
肺功能恶化:FOP的早期并发症

文献标题:Deterioration of pulmonary function: An early complication in Fibrodysplasia Ossificans Progressiva
文献作者:Esm´ee Botman a , Bernard J. Smilde a , Max Hoebink a , d Sanne Treurniet a , Pieter Raijmakers b , Otto Kamp c , Bernd P. Teunissen b , Arend B¨okenkamp , Patrick Jake , Adriaan A. Lammertsma b , Joost G. van den Aardweg e , Anco Boonstra e , Elisabeth M.W. Eekhoff a, *
a Amsterdam UMC, Vrije Universiteit Amsterdam, Department of Internal Medicine section Endocrinology, Amsterdam Movement Sciences, Amsterdam Bone Centre, de Boelelaan 1117, Amsterdam, the Netherlands
阿姆斯特丹UMC,阿姆斯特丹自由大学,内科内分泌科,阿姆斯特丹运动科学,阿姆斯特丹骨骼中心
b Amsterdam UMC, Vrije Universiteit Amsterdam, Department of Radiology and Nuclear Medicine, de Boelelaan 1117, Amsterdam, the Netherlands
阿姆斯特丹UMC,阿姆斯特丹自由大学,放射学和核医学系
c Amsterdam UMC, Vrije Universiteit Amsterdam, Department of Cardiology, de Boelelaan 1117, Amsterdam, the Netherlands
阿姆斯特丹UMC,阿姆斯特丹自由大学,心脏病学系
d Amsterdam UMC, Emma Children’s Hospital, Vrije Universiteit Amsterdam, Department of Pediatric Nephrology, de Boelelaan 1117, Amsterdam, the Netherlands
阿姆斯特丹 UMC,艾玛儿童医院,阿姆斯特丹自由大学,儿科肾脏病学系
e Amsterdam UMC, Vrije Universiteit Amsterdam, Department of Pulmonology, de Boelelaan 1117, Amsterdam, the Netherlands
阿姆斯特丹UMC,阿姆斯特丹自由大学,肺病学系
发布日期:February 25, 2021
文献下载:点击下载
ABSTRACT | 概述
进行性骨化性纤维发育不良综合征(FOP)是一种遗传性疾病,其特征表现是在软组织中形成异位骨化。早于其他边缘部位受影响之前,异位骨化最开始会在胸廓区域发展。起因于沿着胸廓的异位骨化,导致其活动能力受限,并且会造成肺功能的恶化。这是由于异位骨化是进行性的,肺功能可能会随着时间的推移而恶化,然而有关FOP肺部功能的纵向数据却是缺失的。
来自于7位FOP患者的纵向肺功能测试(PFTs)进行了回顾性的评估,用来评价肺功能随着年龄的增长是否会发生变化。这里包含了最大肺活量(FVC),每秒的用力呼气量(FEV1),总肺活量(TLC),肺残气量(RV)以及肺二氧化碳扩散容量与肺泡容量之比(DLCO/VA) 等测试数据。另外,还包含通过全身低剂量CT扫描关联PFT数据来对蔓延全胸的异位骨化量的进展鉴定。
每位患者,首次进行肺功能测试(PFT)的年龄在7-57岁之间,6-18年期间可能做过3-9次PFTs测试。通过总肺活量(TLC)或预估的最大肺活量(FVC)测试发现,除了一名患者之外,其他均有肺部功能的受限。在这些患者中,总肺活量(TLC),最大肺活量(FVC)或这两个指标,会随着年龄的增加逐年降低。除了一名患者,其他所有患者的肺残气量(RV)均有所增加。所有患者的肺二氧化碳扩散容量与肺泡容量之比(DLCO/VA) 是正常的。意想不到的是,在对患者的下颚手术松解关节后,他们每秒的用力呼气量(FEV1)有所增加。五分之四的患者胸部的异位骨化程度早在成年之前就开始发展,但并没有观察到最大肺活量(FVC)的下降。
综上所述,大多数患者在早年便会发现肺部功能的受限。我们的数据表明,肺功能的恶化与年龄有关。
Fibrodysplasia Ossificans Progressiva (FOP) is a genetic disease characterized by the formation of heterotopic ossification (HO) in connective tissues. HO first develops in the thoracic region, before more peripheral sites are affected. Due to HO along the thoracic cage, its movements are restricted and pulmonary function deteriorates. Because development of HO is progressive, it is likely that pulmonary function deteriorates over time, but longitudinal data on pulmonary function in FOP are missing.
Longitudinal pulmonary function tests (PFTs) from seven FOP patients were evaluated retrospectively to assess whether there were changes in pulmonary function during aging. Forced vital capacity (FVC), forced expiratory volume in one second (FEV1), total lung capacity (TLC), residual volume (RV) and diffusing lung capacity for carbon dioxide divided by alveolar volume (DLCO/VA) were included. In addition, HO volume along the thorax together with its progression as identified by whole body low dose CT scans were correlated to PFT data.
Per patient, aged 7–57 years at the time of the first PFT, three to nine PFTs were available over a period of 6–18 years. Restrictive pulmonary function, identified by TLC or suspected by FVC, was found in all, but one, patients. In three patients, TLC, FVC or both decreased further during the follow-up period. All, but one, patients had an increased RV. The DLCO/VA ratio was normal in all FOP patients. Interestingly, FEV1 increased after a surgical intervention to unlock the jaw. In four out of five patients total HO volume in the thoracic region progressed beyond early adulthood, but no further decline in FVC was observed.
In conclusion, restrictive pulmonary function was found in the majority of patients already at an early age. Our data suggest that the deterioration in pulmonary function is age dependent.
1 Introduction | 简介
进行性骨化性纤维发育不良(FOP)是一种罕见的致残性遗传疾病,其特征表现是在肌肉、韧带和肌腱中形成异位骨化。形成异位骨化之前通常会出现急性发作,这是一个炎症发展的过程,目前从病理生理学角度原因不明。大多数情况下,首次发作会在6岁左右,通常会涉及颈部和上背部。胸部异位骨化将导致胸廓固定,限制肺部的正常扩张,由于横膈膜不会受到FOP的影响,因此患者只能依赖横膈膜运动进行呼吸。FOP患者的平均预期寿命在40-50岁左右,心肺综合征是死亡的主要原因。一些横向研究表明,FOP患者的肺功能受限,归因于胸部活动能力的受限。然而,目前尚不清楚在疾病的发展过程中,肺部功能是否会进一步的下降。肺功能的纵向检查(PFT)可以更深入地了解异位骨化的规模以及其发展对肺部功能的影响。
据我们所了解,FOP患者肺功能的纵向数据从未有过研究。这里我们会推定,假设存在肺功能下降与胸腔周围的异位骨化发展的确有关。因此,本想研究的目的是评估PFT随着时间的变化与胸部异位骨化体积变化之间的关系。
Fibrodysplasia Ossificans Progressiva (FOP) is a rare, disabling genetic disease, which is characterized by the formation of heterotopic ossification (HO) in muscles, ligaments and tendons (Kaplan and Smith, 1997; Cohen et al., 1993). HO often is preceded by a flare-up, an inflammatory process with, as yet, unknown pathophysiology. In most cases the first flare-ups occur around the age of six, often involving neck and upper back (Pignolo et al., 2016). Thoracic HO immobilizes the thoracic cage, restricting normal expansion of the lungs (Kaplan et al., 2010; Kaplan and Glaser, 2005; Kussmaul et al., 1998; Connor et al., 1981). As a result, patients are dependent on diaphragmatic breathing as the diaphragm is spared in FOP (Connor et al., 1981). Mean life expectancy of patients with FOP is limited to 40–50 years of age, with cardiorespiratory complications as the major cause of death (Kaplan et al., 2010; Kaplan and Glaser, 2005). Some cross-sectional studies have shown restricted pulmonary function in FOP, which was attributed to limited chest mobility (Kussmaul et al., 1998; Connor et al., 1981; Buhain et al., 1974). It is not known, however, whether pulmonary function declines further while the disease is progressing. Longitudinal pulmonary function tests (PFTs) could give more insight on the impact of both HO volume and its progression on pulmonary function (Botman et al., 2019).
To the best of our knowledge, longitudinal data on pulmonary function in FOP patients have not been studied yet. It can be hypothesized that a decline in pulmonary function, if present, is related to (chronic) progression of HO around the thoracic cage. The aim of this study was therefore to assess the relationship between temporal changes in PFTs and volumetric HO changes along the thoracic area.
2 Methods | 方法
省略。。。。
3 Results | 结果
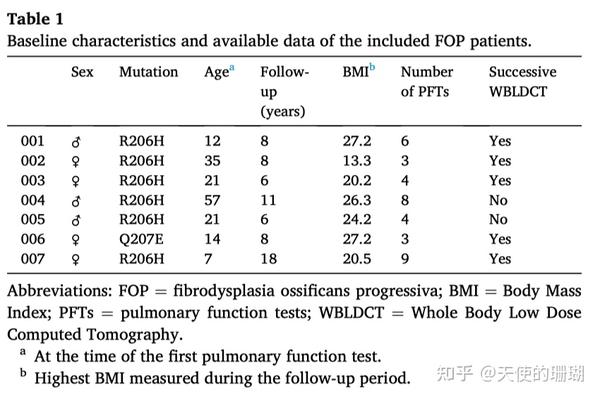
本项研究包含7名FOP患者的纵向肺功能测试(PFTs)。除了一名患者外,所有患者均有典型的(R206H)突变(表1)。变异FOP患者(Q207E)与具有典型突变的患者,在表型上没有差异。所有患者均表现出典型的FOP临床特征,并伴有进行性的异位骨化形成。在急性发作期间,全部患者均接受过皮质类固醇激素和非激素类抗炎药的标准治疗。令人遗憾的是这些患者多年来的急性发作和药物治疗并没有被纪录下来。其中一名患者(患者004)是一名吸烟者,发作期间前后保持着每年5包以上的吸烟量。
总共有37个肺功能测试(PFT)纳入了本次分析。在这些肺功能测试中,12例患者是在儿童时期(小于18岁)患病的。在6至18年期间,每位患者大概做过3-9次肺功能测试。首次进行肺功能测试的年龄范围在7至57岁之间(表1)。61%的肺功能测试是在阿姆斯特丹UMC进行的。有两名患者是在其他中心进行的肺功能测试。
在对五名患者的观察期间,至少会有两次全身低剂量螺旋CT扫描(WBLDCT)用于将胸部异位骨化与肺部功能建立关联。
对与所有37次的肺功能测试(PFT),每秒的用力呼气量(FEV1)和最大肺活量(FVC)的结果均是可用的,而总肺活量(TLC)则是37次肺功能测试(PFT)中进行了20次测量(来自6名患者)。另外对6名患者的37次肺功能测试(PFT)进行了15次的二氧化碳扩散容量测试。
Longitudinal PFTs of seven FOP patients were included in the study. All patients, except one, had the classic mutation (R206H) (Table 1). The patient with the variant Q207E did not differ phenotypically from those with the classic mutation. All patients exhibited the classical clinical features of FOP with progressive HO formation. During flare-ups all patients underwent standard therapy with corticosteroids and nonsteroidal anti-inflammatory drugs. Unfortunately, the frequency of flare-ups and drug treatments over the years had not been recorded. One patient (patient 004) is a smoker, with 5 pack years up to the end of the included period.
In total, 37 PFTs were included in the analysis. Of these PFTs, 12 were obtained in childhood (<18 years of age). Per patient, three to nine PFTs were available over a period of six to eighteen years. The age at which the first pulmonary function was obtained ranged from 7 to 57 years (Table 1). 61% of all the PFTs were obtained at Amsterdam UMC. In two patients, tests were performed in other centers.
In five patients at least two WBLDCT scans were available during the observation period to relate HO progression in the thoracic region with pulmonary function.
For all 37 PFTs, FEV1 and FVC were available, while TLC was only measured in 20 of the 37 PFTs (from 6 patients). Diffusion capacity was measured in 15 of the 37 PFTs from six patients.
3.1. Spirometry (FVC, VC, FEV1) | 肺活量测定法(FVC, VC, FEV1)
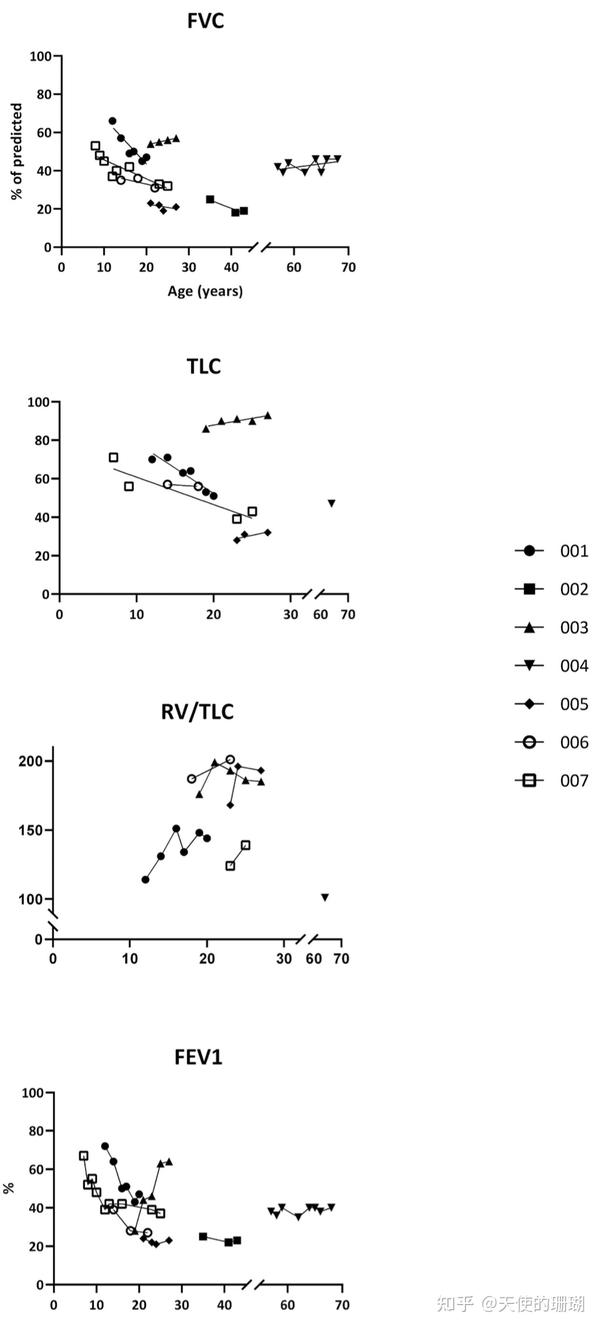
在全部患者中,无论年龄大小与否,最大肺活量(FVC)均低于预测值的80%,在一名最年轻的患者(7岁)接受测试中,最大肺活量(FVC)已经低于80%。在7名FOP患者中,有3名患者的最大肺活量(FVC)随着时间的推移而恶化,在他们的儿童时期便已经开始下降(图1)。其中两名患者,病情的恶化一直持续到23岁的青年时期。另外两名患者也在20岁左右接受了随访,在观察期间,最大肺活量(FVC)没有变化。对与本项研究中年龄最大的两名患者,分别是从57岁到68岁和35岁至43岁期间进行的随访,最大肺活量(FVC)预测值的绝对值和百分比均保持稳定。在整个随访期间,所有患者的肺活量与最大肺活量(FVC)一致。
每秒的用力呼气量(FEV1)与最大肺活量(FVC)之比,也被成为Tiffeneau指数,在两名18岁和68岁的患者中这个指标低于70%(Tiffeneau分别为68%和65%)。相对于所有其他患者,Tiffeneau指标大于70%,排除了任何阻塞的可能。令人意外的是,一名接受颌骨手术的患者,在术后Tiffeneau指标从70%上升到95%。Tiffeneau指标的增加是由于每秒的用力呼气量(FEV1)增加(从原来46%增加到64%),这可能与张口的轻微改善(3毫米)有关(补充数据,图1)。手术前和术后的最大肺活量FVC和肺活量VC一直保持稳定。此外,肺残气量(RV)也没有因为张口改善而改变。这里的5名有颌骨强直的患者和2名无颌骨强直的患者的Tiffeneau指标并无明显差别(分别是65-93%和91-94%)。
注:当 FEV1 除以肺活量(在单独的、非强制的测量中测量)时,就会得到 Tiffeneau 指数。 该指数的正常值约为 0.75。 低于 0.70 存在阻塞性肺功能。
FVC was below 80% of predicted in all patients irrespective of age and was already <80% in the youngest patient tested at the age of seven. FVC deteriorated over time in three of the seven FOP patients with a decline already in childhood.(Fig. 1). In two of these patients, worsening continued into young adulthood, up to the age of twenty-three. For two other patients, also followed in their twenties, FVC did not increase or decline during observation. For the oldest two patients in this study, followed from the age of 57 to 68 years and 35 to 43 years, respectively, both absolute and percentage of predicted values for FVC remained stable. VC was congruent with FVC for all patients throughout the follow-up period.
FEV1/FVC, also known as the Tiffeneau index, was below 70% of predicted in two patients, aged 18 and 68 years old (Tiffeneau of 68% and 65%, respectively). For all other patients the Tiffeneau index was >70%, ruling out any obstructive component. Interestingly, one patient who underwent jaw surgery experienced an increase in the Tiffeneau index from 70% to 95% following surgery. The increased Tiffeneau index resulted from an increase in FEV1 (from 46% to 64%), possibly related to the slight improvement (3 mm) of mouth opening (supplemental data, Fig. 1). FVC and VC remained stable pre- and postoperatively. In addition, also RV did not change due to the increased mouth opening. The Tiffeneau index in five patients with and two patients without jaw ankyloses showed no obvious difference (65–93% vs 91–94%, respectively).
3.2. Static lung volumes (TLC, RV, ERV) | 静态肺容量 (TLC, RV, ERV)
这里有6名患者的总肺活量(TLC)的随访数据可用。对与每位患者而言,只有一项测量结果可用。6位患者中有5位出现较低的总肺活量(TLC),这表明肺部功能受限(低于预估值的80%)。一名患者的最大肺活量和肺活量较低,但总肺活量似乎正常(图1)。
我们在两名患者的儿童时期和青春期早期观察到了总肺活量(TLC)的恶化。一名患者的总肺活量(TLC)在19岁之前开始下降,另一名患者在9至23岁之间开始下降。23岁以后,总肺活量(TLC)就没有了变化,但这里要注意的是,这仅是基于两名患者的数据,他们在总肺活量(TLC)稳定后随访了2年。对与两名年纪较大的患者,并没有总肺活量(TLC)的随访数据。
这6名患者中有5名患者的肺残气量(RV)与总肺活量(TLC)的比率增加(图1)。这一比率在预估值的125%~200%之间。术后张口的增加并未导致肺残气量(RV)的正常。然而,手术的确改善了补呼气量(ERV)。手术前,该患者的补呼气量(ERV)为0.86L,手术后增加到1.16L。相对于其他患者,他们的ERV却介于0.74L和0.1L之间。
TLC follow-up data were available for six patients. For one patient, only one measurement was available. A low TLC, indicating restrictive lung function (below 80% of predicted) was observed in five of the six patients. One patient with a low FVC and VC, appeared to have a normal TLC (Fig. 1).
Deterioration of TLC during the observation period was observed in two patients during childhood and early adolescence. TLC in one patient decreased until the age of 19 and in the other patient between the age of 9 and 23. After the age of 23, no decline in TLC was found, but it should be noted that this is based on data of only two patients who were followed for up to 2 years after stabilization of TLC. For the two oldest patients, TLC follow-up data were not available.
The RV to TLC ratio was increased in five of the six patients (Fig. 1). The ratio ranged from 125 to 200% of predicted. The increase in mouth opening after surgery, did not result in normalization of RV. However, it did result in an increased volume of air that could be exhaled forcibly (ERV). Prior to surgery the ERV for this particular patient was 0.86 L, which increased to 1.16 L after surgery. For all other patients ERV ranged between 0.74 L and 0.1 L.
3.3. Diffusing capacity (DLCO and DLCO/VA) | 肺弥散量 (DLCO and DLCO/VA)
有6名患者的肺一氧化碳弥散量(DLCO)可用,其中5名患者的预估值在40%到60%之间。接受口腔-上颌手术的患者,在术后肺一氧化碳弥散量(DLCO)没有增加。此外,在患有和未患有颌骨强直(前者占三分之二,后者占三分之一)的患者之间,肺一氧化碳弥散量(DLCO)没有发现统计学上的差异(Mann-Whitney U:p=0.64)。当肺一氧化碳弥散量(DLCO)校正了肺泡容积(DLCO/VA)时,全部6名患者的扩散率均大于80%。
DLCO was available for six patients and between 40 and 60% of predicted in five patients. The patient who underwent oro-maxillary surgery showed an no increase in DLCO after surgery. Also, no statistical difference in DLCO was found between patients with (four out of six patients) and without jaw ankyloses (two out of six patients) (Mann Whitney U: p = 0.64). When DLCO was corrected for alveolar volume (DLCO/VA), diffusion was >80% for all six patients.
3.4. Lung parenchyma | 肺实质
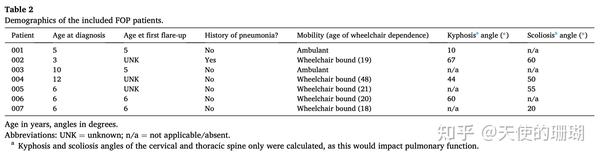
我们用低剂量CT扫描对全部7名患者进行了肺实质评估。其中五名患者的胸腔高度变形,而另外两名患者的胸腔几乎正常。脊柱前凸和脊柱侧凸的存在和严重程度可以见表2.这两名患者分别为20岁和24岁。两人的肺实质正常,没有发现胸膜增厚或心脏重大。5名胸部急性的患者中有3名患者出现了肺内异常:一名患者左肺下叶部分不张大约330毫升,占总肺容积的4%。其中一位患者在22岁时出现过肺部轻度毛玻璃浑浊。实质和胸膜未见异常。一名65岁的患者有轻微的实变(3mm),根据Fleishner标准,目前正在进行高分辨率的CT检查。
Low-dose CT scans to evaluate lung parenchyma were available for all seven patients. Five showed a highly deformed thoracic cage, while it was nearly normal in the other two patients. The presence and severity of kyphosis and scoliosis are presented in Table 2. These two patients were 20 and 24 years old. Both had normal lung parenchyma, no pleural thickening or cardiomegaly. Three of the five patients with a deformed thorax showed intrapulmonary abnormalities: one had a partial atelectasis of the lower left lobe of ≈330 mL, occupying 4% of the total lung volume. One had mild ground-glass opacity at the age of 22. There were no abnormalities in the parenchyma or pleurae. One patient, aged 65, had a minimal consolidation (3 mm), which is currently being followed by high resolution CT according to the Fleishner criteria (MacMahon et al., 2017).
3.5. Heterotopic ossification | 异位骨化
有5名患者的连续6-26个月的低剂量全身CT(LDWBCT)扫描数据可用。患者全身的异位骨化量、胸部异位骨化量和胸背部的异位骨化量均与肺功能测试(PFT)参数无明显相关性(补充数据)。在4名患者中观察到了胸部的异位骨化进展,在6-26个月内的范围是5至11ml。在6个月内胸部区域的异位骨化增加了11ml,最明显的进展过程中伴随着稳定的总肺活量(TLC)、最大肺活量(FVC)和肺一氧化碳弥散量DLCO/肺活量VA(图1)。这包括所有5名连续进行CT扫描的患者在内,在这段时间不长的观察期内,未发现异位骨化的扩张和FVC之间的变化存在关联(spearman's rho=− 0.2; p=0.7)。至此,未发现总异位骨化量、胸部异位骨化量与肺功能测试(PFT)参数之间存在关联(补充数据)。
In five patients successive LDWBCT-scans over a period of 6–26 months were available. Neither total body HO volume, HO volume within the thoracic area, nor HO volume along the thoracic back were significantly correlated with any of the PFT parameters (supplemental data). HO progression in the thoracic area was seen in four patients and ranged from 5 to 11 mL in 6 to 26 months. The most prominent progression in the thoracic area with an increase in HO of 11 mL in 6 months was accompanied by stable TLC, FVC and DLCO/VA (Fig. 1). Including all five patients for whom successive CT scans were available, no association was found between HO expansion and FVC changes over this short period of time (spearman’s rho = − 0.2; p = 0.7). In addition, no association was found between total HO volume, thoracic HO volume and the PFT parameters (supplemental data).
4. Discussion | 讨论
在对7名FOP患者的纵向数据中分析了37次肺功能测试(PFT),以确定这6-18年期间的肺功能是否与胸部异位骨化量和异位骨化的进展有关。除了1名患者外,所有患者均出现了肺功能受限。这种肺功能受限在儿童时期和青春期早期会随着时间的推移而恶化,但在日后的生活中并没有观察到进一步的下降。未发现明显的肺功能阻塞,也未发现肺功能的损害程度与胸部异位骨化量之间的关系。
每秒的用力呼气量(FEV1)是快速评估肺功能的最简单指标。每秒的用力呼气量(FEV1)的值降低通常与肺功能阻塞的程度相关。在当前数据中,所有的患者每秒的用力呼气量(FEV1)值明显下降,但Tiffeneau指标正常。因此,每秒的用力呼气量(FEV1)的下降可以归因于FOP患者的肺容量减少。在FOP中常见的颌骨强直会直接影响每秒的用力呼气量(FEV1)数值,其中上颌骨固定会导致每秒的用力呼气量(FEV1)下降约20%。此外,一项使用不同直径开口的口片用于模拟上呼吸道阻塞的影响的研究发现,每秒的用力呼气量(FEV1)随着直径的见效而逐渐恶化。因此,尽管目前大多数FOP患者的每秒的用力呼气量(FEV1)因肺容量下降而降低,但是颌骨阻滞也可能在每秒的用力呼气量(FEV1)的恶化中发挥着作用。
所有患者的最大肺活量(FVC)与肺活量均会下降,这表明存在肺功能受限。然而,需要注意的是,最初为了能够确定肺功能受限,评估总肺容积量(TLC)至关重要,因此需要使用额外的测试。在目前的研究中,尽管是依据最大肺活量(FVC)的标志性受限(57%)指标,但也仅仅在一名患者中观察到正常的总肺容积量(TLC)。这可能是因为除了这名患者以外,其他所有患者的肺残气量(RV)都有所增加,这也代表了总肺容量(TLC)和肺活量(VC)之间的差异。FOP患者的肺残气量(RV)增加的潜在机制可能是无法完全呼气,这可能是由于胸腔完全僵硬造成的,肺残气量(RV)升高也被视为神经性肌肉疾病的早期肺部异常。在后期,肌肉无力也会导致肺部功能受限。这一过程是否也会发生在FOP患者中,依据目前有限的数据尚无法证实。值得注意的是,65岁的患者的肺残气量(RV)是在正常的范围内。随着年龄的增长,肺残气量(RV)被认为是胸壁硬化的结果。FOP患者不会发生这种硬化,因为他们的胸壁已经完全被异位骨化包裹受限,这解释了当前患者数据,在这个观察期间肺残气量(RV)增加,但却很稳定的原因。由于肺残气量(RV)似乎不会随着时间而波动,在总肺容积量(TLC)初步确认受限后,最大肺活量(FVC)可用于检测肺部的功能。
正如本次研究所观察到的,肺功能限制与两项横向研究的结果一致(Kussmaul等人,1998年;Connor等人,1981年)。这两项研究分别包括21名和15名FOP患者。但不巧的是,期间并没有获得总肺容积量(TLC)的数值。尽管Kussmaul等人所研究的患者年龄在5-55岁之间,但也仅仅只给出了整个实验组的数值,因此无法比较年轻患者和老年患者的肺功能情况。另外一方面,在对成年FOP患者的研究中,Connor等人得出了结论,年龄对受限程度并没有影响,因为最大肺活量(FVC)在不同的年龄组之间并没有差异。目前尚不确定这种恶化是否会真的发生,如果发生,会是在什么年龄发生。我们只能在相对较短的时间内跟踪3名从童年到青春期的患者。这需要更长的随访时间和更多的结构性肺功能测试(PFT)数据来确认肺功能是否会在特定的年龄中稳定下来。假设肺功能限制是由于肋椎关节畸形和胸壁畸形所致(因脊柱和胸腔内的不对称异位骨化而导致的结果)。有人可能会认为胸壁畸形(脊柱后凸或侧凸)的严重程度会影响胸腔的受限,从而影响肺功能。然而,其中两名胸部急性相对矫情的患者也的确出现了严重的肺功能受限。因此,仅仅胸部畸形不能完全预测肺部功能的异常。此外,异位骨化的位置,异位骨化量,尤其是异位骨化是否存在于关键的关节附近,这也可能非常重要。此外,在生命的后期,肺功能几乎不会恶化。
我们需要终身的肺功能测试(PFT)数据和WBLDCT图像来评估与轻度异常的肺实质之间的临床相关性,因为在本次研究中的2名患者身上均有发现。肺功能受限可能会导致肺部松弛不张,从而降低TLC。在当前的研究中,并没有区分由固化的胸腔或肺不张所引起的受限。在其中一名患者中所观察到的肺不张仅占总TLC的一小部分,因此,胸部僵硬可能是FOP患者的肺功能受限的最重要的原因。为了预防肺不张,可以考虑使用带导管的手持装置和含有连接器的呼吸袋进行呼吸机训练,以便维持肺泡的充分同期。此外,如果考虑进行氧疗,应该密切地检测患者,以防止高碳酸血症和高氧对起到或肺实质的损害,尤其注意的是,一般情况下患者的严重受累、胸腔固定已经具有了一定程度的高碳酸血症。
本研究的优势是对一组FOP患者进行了长期的随访。本研究的主要局限性在于,因相关文档的不完整,无法将肺功能测试与临床数据进行关联。此外,由于数据是在标准患者护理的背景下获得的,因此没有定期获得肺功能测试(PFT),也没有获得所有相关数据。还有就是,随着时间的推移或者不同中心之间的测量设备并没有进行标准化。在长期的跟踪随访期间,使用了各种测量仪器,这也包含了其他中心的一些数据,这些中心的测量仪器的情况也无从确认。
总之,通过纵向的肺功能测试(PFT)证实了FOP患者在年轻时就已经出现了肺功能受限。总肺容量(TLC)对与确认FOP患者最初的受限情况是必要的,因为肺残气量(RV)的增加可能会影响最大肺活量(FVC)。此外,要注意的是,由于肺体积小,每秒的用力呼气量(FEV1)的值下降,这也可能是收到了颌骨强直的影响。但无论是异位骨化总量还是进行性的异位骨化发展似乎都不会影响生命后期的费功能。诚然,这也很明显,我们需要更长的随访时间来证明这一发现。



Thirty-seven PFTs were analyzed in a longitudinal cohort of seven FOP patients to determine whether lung function over a period of 6 to 18 years was associated with HO volume and HO progression in the thoracic area. A restrictive pulmonary function was found in all but one patients. This restriction in pulmonary function deteriorated over time during childhood and early adolescence, but a further decline later in life was not observed. No significant obstructive pulmonary function was found, nor a relationship between the degree of pulmonary function impairment and thoracic HO volume.
FEV1 is the simplest parameter to obtain a rapid assessment of lung function. A reduced FEV1 value usually is related to the degree of obstructive pulmonary function (Pellegrino et al., 2005; Brazzale et al., 2016). In the current cohort, significantly reduced FEV1 values were found in all patients, but in the presence of a normal Tiffeneau index. The reduced FEV1 value can therefore be attributed to reduced lung volumes in FOP patients. An ankylosed jaw, often seen in FOP, affects FEV1 values. In one the present patients, FEV1 increased by 40% after surgical unlocking the ankylosed jaw. A similar effect on FEV1 was found in possibly the only published study on this topic, assessing the effect of maxillomandibular fixation in healthy subjects on pulmonary function, where FEV1 decreased with approximately 20% as a result of the maxillomandibular fixation (Kohno et al., 1993). In addition, a study simulating the effect of upper airway obstruction using mouth pieces with orifices of different diameters, found that FEV1 progressively worsened with decreasing diameters (Empey, 1972). Therefore, although FEV1 was decreased in most of the present FOP patients due to decreased lung capacity, jaw occlusion also may play a role in the severity of FEV1.
All patients had reduced FVC and VC, which suggests the presence of restrictive lung function. It should be noted, however, that to confirm restrictive pulmonary function initially, assessment of total lung volume (TLC) is essential, and therefore the use of an additional test is required (Pellegrino et al., 2005). In the present study, a normal TLC was only observed in one patient, despite a suggestive restriction based on FVC (57%). This may be explained by an increased RV, seen in all but one of the patients, and which represents the difference between TLC and VC. The underlying mechanism of an increased RV in FOP patients could be the inability to fully exhale, possibly due to completely ankyloses of the thoracic cage. An increased RV is also seen as an early pulmonary abnormality in neuromuscular diseases (Chiang et al., 2018). In later stages, muscle weakness leads to a restrictive pulmonary function. Whether this process also occurs in FOP patients, could not be confirmed with the current limited dataset. Remarkably, RV in the 65-year old patient was within the normal range. With aging, RV is thought to increase as a result of stiffening of the thoracic wall (Sharma and Goodwin, 2006). FOP patients will not be susceptible for this stiffening as they are already completely ankylosed, explaining the increased, but stable, RV throughout the observed period in the current cohort. As RV does not seem to fluctuate over time, FVC can be used to monitor pulmonary function after initial confirmation of restriction by TLC.
The restrictive pulmonary function, as seen in the present study, is in concordance with findings of two cross-sectional studies (Kussmaul et al., 1998; Connor et al., 1981). These two studies included 21 and 15 FOP patients, respectively. Unfortunately TLC values were not obtained. Although the age of the patients studied by Kussmaul et al. ranged from 5 to 55 years, values were only presented for the entire group, making it impossible to compare pulmonary function of younger patients with that of older patients (Kussmaul et al., 1998). On the other hand, On the other hand, in their study on adult FOP patients, Connor et al. concluded that age had no effect on the degree of restriction, as FVC did not differ between age groups (Connor et al., 1981). It remains uncertain whether such a plateau of deterioration does indeed occur and if so, at what age. We could only follow three patients from childhood to adolescence during a relatively short period. Longer follow-up and more structural PFTs are needed to confirm whether pulmonary function indeed stabilizes at a certain age. It is assumed that the restrictive pulmonary function is the result of both malformed costovertebral joints and chest wall deformities due to asymmetrical HO formation along the spine and thoracic cage (Kaplan et al., 2010). One could argue that the severity of the chest wall deformity (kyphosis or scoliosis) should have an impact on the restriction of the thoracic cage and therefore pulmonary function (Daghighi and Tropp, 2019; Farrell and Garrido, 2020). Two of the patients with relatively mild thoracic deformities did, however, show severe restricted pulmonary function. Therefore, thoracic deformity alone does not fully predict abnormality of lung function. In addition, the location of HO, especially whether HO is located near crucial joints or not, might also be important. Also, pulmonary function hardly appears to deteriorate later in life, it seems that the amount of HO formed in the thoracic area at younger age may already be sufficient to restrict pulmonary function and that it is not affected by further (later) progression of HO. In an attempt to further investigate this, effects of total amount and chronic growth of HO in the thoracic region and pulmonary function were assessed, but neither showed a relationship with the pulmonary function nor its decline. Moreover, previously it has been shown that chest wall expansion does not deteriorate further after the age of 15 (Kussmaul et al., 1998). However, lifetime PFT data from FOP patients are not available yet.
Life-long PFT data and WBLDCT images will be needed to evaluate the clinical relevance of mild abnormalities of the lung parenchyma, which were seen in two of the patients in the present study. Restrictive pulmonary function may lead to relaxation atelectasis, which may reduce TLC. In the present study no distinction was made between restriction caused by an immobile thorax or by atelectasis. Atelectasis observed in one of the patients covered only a small portion of total TLC and, therefore, thoracic stiffness is likely to be the most important cause of restrictive pulmonary function in FOP. In an attempt to prevent atelectasis, respiratory muscle training, using a hand-held unit with tubing and a connected rebreathing bag, could be considered in an attempt to maintain adequate ventilation of the alveoli (Budweiser et al., 2006). In addition, if oxygen therapy is considered, the patient should be monitored closely to prevent hypercapnia and hyperoxia related damage to airways or pulmonary parenchyma (Kaplan and Glaser, 2005), especially as, in general, patients with a severely affected, immobilized thoracic cage already have a degree of hypercapnia (Bergofsky, 1979).
The strength of this study is the long follow-up period of a group of FOP patients. The main limitation of the present study is the inability to relate pulmonary function tests to clinical data, due to incomplete documentation. Also, given that data were acquired within the context of standard patient care, PFTs had not been obtained regularly and not all parameters were obtained. In addition, measuring equipment was not standardized over time or between different centres. Throughout time various measuring instruments have been used, and, data of other centers are included of which the measuring instruments are unknown.
In conclusion, longitudinal PFTs confirmed restricted pulmonary function in FOP patients already at young age. TLC is necessary to confirm the restrictive component in FOP patients initially, as increased RV may affect FVC. In addition, it should be noted that FEV1 values are diminished due to small lung volumes, but might also be affected the jaw ankylosis. Neither total volume of HO nor progression of thoracic HO seemed to affect pulmonary function later in life. It will be clear, however, that longer follow-up periods are needed to confirm this finding.
多多爸( 微信: Aspirinic)
”天使的珊瑚FOP关爱之家“ 微信群主:
明明:微信号: gogoniluyo
方方:微信号: lengmou1314520
多多爸: 微信号: Aspirinic
微信群/公众号搜索:天使的珊瑚FOP关爱之家
注:为避免入错群,请家长/患者入群前,准备好ACVR1的基因检测报告。
参考文献:
Bergofsky, E.H., 1979. Respiratory failure in disorders of the thoracic cage. Am. Rev. Respir. Dis. 119 (4), 643–669.
胸腔疾病中的呼吸衰竭
Botman, E., Raijmakers, P., Yaqub, M., Teunissen, B., Netelenbos, C., Lubbers, W., Schwarte, L.A., Micha, D., Bravenboer, N., Schoenmaker, T., de Vries, T.J., Pals, G., Smit, J.M., Koolwijk, P., Trotter, D.G., Lammertsma, A.A., Eekhoff, E.M.W., 2019. Evolution of heterotopic bone in fibrodysplasia ossificans progressiva: an [(18)F]NaF PET/CT study. Bone 124, 1–6.
FOP异位骨的演变:一项[(18)F]NaF PET/CT研究
Brazzale, D., Hall, G., Swanney, M.P., 2016. Reference values for spirometry and their use in test interpretation: a position statement from the Australian and New Zealand Society of Respiratory Science. Respirology 21 (7), 1201–1209.
肺活量测定的参考值及其在测试解释中的应用:澳大利亚和新西兰呼吸科学学会的立场声明
Budweiser, S., Moertl, M., Jorres, R.A., Windisch, W., Heinemann, F., Pfeifer, M., 2006.
Respiratory muscle training in restrictive thoracic disease: a randomized controlled trial. Arch. Phys. Med. Rehabil. 87 (12), 1559–1565.
限制性胸部疾病的呼吸肌训练:一项随机对照试验
Buhain, W.J., Rammohan, G., Berger, H.W., 1974. Pulmonary function in myositis ossificans progressiva. Am. Rev. Respir. Dis. 110 (3), 333–337.
进行性骨化性肌炎的肺功能
Chiang, J., Mehta, K., Amin, R., 2018. Respiratory diagnostic tools in neuromuscular disease. Children (Basel) 5 (6).
神经肌肉疾病的呼吸诊断工具
Cobb, J., Cobb, J.R., 1948. Outlines for the study of scoliosis, journal of bone and joint surgery. American Volume 5, 261–275.
脊柱侧凸的研究综述,《骨与关节外科杂志》
Cohen, R.B., Hahn, G.V., Tabas, J.A., Peeper, J., Levitz, C.L., Sando, A., Sando, N., Zasloff, M., Kaplan, F.S., 1993. The natural history of heterotopic ossification in patients who have fibrodysplasia ossificans progressiva. A study of forty-four patients. J Bone Joint Surg Am 75 (2), 215–219.
FOP患者异位骨化的自然病史
Connor, J.M., Evans, C.C., Evans, D.A., 1981. Cardiopulmonary function in fibrodysplasia ossificans progressiva. Thorax 36 (6), 419–423.
FOP的心肺功能
Daghighi, A., Tropp, H., 2019. Computed tomography lung volume estimation and its relation to lung capacities and spine deformation. J Spine Surg 5 (1), 132–141.
CT肺容积估计及其与肺容量和脊柱变形的关系
Empey, D.W., 1972. Assessment of upper airways obstruction. Br. Med. J. 3 (5825), 503–505.
上呼吸道阻塞的评估
Farrell, J., Garrido, E., 2020. Predicting preoperative pulmonary function in patients with thoracic adolescent idiopathic scoliosis from spinal and thoracic radiographic parameters. Eur. Spine J.
根据青少年胸部特发性脊柱侧弯和影响学数据来预测患者术前的肺部功能。
Kaplan, F.S., Glaser, D.L., 2005. Thoracic insufficiency syndrome in patients with fibrodysplasia ossificans progressiva. Clinical Reviews in Bone and Mineral Metabolism 3 (3), 213–216.
FOP患者的胸廓功能不全综合征
Kaplan, F.S., Smith, R.M., 1997. Fibrodysplasia ossificans progressiva (FOP). J. Bone Miner. Res. 12 (5), 855.
进行性骨化性纤维发育不良(FOP)
Kaplan, F.S., Zasloff, M.A., Kitterman, J.A., Shore, E.M., Hong, C.C., Rocke, D.M., 2010. Early mortality and cardiorespiratory failure in patients with fibrodysplasia ossificans progressiva. J. Bone Joint Surg. Am. 92 (3), 686–691.
FOP患者的早期死亡率和心肺功能衰竭
Kohno, M., Nakajima, T., Someya, G., 1993. Effects of maxillomandibular fixation on respiration. Journal of Oral and Maxillofacial Surgery : Official Journal of the American Association of Oral and Maxillofacial Surgeons 51 (9), 992–996.
上颌骨固定对呼吸的影响
Kussmaul, W.G., Esmail, A.N., Sagar, Y., Ross, J., Gregory, S., Kaplan, F.S., 1998. Pulmonary and cardiac function in advanced fibrodysplasia ossificans progressiva. Clinical Orthopaedics and Related Research (346), 104–109.
晚期FOP患者的肺和心功能
MacMahon, H., Naidich, D.P., Goo, J.M., Lee, K.S., Leung, A.N.C., Mayo, J.R., Mehta, A. C., Ohno, Y., Powell, C.A., Prokop, M., Rubin, G.D., Schaefer-Prokop, C.M., Travis, W.D., Van Schil, P.E., Bankier, A.A., 2017. Guidelines for management of incidental pulmonary nodules detected on CT images: from the Fleischner Society 2017. Radiology 284 (1), 228–243.
CT图像上偶然发现的肺结节的处理指南:来自弗莱什纳学会2017年
Pellegrino, R., Viegi, G., Brusasco, V., Crapo, R.O., Burgos, F., Casaburi, R., Coates, A., van der Grinten, C.P., Gustafsson, P., Hankinson, J., Jensen, R., Johnson, D.C., MacIntyre, N., McKay, R., Miller, M.R., Navajas, D., Pedersen, O.F., Wanger, J., 2005. Interpretative strategies for lung function tests. Eur. Respir. J. 26 (5), 948–968.
肺功能测试的解释策略
Pignolo, R.J., Bedford-Gay, C., Liljesthrom, M., Durbin-Johnson, B.P., Shore, E.M., Rocke, D.M., Kaplan, F.S., 2016. The natural history of flare-ups in fibrodysplasia ossificans progressiva (FOP): a comprehensive global assessment. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research 31 (3), 650–656.
进行性骨化性纤维发育不良(FOP)发病的自然史:一项全面的全球评估
Quanjer, P.H., Stanojevic, S., Cole, T.J., Baur, X., Hall, G.L., Culver, B.H., Enright, P.L., Hankinson, J.L., Ip, M.S., Zheng, J., Stocks, J., 2012. E.R.S.G.L.F. Initiative, Multiethnic reference values for spirometry for the 3–95-yr age range: the global lung function 2012 equations. Eur Respir J 40 (6), 1324–1343.
倡议,3-95岁年龄段肺活量测定的多民族参考值:2012年全球肺功能方程式
Sharma, G., Goodwin, J., 2006. Effect of aging on respiratory system physiology and immunology. Clin. Interv. Aging 1 (3), 253–260.
衰老对呼吸系统生理和免疫学的影响
Stanojevic, S., Graham, B.L., Cooper, B.G., Thompson, B.R., Carter, K.W., Francis, R.W., Hall, G.L., 2017. T.w.g. global lung function initiative, T. global lung function initiative, official ERS technical standards: global lung function initiative reference values for the carbon monoxide transfer factor for Caucasians. Eur. Respir. J. 50 (3).
全球肺功能倡议,官方ERS技术标准:全球肺功能倡议高加索人一氧化碳转移因子参考值
