Presentation1, radiological imaging of popliteal fossa masses.
•Download as PPTX, PDF•
24 likes•9,048 views

Health& Medicine

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Presentation1, radiological imaging of popliteal fossa masses.
Similar to Presentation1, radiological imaging of popliteal fossa masses. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1, radiological imaging of popliteal fossa masses.
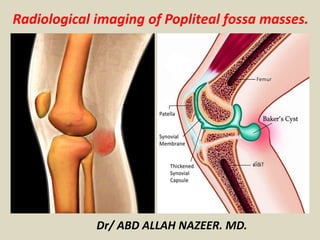
- 1. Radiological imaging of Popliteal fossa masses. Dr/ ABD ALLAH NAZEER. MD.
- 2. Axial PD MRI of the popliteal fossa.
- 3. Coronal PD MRI of the popliteal fossa.
- 4. SYNOVIAL Pigmented villonodular synovitis (PVNS): PVNS: Knee (80%) > ankle > hip > shoulder > elbow Unknown etiology - possibly a reactive inflammatory process Abnormal synovium prone to hemorrhage Hemosiderin deposits in synovium and with nodule formation due to repeated hemorrhagic effusions Managed as low-grade, locally aggressive neoplasm. Imaging features: MRI diagnostic in 95% of cases: Gradient echo imaging shows "blooming" phenomenon of hemosiderin-laden nodules. Large effusion +/- erosions. Intense inhomogeneous enhancement.
- 5. MRI PD FS sagittal (a) and T1 axial (b) demonstrating a large posterior intra-articular lobulated mass with villonodular proliferation of hemorrhagic synovium demonstrated areas of low signal intensity representing hemosiderin (red arrows). Typical imaging appearances of PVNS which was histologically confirmed.
- 6. Typically appearances of PVNS. Radiograph of the knee (a) demonstrates increased soft tissue density in the posterior aspect of the knee (red arrow). MR confirmed a large intra-articular lobulated lesion with areas of nodular low signal intensity regions (hemosiderin) seen on sagittal PD (b) which 'blooms' on axial T2* gradient echo (c).
- 7. MRI PD sagittal (a) demonstrating a well-defined low signal lesion abutting the posterior cruciate ligament which demonstrates intense inhomogeneous enhancement post contrast on sagittal (b) and axial (c) T1FS which is typical for PVNS. Contrast can make small lesions more conspicuous but usually not required. Pre T1FS not shown.
- 8. Pigmented villonodular synovitis. PD-weighted MRI sequences, both in the sagittal plane, showing nodular synovial thickening interspersed with hypointense foci, especially in the suprapatellar and posterior recesses of the knee.
- 9. Synovial chondromatosis: Knee (50-65%) > hip > shoulder > elbow Benign neoplastic synovial proliferation and formation of cartilaginous (chondromatosis) or osseous bodies (osteochondromatosis) Malignant transformation is extremely rare and no reliable distinguishing feature. Imaging features: Multiple, round, similar-sized calcified bodies seen on radiograph. 80% have erosions detectable by MR Bodies are of variable MR signal, depending on proportion of calcium, chondroid, and mature ossific tissue.
- 10. Lateral radiograph of the knee (a) and sagittal gradient echo T2* (b) demonstrates innumerable tiny ossified bodies both in the anterior and posterior joint space. Numerous bodies can become conglomerate, appearing as a "mass" within the joint as in this case. This was a case of biopsy proven synovial osteochondromatosis.
- 11. Synovial chondromatosis. Sagittal proton density (PD)-weighted MRI scans with fat suppression. Multiple intra-articular loose bodies located in the suprapatellar recess (arrow) and posterior recess (asterisk), where a popliteal cyst (Baker's cyst) can be seen.
- 13. BURSAL: Baker's cyst: Fluid-filled sac with neck arising from interspace between gastrocunemeous muscle and semimembranosus tendon. Contralateral subclinical Baker cysts common. Imaging features: Must see neck arising from medial gastrocunemeous- semimembranosus tendon interspace to make diagnosis of Baker cyst. Characteristic "talk-bubble" configuration on transverse scans Free fluid tracking adjacent to cyst indicates recent leakage. Acute pain suggestive of rupture or hemorrhage into cyst
- 14. Axial PD MRI of the popliteal fossa demonstrating the characteristic appearance of a Baker's cyst. A cystic structure with a 'talk bubble' configuration is seen arising between the tendons of the medial head of the gastrocunemeous and semimembranosus muscles.
- 15. Transverse ultrasound (a) demonstrates a large echogenic solid lesion in the popliteal fossa with no increased Doppler signal. T1 axial (b) and sagittal (c) demonstrates a large T1 hyperintense collection arising between the medial head of the gastrocunemeous (blue arrow) and semimembranosus tendon (red arrow) in keeping with a large hemorrhagic Baker's cyst. Signal loss of the knee joint due to total knee arthroplasty.
- 16. Baker's cyst. A 48-year-old male presented with swelling in the popliteal fossa: sagittal (A) and axial (B) T2W gradient-echo images show a distended gastrocnemius--semimembranosus bursa (arrows).
- 17. SOFT TISSUE: Ganglion: Myxoid tissue encased in a fibroblastic collagenous wall (pseudocapsule) with no synovial lining Arises from joint or tendon but intraosseous (Muir et al) or intramuscular (Parks et al) locations have been reported In the knee, commonly arises from cruciate ligaments or joint capsule. Imaging features: T2: Uniformly hyperintense soft tissue cystic mass
- 18. MR STIR axial (a), coronal (b) and sagittal (c) of the knee demonstrating a uniformly T2 hyperintense multilobulated soft tissue cystic mass arising from the posterior knee joint capsule which was histologically proven as a ganglion.
- 19. Standard non-contrast PD sequenced MRI scans revealing ganglion cyst arising from ACL, enveloping ACL fibres and predominantly extending posteriorly.
- 20. Ganglion Cyst of ACL.
- 21. 2 cm cyst in the posterior intercondylar notch, mainly surrounding the PCL and Humphrey's ligament.
- 22. Lipoma: Benign lipomatous tumour composed of mature adipose tissue representing almost 50% of soft tissue masses. Well-defined, oblong-shaped encapsulated mass with fine linear striations parallel to long axis of tumour Characterised by location as: 1-superficial to the deep fascia 2-deep to the deep fascia 3-intramuscular . Imaging features: Should be similar to subcutaneous fat on any imaging modality.
- 23. AP and lateral radiographs of the knee demonstrating increased fat density within the soft tissues of the posteromedial aspect of the knee (blue arrow). Note how this is similar to the normal density of the suprapatellar pouch that contains fat (red arrow) suggesting this mass is fatty in nature. Lipomas follow fat density/signal on all modalities.
- 24. Axial (a) and coronal (b) T1 and corresponding axial (c) and coronal (d) fat suppressed MRI sequences demonstrating the fatty lesion seen in the radiograph of Figure 10. The lesion is high signal on T1 in keeping with fat and demonstrates complete suppression in keeping with a lipoma. Due to its size biopsy was performed confirming a simple lipoma.
- 25. Lipoma arborescens. PD-weighted MRI sequences, both in the sagittal plane, with fat suppression (A) and without (B), showing intra-articular anomalous tissue, with a frond-like aspect, presenting a hyperintense signal in the PD-weighted sequences without fat suppression and showing a reduction in the signal strength when fat suppression is applied. Moderate joint effusion can also be seen.
- 26. Fibromatosis: Spectrum of benign fibroblastic disorders with tendency to infiltrate adjacent tissues Tendency for local recurrence (65%) without metastasis. Imaging features: Intense enhancement post contrast Extends along fascial planes Locally infiltrative US: Nonspecific soft tissue mass, variable echogenicity, smooth well-defined margins. non-contrast CT: Soft tissue mass hyperdense to muscle MRI: T1 - Hypointense to muscle; T2 - Hyperintense with bands of hypointense signal regions (fibrous components).
- 27. Axial T1 (a), axial STIR (b) and corresponding T1 and STIR coronal MRI images (c) and (d) respectively, demonstrate a soft tissue mass hypointense to skeletal muscle (blue arrow) that was low signal on all sequences. There curvilinear areas of low signal represent areas of mature collagen.
- 29. Fasciitis: Benign mass-forming fibrous proliferation Extension of mass along fascia suggests diagnosis Three types: Subcutaneous = well-circumscribed round nodule attached to fascia extending into superficial fat Fascial = poorly circumscribed fascial mass with satellite growth pattern Intramuscular = ovoid intramuscular mass attached to fascia. Imaging features: Similar intensity to skeletal muscle on T1, intermediate to high signal intensity on T2 Enhancement depends on myxoid and fibrous content.
- 30. MRI depicting intra-articular nodular fasciitis. Axial T2-weighted (A), sagittal T2-weighted (B), and sagittal T1-weighted (C) images.
- 31. Sagittal T1 (a) demonstrates a soft tissue lesion anterior to the popliteal vessels which is similar intensity to skeletal muscle on T1 and high signal intensity on axial STIR (b). Pre (c) and post (d) contrast T1FS demonstrates predominantly peripheral enhancement. Biopsy of the lesion confirmed proliferative fasciitis.
- 32. Epidermal inclusion cyst: benign lesion formed by the inclusion of dermal squamous epithelium with retention of keratinous debris and cholesterol or sebaceous materials Well-circumscribed subcutaneous mass. Imaging features: T1 isointense to muscle with mild heterogeneous signal ranging from low to high signal T2 Hyperintense signal with low or high signal debris. Absent to low-level central contrast enhancement with enhancing capsule.
- 33. Transverse ultrasound image of a superficial subepidermal lesion with internal speckles and posterior acoustic enhancement. This lesion was histologically confirmed as an epidermal inclusion cyst - though the classic 'pseudotestis' appearance is not seen.
- 34. Axial MR images of the knee. Dermal soft tissue session seen in figure 15 is low on T1 (a) and high on T2 (b) with internal low signal debris. Post contrast T1FS (c) demonstrates only subtle peripheral enhancement. Biopsy proven epidermal inclusion cyst.
- 35. Heterotopic ossification/Myositis ossificans: Benign Heterotopic formation of bone and cartilage in soft tissue. Stem cells for osteoid production exist within affected soft tissues Stimulus is usually traumatic though it may be in apparent or forgotten by patient. Imaging features: Evolving radiographic stages with stages of bone development (indistinct soft tissue through to mature bone formation) Peripheral bone formation with central immature bone (versus parosteal osteosarcoma which has organized bone centrally, less mature bone peripherally).
- 36. AP and lateral radiographs of the knee demonstrates ossification of the soft tissues at the posterior aspect of the knee. Importantly, no connection to the femur is seen and periosteal reaction. Axial CT (b) and MR STIR (d) demonstrates bone density within the soft tissues posterior to the medial femoral condyle with no aggressive features. Differentials include heterotopic ossification but a parosteal osteosarcoma cannot be entirely excluded although less likely. Biopsy confirmed heterotopic ossification.
- 38. Soft tissue sarcoma: Malignant tumour that arises from connective (mesenchymal) tissue other than bone Classified according to tissue type rather than anatomical origin. Grow centrifugally from single focus Suspicious features include a soft tissue mass that is increasing in size, has a size >5cm or is deep to the deep fascia, whether or not it is painful Imaging features: Features depend on the type of tumour and may have, internal cystic component, myxoid tissue, fat, calcification or necrosis Large heterogeneous hypoechoic mass Usually located in deep (subfascial) tissues Well-encapsulated Usually hypervascular with disorganized vascular pattern on color Doppler imaging ± Myxoid tissue: Well-defined, intra-tumoral anechoic or hypoechoic areas. ± Necrosis: Poorly-defined hypoechoic areas. ± Calcification: Discrete intra-tumoral echogenic foci with acoustic shadowing. ± Hemorrhage: Ill-defined intra-tumoral echogenic areas without acoustic shadowing
- 39. Axial STIR (a) demonstrates a complex soft tissue lesion superficial to the deep fascia. Pre (b) and post (c) contrast T1Fs demonstrates heterogenous enhancement. Soft tissue sarcomas are tumors without specific imaging findings beyond solid enhancing, soft tissue mass and needs biopsy for histological diagnosis. Biopsy confirmed undifferentiated pleomorphic sarcoma.
- 40. NDIFFERENTIATED PLEOMORPHIC SARCOMA (formerly malignant fibrous histiocytoma): 5% are extensively hemorrhagic, presenting as fluctuant mass often misdiagnosed as hematoma Underlying malignancy should be excluded in patients thought to have spontaneous musculoskeletal hemorrhage. Imaging features: Calcification present peripherally in 5-20% Similar signal intensity to muscle on T1 MRI Heterogeneously hyperintense to muscle on fluid-sensitive sequences.
- 41. Axial T2FS (a) and sagittal T1 (b) MRI demonstrates a high T2/low T1 signal mass in the posterior aspect of the knee with internal areas of intermediate and low signal which bloom on sagittal gradient echo T2* (c) in keeping with calcification. This lesion was histologically proven as undifferentiated pleomorphic sarcoma.
- 42. LIPOSARCOMA: Liposarcomas account for approximately 10% of all soft tissue sarcomas Liposarcomas arise from fat cells and can occur anywhere in the body. There are 6 different sub-types; the most common are: 1-well-differentiated liposarcoma, 2-pleomorphic liposarcoma 3-myxoid liposarcoma Imaging features: Non-specific soft tissue mass with myxoid and fat tissue ~< 25% fat.
- 43. Transverse ultrasound of the knee demonstrates a fatty lesion with increased Doppler signal (a). Panoramic ultrasound view (b) of the lesion demonstrates a large fatty lesion. Axial STIR MR (c) and T2 sagittal (d) demonstrates mixed signal intensity mass with heterogeneous enhancement (e) post contrast (pre contrast T1FS not shown). Biopsy confirmed a myxoid liposarcoma.
- 44. SYNOVIAL SARCOMA: Contrary to name, synovial sarcoma is not does not arise intra-articular or from synovium Malignant soft tissue tumour with predilection for juxta-articular regions of young patients especially popliteal fossa of knee or tendon sheath. Imaging features: Enhancing soft tissue mass near a joint Calcification, hemosiderin, cystic change, fluid-fluid levels relatively common.
- 45. Transverse ultrasound (a) demonstrates a soft tissue lesion with increased Doppler signal. Axial T1 MR (b) and sagittal T2FS (c) demonstrates a juxtaarticular low T1/high T2 soft tissue mass which enhanced post contrast (images not shown). Lesion proved to be a synovial sarcoma.
- 46. Synovial sarcoma. Fat-suppressed T1-weighted MRI sequences in the axial (A) and sagittal (B) planes, after intravenous injection of paramagnetic contrast. Voluminous multiloculated expansile lesion, with the "bowl of grapes" aspect, showing intense enhancement after contrast administration. The femoral cortical bone (arrow) is poorly defined.
- 47. a) Lateral radiograph showing scattered calcification in synovial chondromatosis (white arrow), and b) T2-weighted sagittal MR scan of the knee showing heterogenous malignant synovial chondromatosis (white
- 48. VASCULAR: Popliteal artery aneurysm: Popliteal artery is most common lower extremity location (70% of all peripheral aneurysms). Imaging features: Fusiform or saccular arterial enlargement, often with laminar thrombus within. Longitudinal panoramic view of the popliteal artery demonstrating a focal fusiform aneurysm with mural thrombus.
- 49. CT axial (a) and coronal reformat (b) demonstrating a right popliteal aneurysm (yellow arrow) which is completely occluded with thrombus.
- 50. MR axial (a) and coronal T1 (b), coronal STIR (c) demonstrating the occluded right popliteal artery which contains hyperintense T1 mural thrombus with central low signal material in keeping with chronic blood products. Image (d) is a zoomed up STIR coronal image demonstrate layers of differing blood products within the aneurysm.
- 51. Popliteal artery pseudoaneurysm. Sagittal PD-weighted MRI sequence (A) and sagittal fat-suppressed T1-weighted MRI sequence obtained after intravenous injection of paramagnetic contrast (B). Small bone projection from the tibial metaphysis (arrow) into the popliteal fossa, where there is an oval image with heterogeneous content, which shows partial enhancement by contrast, representing a partially thrombosed pseudoaneurysm.
- 52. Vascular malformations and hemangiomas: Hemangiomas are vascular tumours that are rarely apparent at birth, grow rapidly during the first 6 months of life, involutes with time and do not necessarily infiltrate but can sometimes be destructive Vascular malformation/arteriovenous malformation (AVM) is a diffuse mass of dilated tortuous serpiginous vessels involving both arteries and veins. In contrast to hemangiomas, they are present at birth, slow growing, infiltrative, and destructive Almost all AVMs and nearly 40% of hemangiomas eventually require intervention. Imaging features: Flow voids in high flow AVM High signal intensity on fat-suppressed T2 : Bright "bag of worms" Low T2 signal intensity foci may reflect phleboliths, scars or hemosiderin deposition best seen on gradient echo sequences.
- 53. MR Axial T1 (a), T2FS (b) and post contrast T1FS (c) demonstrating a low T1/High T2 soft tissue mass with intense enhancement. Intralesional low signal areas are suggestive of flow voids. Biopsy confirmed a hemangioma.
- 54. Hemangiopericytoma (HPC): Entity arising from pericytes with 70% being benign Characterised by its branching vascular pattern that (although can be seen in numerous benign and malignant tumours). Solitary fibrous tumour and hemangiopericytoma are histologically similar and currently used almost interchangeably and are thought of as being part of the same histopathologic spectrum. Lower extremity > retroperitoneum > head/neck > trunk > upper extremity Longitudinal ultrasound image (a) demonstrating a vascular soft tissue mass. Axial MR T2 (b) and sagittal T1 (c) demonstrates a predominantly hyperintense lesion with internal branching flow-voids (red arrows) in keeping with vessels. Biopsy proved a hemangiopericytoma.
- 55. Myopericytoma: Benign neoplasm thought to represent a subset of hemangiopericytoma (HPCs) WHO defines myopericytoma as a distinct entity encompassing myopericytoma and glomangiopericytoma. Arises from perivascular myoid cells. Imaging features: Typically well-defined subcutaneous mass typically occurring in the lower extremities. Isointense to muscle on T1 Hyperintense on T2 weighted sequences Intense enhancement post contrast MR axial STIR (a) and pre (b) and post (c) axial T1FS demonstrates an intermuscular mass more conspicuous post contrast. Biopsy confirmed a myopericytoma.
- 56. NEURAL: Peripheral nerve sheet tumour (PNST): Benign tumour arising from nerve; histologically classified as either schwannoma or neurofibroma Any peripheral nerve can be affected Intermuscular > subcutaneous > intramuscular. Imaging features: Typically fusiform or oblong-shaped and oriented along long axis of nerve. Nerve entering or exiting from tumor is seen in majority (90%) Posterior enhancement is common (70%).
- 57. Coronal (a) and axial (b) MR T2FS demonstrating the classical fusiform 'target' lesion with the nerve seen entering and exiting from the lesion in keeping with a peripheral nerve sheath tumour (PNST). Axial STIR MR of a neurofibroma which demonstrates the typical 'target' appearance of a nerve sheath tumour. Central (red arrow) fibrocollagenous component (low T2) surrounded by peripheral (blue arrow) myxoid component (high T2).
- 58. Peripheral nerve sheath schwannoma.
- 59. Synovial sarcoma. A 23- year-old male with palpable mass. (A) Sagittal T1W image demonstrates hypointense oblong mass in semimembranosus muscle (arrow), which has solid internal enhancement (arrow) on post-contrast T1W fat-saturated image (B). (C) Photomicrograph (H and E, ×200) shows a highly cellular spindle cell neoplasm composed of densely packed cells with scant cytoplasm. The tumor is characterized by its lack of nuclear pleomorphism and a mitotic rate that is lower than expected for such a cellular tumor, consistent with a synovial sarcoma.
- 60. Malignant peripheral nerve sheet tumour: Malignant spindle cell sarcoma of neural origin 25-70% associated with Neurofibromatosis 1 10-20% radiation-induced 5-10% of all soft tissue sarcomas Imaging features: Infiltrative, ill-defined, fusiform mass > 5 cm MR sagittal T1 (a) and axial STIR (b) demonstrates a large fusiform T2 hyperintense mass in the region of the common peroneal nerve. Biopsy confirmed a malignant peripheral nerve sheath tumour.
- 61. LYMPHOID: Non Hodgkin's Lymphoma: Extra nodal lymphoma soft tissue lymphoma is reported as <0.01% Must indicate to pathology if lymphoma is suspected to allow appropriate immunohistochemical analysis to be performed. Staging and management of lymphoma is drastically different compared to sarcomas Imaging findings: Infiltrative mass - encases neurovascular bundle Isointense to muscle on T1 Hyperinternse of T2 Contrast imaging does not add further to the tissue characterization: both homogenous and heterogenous enhancement post contrast has been reported.
- 62. Axial MR T1 (a) and STIR (b) demonstrates an ill-defined infiltrative soft tissue mass encasing the popliteal artery - typical of lymphoma. Axial CT angiogram (c) of the lower leg demonstrated a patent popliteal artery. Biopsy confirmed Non-Hodgkin's lymphoma.
- 63. MUSCULAR/TENDON: Giant cell tumour of tendon sheath (GCTTS): Benign synovial proliferation within tendon sheath, Same pathologic entity as pigmented villonodular synovitis (PVNS) but in a different location Lobulated soft tissue mass immediately adjacent to tendon Hand > wrist > ankle/foot > knee > elbow > hip Imaging features: Low T1 and T2 signal intensity soft tissue lobulated mass with intense inhomogeneous enhancement Low signal hemosiderin rim "blooms" on gradient echo imaging Sagittal T1 MR (a) and axial STIR (b) demonstrates a soft tissue mass with peripheral low signal rim on both sequences suggestive of hemosiderin. Biopsy confirmed a giant cell tumour of the tendon sheath.
- 64. Leiomyosarcoma: Vascular malignant neoplasm arising from smooth muscle Arises in skin, soft tissue, blood vessel Imaging features: Nonspecific soft tissue mass +/- calcification, necrosis, hemorrhage, or cystic change giving rise to fluid-fluid levels Aggressive lesion invading adjacent bone. AP radiograph (a) of the knee demonstrates abnormal increased soft tissue density in the medial aspect of the keen (blue arrow). Axial (b) and sagittal (c) STIR MR demonstrates a large soft tissue mass with multiple fluid-fluid levels (red arrows). Biopsy confirmed a leiomyosarcoma.
- 65. Parosteal osteosarcoma (differential diagnosis - heterotopic ossification/myositis ossificans): Low-grade osteosarcoma arising on surface of bone 65% of all lesions occur in the posterior cortex of the distal femoral metadiaphysis Fusiform mass along length of bone which tends to "wrap around" as it enlarges Initially associated with the surface and can present as an area of cortical thickening, and therefore be misinterpreted as a healing stress fracture As the mass grows, parts of it may be adjacent to cortex without being contiguous to it, giving appearance of "cleft" Bone is mature at site of origin, less mature at periphery [opposite ossification pattern of myositis ossificans
- 68. Chondrosarcoma: malignant cartilaginous tumours that account for 20-27% of all primary malignant bone tumours. Predominantly in the long bones Primary or secondary (osteochondroma, enchondroma) Multiple subtypes: conventional intramedullary chondrosarcoma (or central chondrosarcoma): juxtacortical chondrosarcoma: myxoid chondrosarcoma: extraskeletal chondrosarcoma Imaging features: 1-Destructive lesion with intralesional calcification (chondroid matrix) 2- High T2 signal of chondroid matrix 3- Heterogenous contrast enhancement
- 69. Lateral radiograph of the knee demonstrating areas of calcification within the soft tissue posteriorly (blue arrow). MR Sagittal T1 (b), sagittal (c) and axial (d) T2FS demonstrating high T2 signal mass. Biopsy confirmed an extraskeletal chondrosarcoma.
- 70. Thank You.