during the course of the infection, the disease spreads and leads to formation of fistulas. -These fistulas or sinus tracts discharge purulent material containing yellow granules, known as sulfur granules. - If left untreated, this condition may spread to the blood and eventually to the brain and to the orbit.
- 11. Fig- cervicofacial actinomycosis in tooth
- 12. •THORACIC ACTINOMYCOSIS- -This condition is responsible for 15-20% of cases of actinomycosis. -It is caused by aspiration of oropharyngeal secretions containing Actinomyces and occasionally during perforation of the esophagus. -The condition commonly presents as apulmonary infiltrate or mass involving the lung. fig- thoracic actinomycosis
- 13. -The condition, if left untreated, can spread outwardly through the pleura, pericardium, and chest wall, ultimately leading to the formation of multiple sinuses that discharge sulfur granules.
- 14. •ACTINOMYCOSIS OF THE ABDOMEN AND PELVIS- -This condition accounts nearly 10-20% of reported cases. - The ileocecal region is the most common site involved in the condition. -The condition typically presents as a slowly growing tumor. fig- pelvic actinomycosis
- 15. -The infection subsequently spreads and involves abdominal organs including the abdominal wall, leading to the formation of draining sinuses. - Actinomycosis of pelvis is commonly associated with prolonged (for many years) use of intrauterine contraceptive devices. The infection spreads directly from uterus to pelvis.
- 16. EPIDERMIOLOGY ⦿ Actinomycosis is distributed worldwide. The condition is more common in rural areas and in farm workers. ⦿ The condition is seen more commonly in individuals with poor dental hygiene and in the people with low socioeconomic conditions. ⦿ Men are affected more commonly than women (male to female ratio is 4:3) with the exception of pelvic actinomycosis. ⦿ Majority of the cases are reported in young and middle-aged patients.
- 17. LABORATORY DIAGONOSIS ⦿ Laboratory diagnosis is made by direct detection of Actinomyces in specimens by microscopy and by isolation of organism by culture. ◗ Specimens- - The specimens include sputum, bronchial secretions and discharges,and infected tissues. - All these specimens may contain large number of sulfur granules. - The sulfur granules are also present on the dressings removed from a draining sinus tract.
- 18. ◗ Microscopy- -Sulfur granules are white to yellow and vary in size from minute specs to large granules. -These granules are separated from pus and other specimens and are collected directly from draining sinuses. - These are crushed between two slides and are stained by Gram or Ziehl–Neelsen staining method, using 1% sulfuric acid for decolorization.
- 19. -The stained smears on microscopic examination show Gram-positive hyphal fragments surrounded by peripheral zone of swollen, radiating, club-shaped structures presenting a sunray appearance. -These club-shaped structures are Gram positive, acid fast, and are believed to be antigen complexes.
- 20. Figure - Actinomycosis. Microscopic appearance of sulphur granule lying inside an abscess. The margin of the colony shows hyaline filaments highlighted by Masson’s trichrome stain (right photomicrograph).
- 21. DIAGONOSTIC TECHNIQUES ⦿ Molecular Diagnosis DNA probes and PCR (polymerase chain reaction) have been evaluated and used with high sensitivity and specificity for accurate identification of Actinomyces species in clinical specimens.
- 22. ◗ CULTURE- -Sulfur granules or pus-containing Actinomyces are immediately cultured under anaerobic conditions at 35-37°C for up to 14 days. -The specimens are inoculated on blood agar, BHI agar, and into thioglycollate broth and incubated anaerobically at 37° C. -A.israeli produces(1-5mm) large, white,smooth,entire lobulated colonies resembling molartooth after 10 days of anaerobic incubation. Fig- Molar tooth-shaped colonies of Actinomyces israelii on blood agar.
- 23. TREATMENT ⦿ High-dose penicillins or tetracyclines given over a prolonged period are the mainstay of therapy for actinomycosis. ⦿ Metronidazole, cotrimoxazole, and sulfamethoxazole, and penicillinase-resistant penicillins, such as methicillin, oxacillin, and cloxacillin do not have activity against Actinomyces species. ⦿ Surgical therapy is included for more extensive and complicated cases of actinomycosis.
- 24. PREVENTION & CONTROL ⦿ Good dental hygiene and oral hygiene are important in prevention of the disease.
- 25. * Source of information- - Textbook of microbiology by- subhash Chandra parija and cp baveja - Images courtesy- google and different books