pneumonectomy
(redirected from pneumonectomies)Also found in: Dictionary, Thesaurus, Encyclopedia.
pneumonectomy
[noo″mo-nek´to-me]excision of lung tissue, of an entire lung (total pneumonectomy) or less (partial pneumonectomy), or of a single lobe (lobectomy).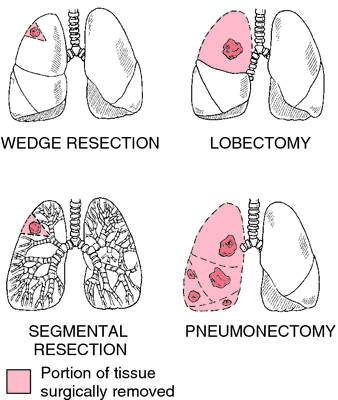
Patient Care. Pneumonectomy is most often done as a treatment for lung cancer; it is also done with less common diseases such as extensive unilateral tuberculosis, bronchiectasis, and multiple abscesses of the lung. Thus patients who have a pneumonectomy are likely to have suffered some chronic and debilitating illness prior to surgery and will have special needs to avoid complications and promote healing and recovery.
After surgical removal of a lung, the chest is closed and there is no closed drainage of the thoracic cavity. Instead, pressure within the pleural space is adjusted by using a simple thoracentesis and manometer, which help maintain the mediastinum midline. Fluid and air are allowed to accumulate in the space left by the excised lung to prevent shift of the mediastinum to the operative side. A second reason for not inserting a chest tube and drainage is the danger of contamination and possible empyema.
The patient is not allowed to lie on the operative side. If the operative lung is permitted to be dependent, fluid can enter the space, causing tension pneumothorax secondary to mediastinal shift; should the bronchial stump rupture, drowning in the accumulated fluid could occur.
Fluid balance is watched closely by pressure monitoring to avoid overhydrating the patient. A central venous line or Swan-Ganz catheter may be used to guide fluid replacement. Serial blood gases and chest x-rays are done to detect early signs of respiratory complications. Additionally, blood tests are done and electrolyte levels are evaluated to detect problems of infection and imbalance.
The most common postoperative complication is respiratory insufficiency, especially in patients who have had poor pulmonary function before surgery. Signs of respiratory problems include a change in mental status related to hypoxia, fever, tachycardia, and tachypnea. Pain is managed with analgesics on a routine basis. In addition to providing comfort and rest for the patient, analgesics allow the patient to move more freely and cough up accumulated secretions more effectively. Pulmonary hygiene is a vital component of postoperative care as it helps the remaining lung increase its vital capacity and total lung capacity and avoid atelectasis.
In patients who are over 60 years of age or have a preexisting cardiac disease, there is the possibility that cardiac arrhythmias can develop. Pain, hypoxemia, hypovolemia, and acid-base imbalance can contribute to this complication. A fistula between the bronchus and pleura sometimes occurs, leading to subcutaneous emphysema and mediastinal shift caused by a massive air leak. If the fistula is evident on the first or second postoperative day, it is probably due to a slipped ligature on the bronchial stump. An air leak that occurs later, on the fifth to tenth postoperative day, is probably due to an infection and poor wound healing. A ruptured bronchial stump must be repaired surgically as soon as possible. Signs that a stump has ruptured include dyspnea, change in mental status, and expectoration of serosanguineous fluid.
Hemorrhage, usually due to a slipped ligature on a major artery, is a relatively rare complication, but when it occurs it can be fatal. The patient rapidly goes into profound shock from circulatory collapse. This complication must be detected early and corrected promptly.
Patients recovering from pneumonectomy require intensive care to avoid the life-threatening complications listed above. Central pressure monitoring, continuous cardiac monitoring, serial laboratory testing of arterial blood gases and electrolyte levels, and frequent periodic checking of vital signs are all necessary either to avoid or to detect and manage these complications in their earliest stages. Additionally, expert care by each member of an interdisciplinary team is necessary to assure an uneventful recovery and restoration of patients to their former daily activities.
After surgical removal of a lung, the chest is closed and there is no closed drainage of the thoracic cavity. Instead, pressure within the pleural space is adjusted by using a simple thoracentesis and manometer, which help maintain the mediastinum midline. Fluid and air are allowed to accumulate in the space left by the excised lung to prevent shift of the mediastinum to the operative side. A second reason for not inserting a chest tube and drainage is the danger of contamination and possible empyema.
The patient is not allowed to lie on the operative side. If the operative lung is permitted to be dependent, fluid can enter the space, causing tension pneumothorax secondary to mediastinal shift; should the bronchial stump rupture, drowning in the accumulated fluid could occur.
Fluid balance is watched closely by pressure monitoring to avoid overhydrating the patient. A central venous line or Swan-Ganz catheter may be used to guide fluid replacement. Serial blood gases and chest x-rays are done to detect early signs of respiratory complications. Additionally, blood tests are done and electrolyte levels are evaluated to detect problems of infection and imbalance.
The most common postoperative complication is respiratory insufficiency, especially in patients who have had poor pulmonary function before surgery. Signs of respiratory problems include a change in mental status related to hypoxia, fever, tachycardia, and tachypnea. Pain is managed with analgesics on a routine basis. In addition to providing comfort and rest for the patient, analgesics allow the patient to move more freely and cough up accumulated secretions more effectively. Pulmonary hygiene is a vital component of postoperative care as it helps the remaining lung increase its vital capacity and total lung capacity and avoid atelectasis.
In patients who are over 60 years of age or have a preexisting cardiac disease, there is the possibility that cardiac arrhythmias can develop. Pain, hypoxemia, hypovolemia, and acid-base imbalance can contribute to this complication. A fistula between the bronchus and pleura sometimes occurs, leading to subcutaneous emphysema and mediastinal shift caused by a massive air leak. If the fistula is evident on the first or second postoperative day, it is probably due to a slipped ligature on the bronchial stump. An air leak that occurs later, on the fifth to tenth postoperative day, is probably due to an infection and poor wound healing. A ruptured bronchial stump must be repaired surgically as soon as possible. Signs that a stump has ruptured include dyspnea, change in mental status, and expectoration of serosanguineous fluid.
Hemorrhage, usually due to a slipped ligature on a major artery, is a relatively rare complication, but when it occurs it can be fatal. The patient rapidly goes into profound shock from circulatory collapse. This complication must be detected early and corrected promptly.
Patients recovering from pneumonectomy require intensive care to avoid the life-threatening complications listed above. Central pressure monitoring, continuous cardiac monitoring, serial laboratory testing of arterial blood gases and electrolyte levels, and frequent periodic checking of vital signs are all necessary either to avoid or to detect and manage these complications in their earliest stages. Additionally, expert care by each member of an interdisciplinary team is necessary to assure an uneventful recovery and restoration of patients to their former daily activities.

Pneumonectomy. From Polaski and Tatro, 1996.
Miller-Keane Encyclopedia and Dictionary of Medicine, Nursing, and Allied Health, Seventh Edition. © 2003 by Saunders, an imprint of Elsevier, Inc. All rights reserved.
pneu·mo·nec·to·my
(nū'mō-nek'tō-mē),Removal of an entire lung.
Synonym(s): pulmonectomy
[G. pneumōn, lung, + ektomē, excision]
Farlex Partner Medical Dictionary © Farlex 2012
pneumonectomy
(no͞o′mə-nĕk′tə-mē, nyo͞o′-) alsopneumectomy
(no͞o-mĕk′tə-mē, nyo͞o-)n. pl. pneumonecto·mies
Surgical removal of all or part of a lung.
The American Heritage® Medical Dictionary Copyright © 2007, 2004 by Houghton Mifflin Company. Published by Houghton Mifflin Company. All rights reserved.
pneumonectomy
Surgery The excision of an entire lungMcGraw-Hill Concise Dictionary of Modern Medicine. © 2002 by The McGraw-Hill Companies, Inc.
pneu·mo·nec·to·my
(nū'mō-nek'tŏ-mē)Removal of all pulmonary lobes from a lung in one operation.
[G. pneumōn, lung, + ektomē, excision]
Medical Dictionary for the Health Professions and Nursing © Farlex 2012
pneumonectomy
Surgical removal of a lung. This is sometimes done to treat cancer limited to one lung.Collins Dictionary of Medicine © Robert M. Youngson 2004, 2005