Pace and Ablate vs AF ablation


These are technically both different types of ablation used to treat AF. So which one is better for you?
AF ablation may be better for some patients and 'pace and ablate' better for others. It depends on your circumstances, previous treatments, and the reversibility of your AF. For those of you who missed last week's post on what 'pace and ablate' is, jump back to that post first- it'll be worth it.
'Pace and ablate' knocks out the conduction from the top and bottom pumping chambers of the heart, leaving a patient dependent on their pacemaker. It's irreversible. Alternatively, AF ablation aims to specifically target the regions in the top chambers that trigger the AF. So if normal sinus rhythm is restored, the patient can return to their natural conduction. However, you can have a recurrence of AF (or other atrial arrhythmias) after AF ablation. This means the AF-associated symptoms or AF-associated cardiac dysfunction could come back.
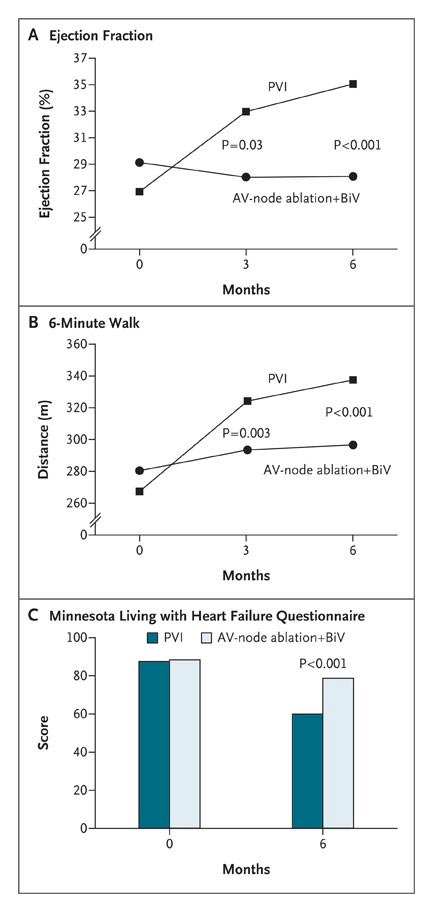
You can think of 'pace and ablate' as the hammer and AF ablation as the scalpel- both have their roles. Last week we looked at a study comparing 'pace and ablate' versus medical management in a highly specific group. One randomised study compared 'pace and ablate' versus AF catheter ablation (specifically 'pulmonary vein isolation' which is the cornerstone technique of AF ablation and something we'll deep dive into next week) specifically in patients with heart failure. The PABA-CHF study compared the relative impact on heart function between 81 patients split between the two treatment groups.
The researchers reported greater improvement in heart pumping function (on the echo scan), exercise capacity, and symptom scores in the AF ablation group compared to 'pace and ablate', although the improvement was seen in both groups. The researchers measured the improvement at 6-months after the ablation- at this timepoint, 88% of patients who had AF ablation remained in sinus rhythm. One benefit of 'pace and ablate' is that it completely eliminates AF from conducting through the heart...forever. So it would have been interesting to see whether this benefit was retained in patients over the longer term when perhaps more of the AF ablation group had a recurrence of their AF. Nevertheless, AF ablation clearly came out on top at this pre-specified timepoint and this work supports AF ablation in heart failure patients.
The authors undertook a great study here- many researchers have compared ablation to medications, and fewer have compared it to a different procedure as the group did here. One particular feature was they didn't rely on just one metric to measure cardiac function- they used 3 different ones to give a more holistic perspective. This is what we're doing in AFHF study by the way (one imaging-based metric, one blood tests-based one and one marker of exercise capacity)
One thing to consider is that, you can have an AF ablation and then have a 'pace and ablate' procedure. This does not work the way round- once you have a 'pace and ablate' you can't reverse it. This is why many Electrophysiologists will suggest an AF ablation procedure in the first instance, and when they feel the AF cannot be reversed with tablets or repeated AF ablation procedures, will they consider 'pace and ablate' treatment- when the AF is permanent and the patient remains highly symptomatic.
If the scalpel doesn't do the job, sometimes you can justify bringing out the hammer
Khan MN, Jaïs P, Cummings J, Di Biase L, Sanders P, Martin DO, Kautzner J, Hao S, Themistoclakis S, Fanelli R, Potenza D, Massaro R, Wazni O, Schweikert R, Saliba W, Wang P, Al-Ahmad A, Beheiry S, Santarelli P, Starling RC, Dello Russo A, Pelargonio G, Brachmann J, Schibgilla V, Bonso A, Casella M, Raviele A, Haïssaguerre M, Natale A; PABA-CHF Investigators. Pulmonary-vein isolation for atrial fibrillation in patients with heart failure. N Engl J Med. 2008 Oct 23;359(17):1778-85. doi: 10.1056/NEJMoa0708234. PMID: 18946063.