Juvenile idiopathic arthritis (JIA)
•Download as PPTX, PDF•
188 likes•57,972 views

Seminar presentation by 4th year medical student under supervision of a doctor. Reference is as in the slide presentation.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Juvenile idiopathic arthritis (JIA)
Similar to Juvenile idiopathic arthritis (JIA) (20)
More from yuyuricci
More from yuyuricci (20)
Recently uploaded
Recently uploaded (20)
Juvenile idiopathic arthritis (JIA)
- 1. JUVENILE IDIOPATHIC ARTHRITIS NIK NOR LIYANA BINTI NIK MD NOR SUHAIMI
- 2. INTRODUCTION Juvenile idiopathic arthritis presents as chronic joint swelling, pain with functional limitation for at least 6 weeks of unknown cause that starts before 16 year of age. U N K N O W N E T I O L O G Y A T L E A S T 6 W E E K S O N S E T B E F O R E 1 6 Y E A R S O L D
- 3. SIGN & SYMPTOMS A R T I C U L A R E X T R A - A R T I C U L A R 1. Joint swelling 2. Joint pain 3. Joint stiffness / gelling after periods of inactivity 4. Joint warmth 5. Restricted joint movements 6. Limping gait 1. General 2. Growth disturbances 3. Skin 4. Others 5. Enthesitis* *Inflammation of the entheses (the sites of insertion of tendon, ligament or joint capsule into bone)
- 4. SIGN & SYMPTOMS E X T R A - A R T I C U L A R General Fever, pallor, anorexia, loss of weight Growth disturbances General : Growth failure, delayed puberty Local : Limb length / size decrepency, micronagthia Skin Subcutaneous nodules Rash – systemic, psoriasis, vasculitis Others Hepatomegaly, splenomegaly, lymphadenopathy Serositis, muscle atrophy / weakness Uveitis : Chronic (silent), acute in Enthesitis related arthritis Enthesitis
- 5. CLASSIFICATION There are 3 major types of JIA: Some other less-common forms include: Enthesitis-related arthritis Psoriasis arthritis Undifferentiated arthritis 1. Oligoarticular JIA 3. Systemic JIA 2. Polyarticular JIA RF positive RF negative
- 7. OLIGOARTHRITIS WHAT IS OLIGOARTHRITIS? Oligoarticular arthritis occurs in 50% to 60% of young people who have JIA. It is the most common type of JIA in young people. It affects four or fewer joints in the first six months after diagnosis. There are two types of oligoarticular JIA: 1. Oligoarticular-persistent JIA 2. Oligoarticular-extended JIA. Subtypes Age at onset Diagnostic Persistent Extended < 6 years old Affects ≤4 joints throughout course of disease Affects >4 joints after the 1st 6 months of disease
- 8. OLIGOARTHRITIS O L I G O A R T I C U L A R – P E R S I S T E N T A R T H R I T I S Mildest form of JIA. Affects female > male . It most often affects the large joints such as the knee, ankle, wrist, and/or elbow joints. It can be associated with an eye disease called uveitis. It is rare to have permanent joint damage with appropriate treatment of this type of JIA.
- 9. OLIGOARTHRITIS O L I G O A R T I C U L A R – E X T E N D E D A R T H R I T I S This type of JIA also affects four or fewer joints in the first six months after diagnosis. However, after six months or more, patients with oligoarticular-extended arthritis develop arthritis in five or more joints. Oligoarticular-extended arthritis can affect both large and small joints.
- 10. OLIGOARTHRITIS
- 11. POLYARTHRITIS WHAT IS POLYARTHRITIS? • The second most common type of JIA in children and teens. Affects five or more joints within the first six months of being diagnosed with JIA. • There are two types of polyarticular arthritis: 1. Rheumatoid factor positive polyarticular JIA, associated with the presence of a rheumatoid factor antibody in the blood. 2. Rheumatoid factor negative polyarticular JIA, where there is no rheumatoid factor antibody in the blood. Subtypes Age at onset Diagnostic RF + RF - 6 – 7 years 9 – 12 years Affects ≥5 joints in the 1st 6 months of disease with negative RF Affects ≥5 joints in the 1st 6 months of disease with ≥2 positive RF tested at least 3 months apart
- 12. POLYARTHRITIS P O L Y A R T I C U L A R – R F P O S I T I V E A R T H R I T I S Common in young people over 10 years of age. Female > male It affects both the small joints of the hands and feet, and large joints like the knees, hips and ankles. It affects joints on both sides of the body. This type of JIA behaves the most like adult rheumatoid arthritis
- 13. POLYARTHRITIS P O L Y A R T I C U L A R – R F P O S I T I V E A R T H R I T I S With this type of JIA, your child may also have other symptoms: Rheumatoid nodules, which are hard bumps under the skin. Anemia. Significant fatigue Poor appetite, with some weight loss. Low grade fever A general feeling of being unwell These symptoms occur when the disease is active and untreated. The symptoms will improve with proper treatment.
- 14. POLYARTHRITIS P O L Y A R T I C U L A R – R F N E G A T I V E A R T H R I T I S It can occur at any age. Female > male Usually starts in many joints at the same time. Some young people only have polyarticular JIA for a limited period of time while others may have it for many years. This type of JIA is more likely to last into adulthood.
- 15. SYSTEMIC ARTHRITIS WHAT IS SYSTEMIC ARTHRITIS? Systemic arthritis is less common and affects only 10% to 15% of children and teenagers with JIA. It is often a more severe form of JIA. Systemic means it affects many parts of the body, rather than just the joints. Subtypes Age at onset Diagnostic Systemic 2 - 4 years old Affects ≥1 joints with or preceded by fever of at least 2 weeks duration, plus ≥1 of the following: Transient erythematous rash Enlargement of lymph nodes Hepatomegaly Splenomegaly Pericarditis ± pleuritis ± peritonitis
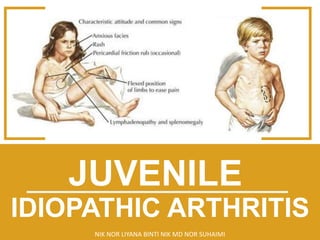
- 16. SYSTEMIC ARTHRITIS S Y S T E M I C A R T H R I T I S Boys = girls May range from mild to severe There is usually a spiking fever. This is a fever that rapidly rises and falls. The fever occurs once or twice every day. The JIA joint symptoms (joint pain or swelling) begin within six months after the fever first appears. Pale pink-red spots on the chest, upper arms, thighs, and other parts of the body. Swollen lymph glands are common. Enlarged spleen and liver
- 17. SYSTEMIC ARTHRITIS S Y S T E M I C A R T H R I T I S
- 18. SYSTEMIC ARTHRITIS S Y S T E M I C A R T H R I T I S
- 19. SYSTEMIC ARTHRITIS S Y S T E M I C A R T H R I T I S
- 20. ENTHESITIS ARTHRITIS WHAT IS ENTHESITIS ARTHRITIS? Enthesitis-related-arthritis involves inflammation in both the joints and the entheses, which are the spots where tendons or ligaments attach to bones. Subtypes Age at onset Diagnostic Enthesitis related 9 – 12 years old Arthritis ± enthesitis plus ≥2 of the following: Presence or history of sacroiliac joint tenderness &/or inflammatory lumbosacral pain Positive human leukocyte (HLA) B27 antigen Onset of arthritis in male >6 years old Acute anterior uveitis History of ankylosing spondylitis, enthesitis - related arthritis, sacroilitis w/ inflammatory bowel disease, Reiter syndrome, or family history of acute anterior uveitis
- 21. ENTHESITIS ARTHRITIS E N T H E S I T I S A R T H R I T I S
- 22. ENTHESITIS ARTHRITIS E N T H E S I T I S A R T H R I T I S Male > female Often lasts into adulthood. Usually involves just a few joints in the legs. The hips are often affected. Enthesitis is most common around the knees, ankles, and bottom of the feet. Knee, heel, and foot pain are common with activities. May affect the spine and the joints between the base of the spine and pelvis leading to neck or back pain and stiffness.
- 23. ENTHESITIS ARTHRITIS E N T H E S I T I S A R T H R I T I S
- 24. ENTHESITIS ARTHRITIS E N T H E S I T I S A R T H R I T I S Inflammation and swelling in the tendons of the fingers and toes making the fingers and toes look like sausages. This is called dactylitis. Inflammation of the small joints of the feet, called tarsitis. Enthesitis-related arthritis may be associated with inflammation of the skin or bowels.
- 25. PSORIATIC ARTHRITIS WHAT IS PSORIASIS AND PSORIATIC ARTHRITIS? Psoriasis is a skin disease. It is a scaly red rash that can develop on the scalp, behind the ears, on the eyelids, elbows, knees, buttocks, or in the belly button. Some people with psoriasis may also have pits or ridges in their fingernails. Children or teenagers with psoriasis also have arthritis. This is called psoriatic arthritis. Sometimes the psoriasis starts before the arthritis, but sometimes the arthritis begins before the psoriasis. A family history of psoriasis is an important clue to the correct diagnosis. Subtypes Age at onset Diagnostic Psoriatic 7 – 10 years old Arthritis ± psoriasis plus ≥2 of the following: Dactylitis Nail pitting & oncholysis Family history of psoriasis
- 26. PSORIATIC ARTHRITIS P S O R I A T I C A R T H R I T I S It can occur at any age. Male = female It can affect a few or many joints. May involve the hips or back. Associated with dactylitis. There is a moderate risk of uveitis
- 27. CLASSIFICATION
- 28. INVESTIGATIONS The diagnosis is essetially clinical – labolatory investigations are only supportive. 1. Full blood count – anaemia, leukocytosis and elevated platelets 2. ESR and peripheral blood film – markers of inflammation 3. X-ray/s of affected joint(s) - to look for malignancy 4. Antinuclear antibody – identifies risk factors for uveitis 5. Rheumatoid fever – assess prognosis in polyarthritis for early tx 6. Others Complement levels ASOT Ferritin Immunoglobulins (IgG, IgA and IgM) HLA B27 Synovial fluid aspiration
- 29. INVESTIGATIONS
- 30. TREATMENT There is no known cure for JIA. However, there are safe and effective medications to help control the disease. These medications help to: 1. Decrease the inflammation 2. Decrease pain and swelling 3. Make it easier for your child to stay active and exercise 4. Prevent or lessen damage to the joints. 5. Increase quality of life NSAIDs Corticosteroids Corticosteroid Joint Injections Disease Modifying Anti-Rheumatic Drugs (MRADs) Biologic Agents
- 31. TREATMENT NSAIDs Corticosteroids Corticosteroid Joint Injections Disease Modifying Anti-Rheumatic Drugs (MRADs) Biologic Agents 1. Naproxen (Naprosyn) 2. Ibuprofen (Advil) 3. Indomethacin (Indocid) 4. Diclofenac sodium (Voltaren) 1. Prednisolone 2. Methylprednisolone 1. Triamcinolone hexacetonide 2. Triamcinolone acetonide 3. Methylprednisolone 1. Methotrexate (Rheumatrex) 2. Sulfasalazine (Salazopyrin) 3. Hydroxychloroquine (Plaquenil) 4. Leflunomide (Arava) 1. Etanercept (Enbrel) 2. Infliximab (Remicade) 3. Adalimumab (Humira) 4. Rituximab (Rituxan) 5. Abatacept (Orencia) 6. Tocilizumab (Actemra)
- 32. TREATMENT
- 33. TREATMENT 1. Physiotherapy Avoid prolonged immobilization Strengthens muscles, improves and maintain range of movement Improves balance and cardiovascular fitness 2. Ophthalmologist All patients must be referred to the ophthalmologist for uveitis screening and have regular follow-up. 3. Nutritional Therapy Calcium intake Calcium + vitamin D is advised in patients on corticosteroids Ensure appropriate protein and calorie intake
- 34. TREATMENT 4. Orthotics Management Splints and foot orthotics may be recommended 5. Thermotherapy Heat treatments Massage Cold treatment
- 35. COMPARISON
- 36. COMPARISON
- 37. REFERENCES 1. DeWitt EM, Schanberg LE, Rabiovich CE. Treatment of Rheumatic Diseases. In: Kliegman RM, Stanton BF, St Geme JW III, et al, eds. Nelson textbook of Pediatrics. 19th ed. Philadelphia: Saunders, Elsevier; 2011 1. Paediatric Protocol For Malaysia Hospitals, 3rd Edition 1. https://specialty.mims.com/rheumatology 1. http://www.aboutkidshealth.ca