Nonadult Supervision of Children in Low- and Middle-Income Countries: Results from 61 National Population-Based Surveys


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Measures of Nonadult Supervision
2.3. Predictors of Nonadult Supervision
2.4. Statistical Analyses
2.5. Ethical Approval
3. Results
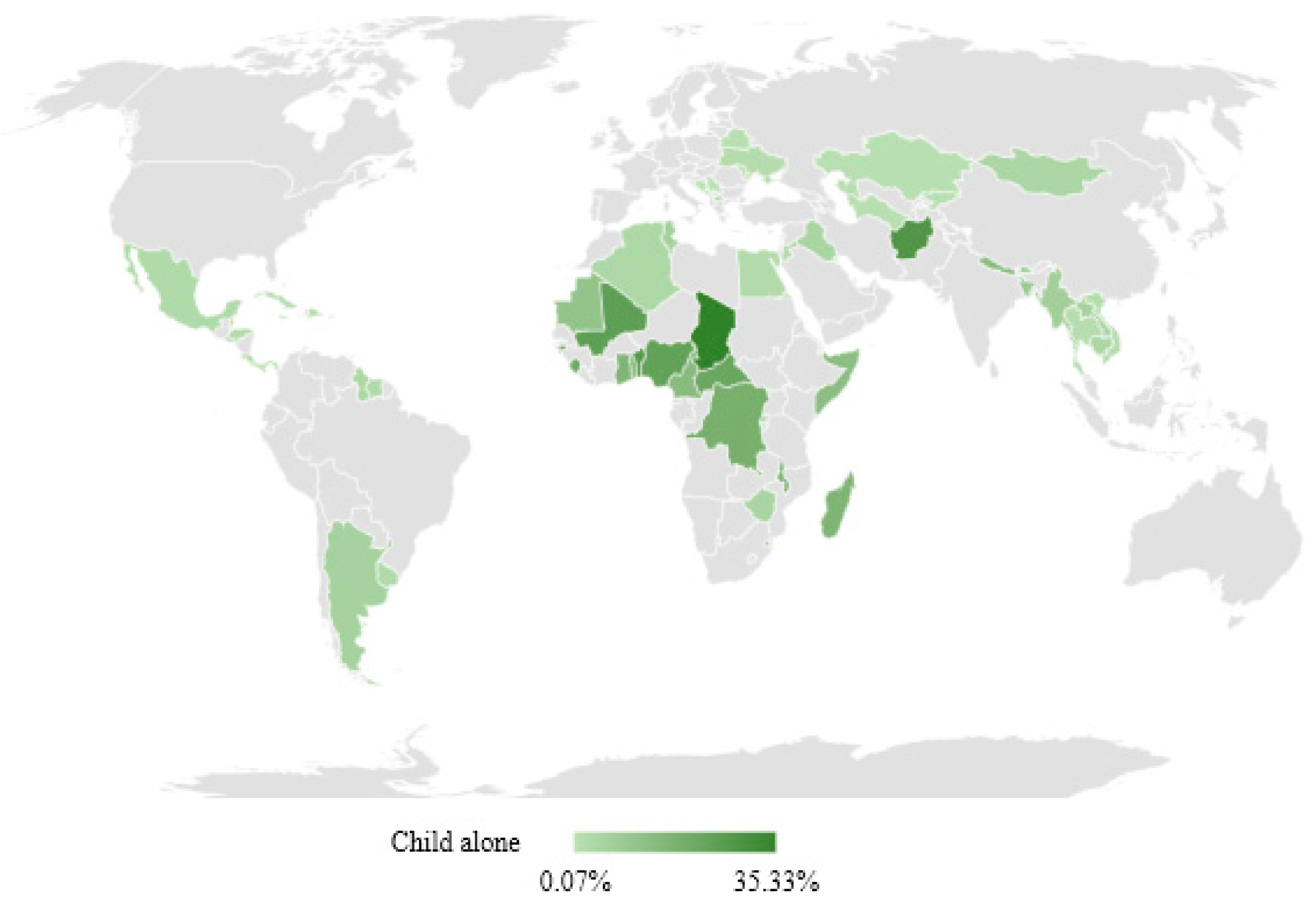
3.1. Prevalence of Child Home Alone
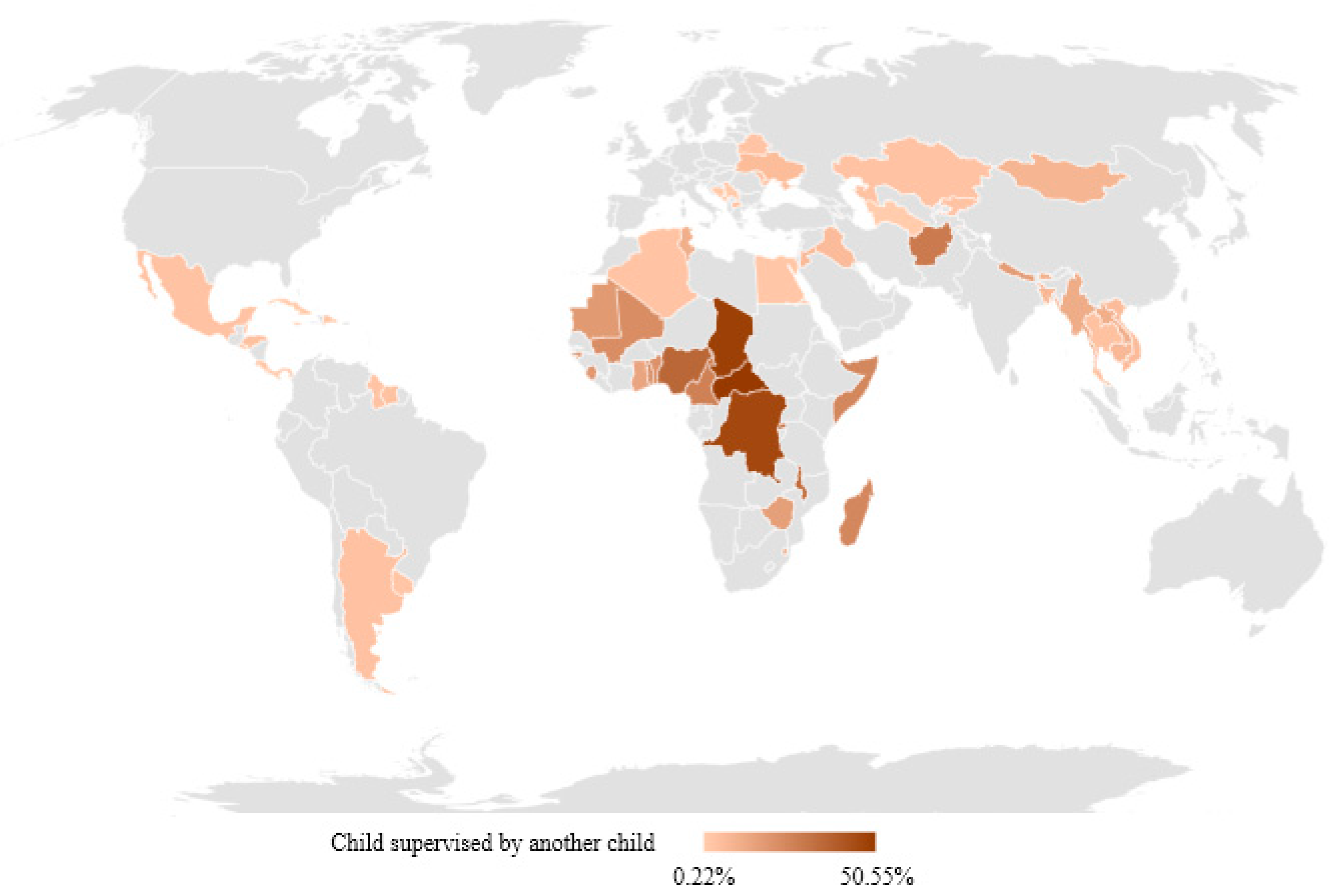
3.2. Prevalence of Child Supervised by Another Child
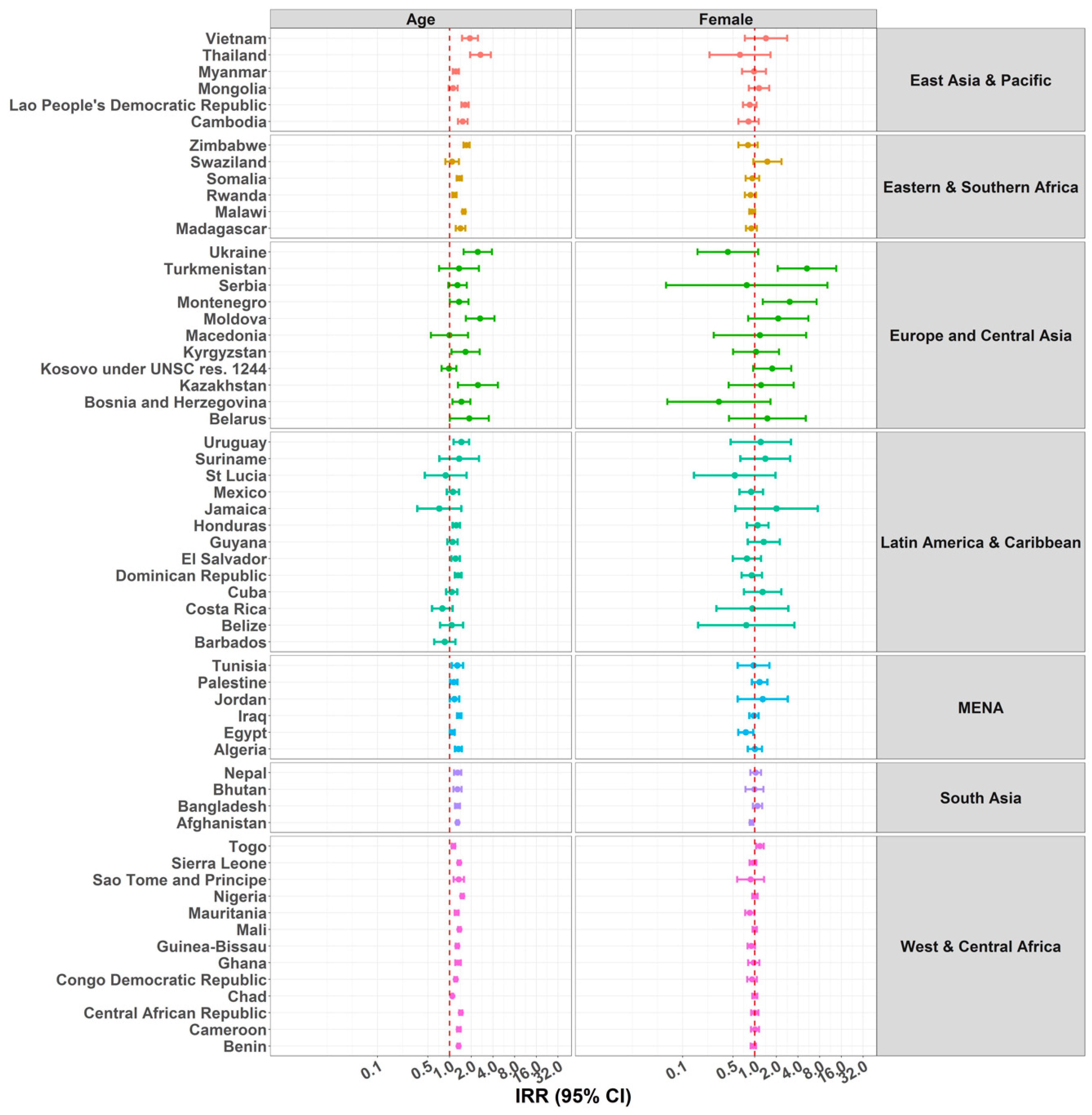
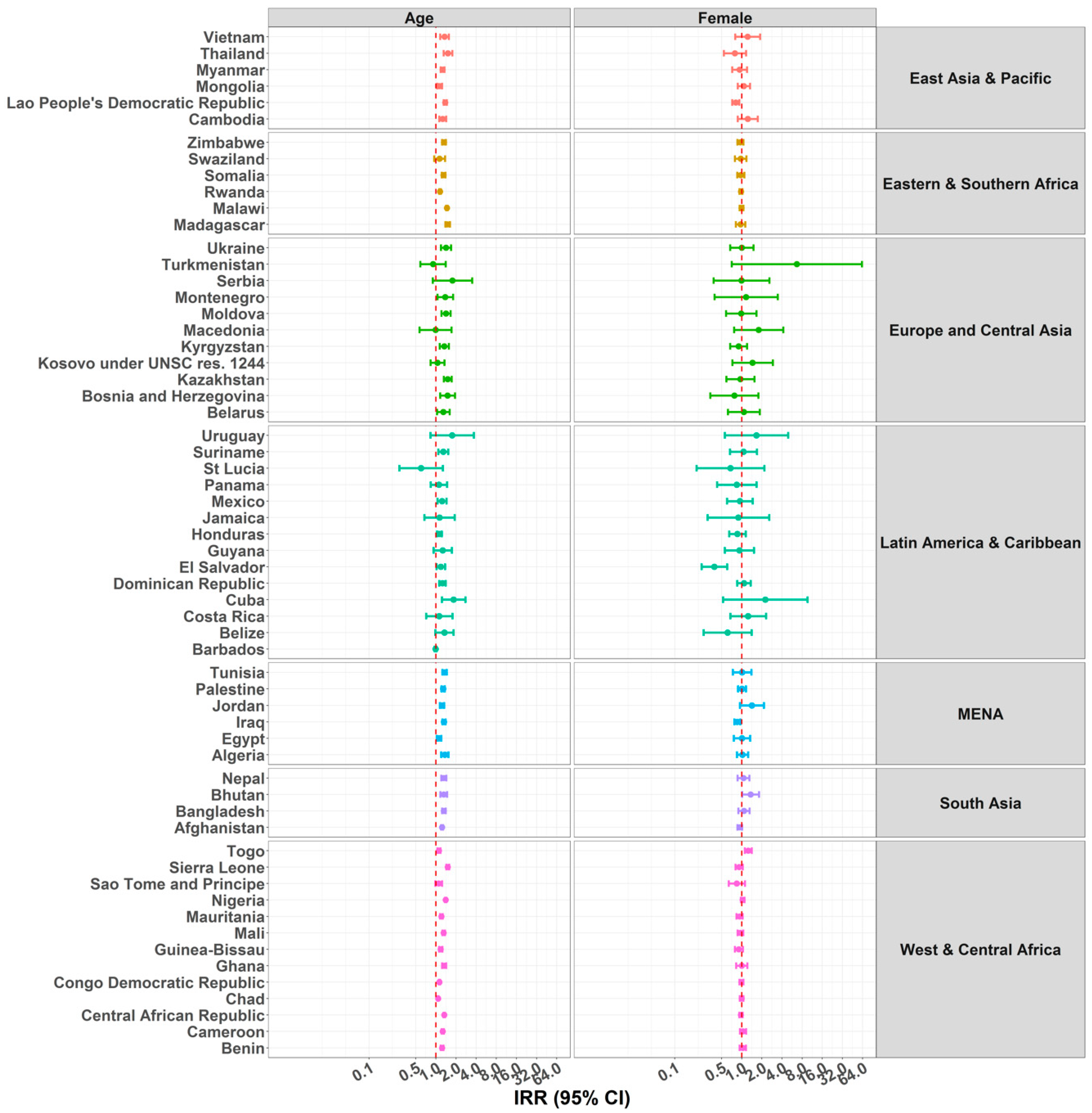
3.3. Child Age and Sex
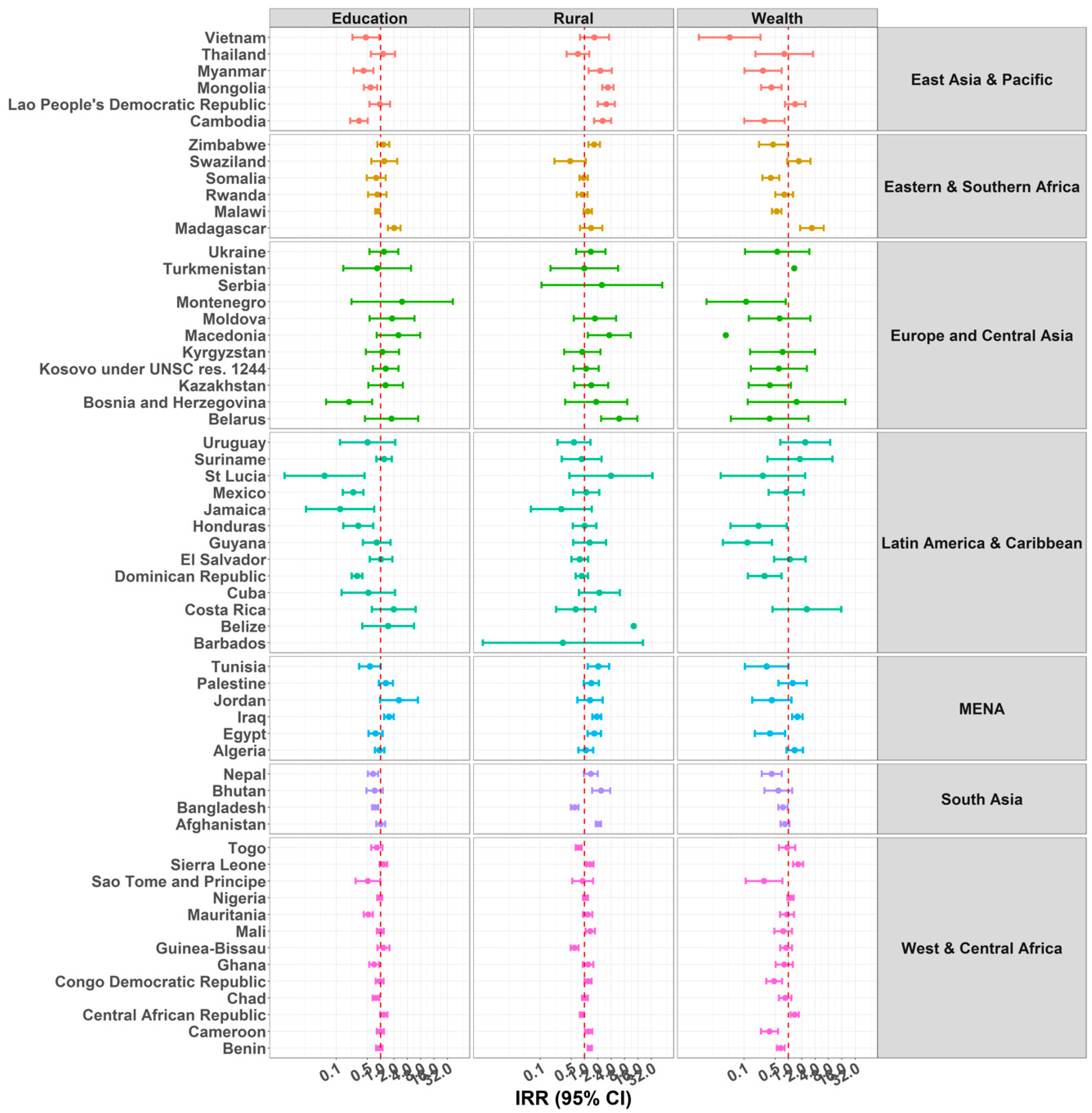
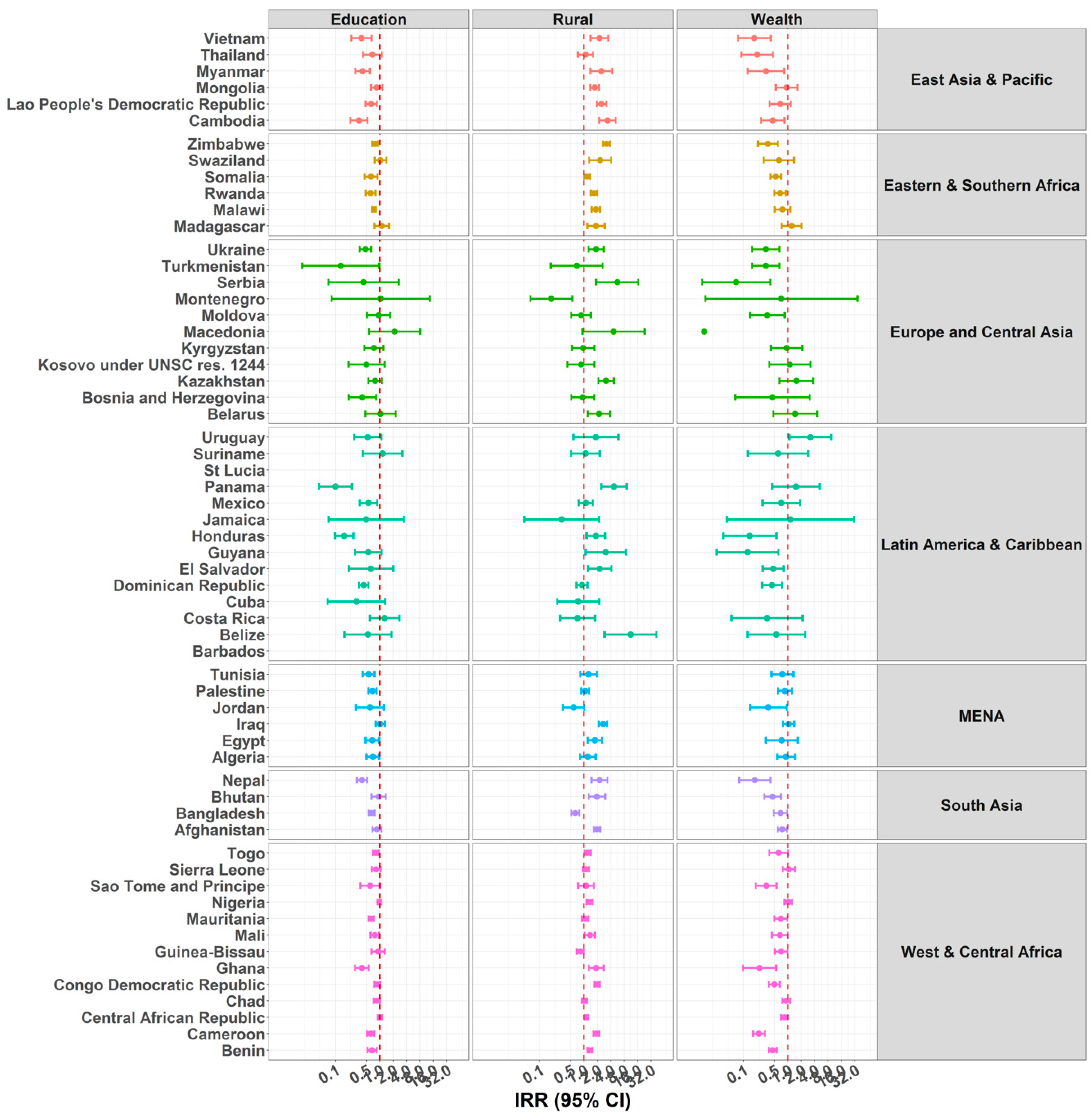
3.4. Mother’s Education
3.5. Rurality and Socio-Economic Status
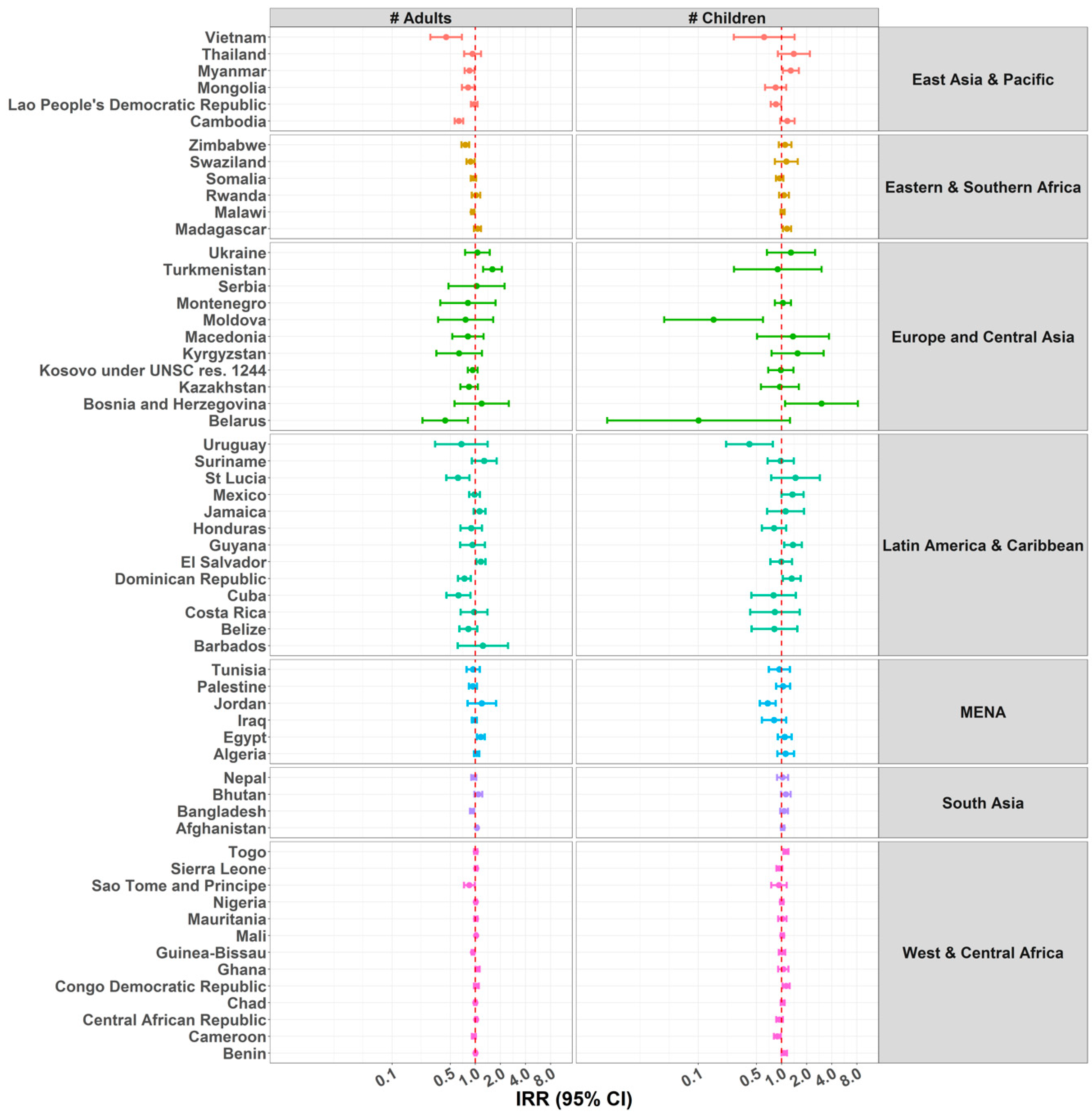
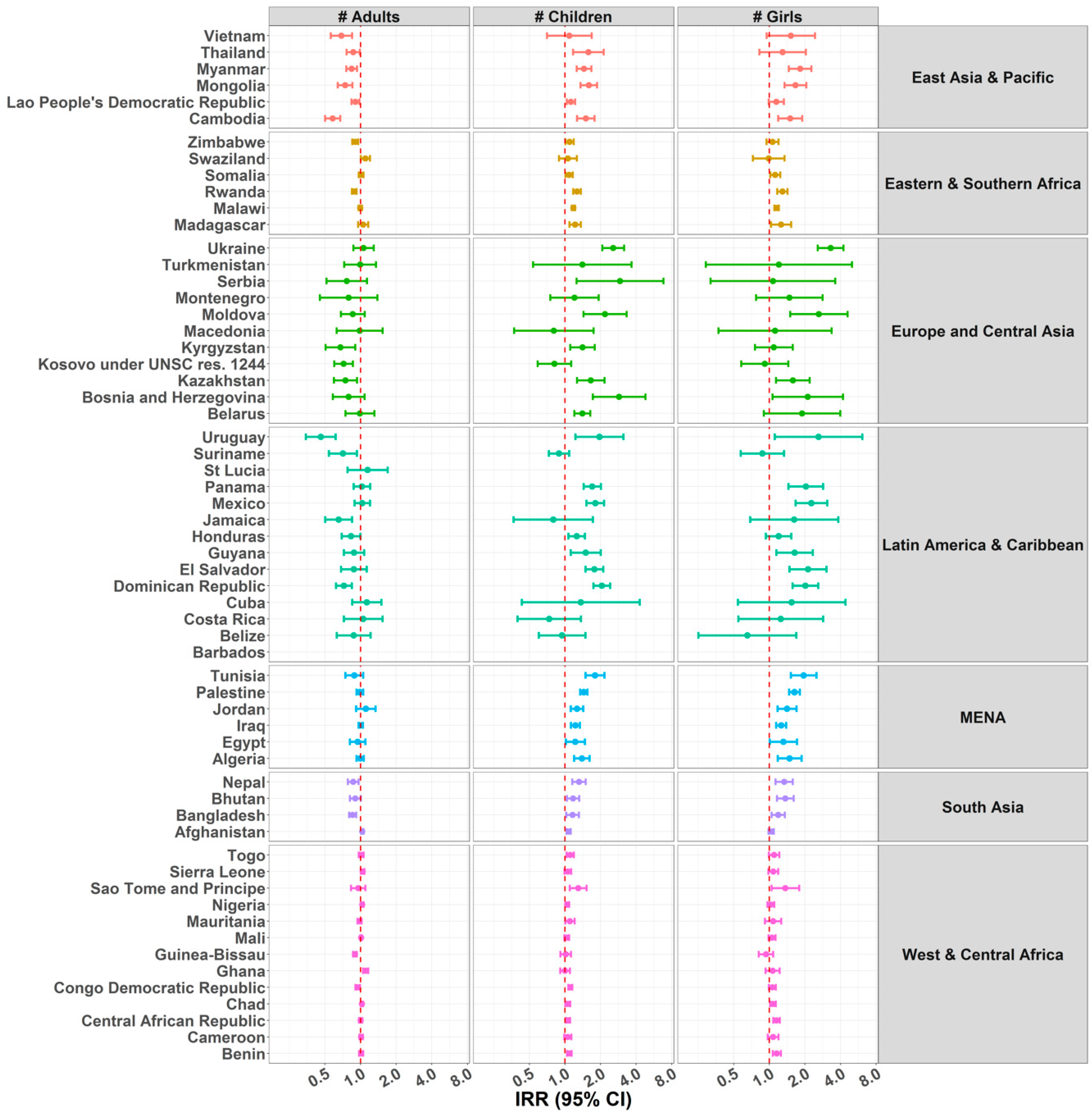
3.6. Number of Individuals in the Household
4. Discussion
4.1. Prevalence of Non-Adult Supervision
4.2. Child Age and Sex
4.3. Mother’s Education
4.4. Rurality and Socio-Economic Status
4.5. Number of Individuals in the Household
4.6. Key Considerations for Future Child Supervision Research
4.7. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schwebel, D.C.; Gaines, J. Pediatric Unintentional Injury: Behavioral Risk Factors and Implications for Prevention. J. Dev. Behav. Pediatr. 2007, 28, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Morrongiello, B.A.; Schmidt, S.; Schell, S.L. Sibling supervision and young children’s risk of injury: A comparison of mothers’ and older siblings’ reactions to risk taking by a younger child in the family. Soc. Sci. Med. 2010, 71, 958–965. [Google Scholar] [CrossRef] [PubMed]
- Morrongiello, B.A.; Zdzieborski, D.; Stewart, J. Supervision of Children in Agricultural Settings: Implications for Injury Risk and Prevention. J. Agromed. 2012, 17, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Peden, M.; Oyegbite, K.; Ozanne-Smith, J.; Hyder, A.A.; Branche, C.; Rahman, A.F.; Rivara, F.; Bartolomeos, K. World Report in Child Injury Prevention; World Health Organization and UNICEF: Geneva, Switzerland, 2008. [Google Scholar]
- Agran, P.F.; Anderson, C.; Winn, D.; Trent, R.; Walton-Haynes, L.; Thayer, S. Rates of Pediatric Injuries by 3-Month Intervals for Children 0 to 3 Years of Age. Pediatrics 2003, 111, e683. [Google Scholar] [CrossRef] [PubMed]
- Schnitzer, P.G.; Dowd, M.D.; Kruse, R.L.; Morrongiello, B.A. Supervision and risk of unintentional injury in young children. Inj. Prev. 2015, 21, e63–e70. [Google Scholar] [CrossRef] [PubMed]
- Morrongiello, B.A.; Ondejko, L.; Littlejohn, A. Understanding Toddlers’ In-Home Injuries: I. Context, Correlates, and Determinants. J. Pediatr. Psychol. 2004, 29, 415–431. [Google Scholar] [CrossRef] [PubMed]
- Damashek, A.; Kuhn, J. Toddlers’ Unintentional Injuries: The Role of Maternal-Reported Paternal and Maternal Supervision. J. Pediatr. Psychol. 2013, 38, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Akers, A.Y.; Muhammad, M.R.; Corbie-Smith, G. “When you got nothing to do, you do somebody”: A community’s perceptions of neighborhood effects on adolescent sexual behaviors. Soc. Sci. Med. 2011, 72, 91–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffin, K.W.; Botvin, G.J.; Scheier, L.M.; Diaz, T.; Miller, N.L. Parenting practices as predictors of substance use, delinquency, and aggression among urban minority youth: Moderating effects of family structure and gender. Psychol. Addict. Behav. 2000, 14, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Buhi, E.R.; Goodson, P. Predictors of adolescent sexual behavior and intention: A theory-guided systematic review. J. Adolesc. Health 2007, 40, 4–21. [Google Scholar] [CrossRef] [PubMed]
- Aizer, A. Home alone: Supervision after School and Child Behavior. J. Public Econ. 2004, 88, 1835–1848. [Google Scholar] [CrossRef]
- Colwell, M.J.; Pettit, G.S.; Meece, D.; Bates, J.E.; Dodge, K.A. Cumulative risk and continuity in nonparental care from infancy to early adolescence. Merrill-Palmer Q. 2001, 47, 207–234. [Google Scholar] [CrossRef]
- Goyette-Ewing, M. Children’s After School Arrangements: A Study of Self-Care and Developmental Outcomes. J. Prev. Interv. Community 2000, 20, 55–67. [Google Scholar] [CrossRef]
- Shumow, L.; Smith, T.J.; Smith, M.C. Academic and Behavioral Characteristics of Young Adolescents in Self-Care. J. Early-Adolesc. 2009, 29, 233–257. [Google Scholar] [CrossRef]
- Ji, K.; Finkelhor, D.; Dunne, M. Child sexual abuse in China: A meta-analysis of 27 studies. Child Abus. Negl. 2013, 37, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Weisner, T.S.; Gallimore, R.; Bacon, M.K.; Barry, H.; Bell, C.; Novaes, S.C.; Edwards, C.P.; Goswami, B.B.; Minturn, L.; Nerlove, S.B.; et al. My Brother’s Keeper: Child and Sibling Caretaking [and Comments and Reply]. Curr. Anthropol. 1977, 18, 169–190. [Google Scholar] [CrossRef]
- Lancy, D. The Anthropology of Childhood: Cherubs, Chattel, and Changelings; Cambridge University Press: New York, NY, USA, 2008. [Google Scholar]
- Whiting, B.B.; Whiting, J.W. Children of Six Cultures: A Psycho-Cultural Analysis; Harvard U Press: Oxford, UK, 1975. [Google Scholar]
- Weisner, T.S. Socialization for parenthood in sibling caretaking societies. In Parenting across the Life Span: Biosocial Dimensions; Aldine Publishing Co.: Hawthorne, NY, USA, 1987; pp. 237–270. [Google Scholar]
- Fouts, H.; Hewlett, B.; Lamb, M.; BirdDavid, N.; Crespi, B.; Gottlieb, A.; HaddixMcKay, K.; Korbin, J.; Sellen, D.; Takada, A.; et al. Parent-Offspring Weaning Conflicts among the Bofi Farmers and Foragers of Central Africa. Curr. Anthropol. 2005, 46, 29–50. [Google Scholar] [CrossRef]
- Dahlblom, K.; Herrara, A.R.; Peña, R.; Dahlgren, L. Home Alone: Children as Caretakers in León, Nicaragua. Child. Soc. 2009, 23, 43–56. [Google Scholar] [CrossRef] [Green Version]
- Suda, C. Street children in Nairobi and the African cultural ideology of kin-based support system. Change and challenge. Child Abus. Rev. 1997, 6, 199–217. [Google Scholar] [CrossRef]
- LeVine, R.A.; Dixon, S.; Richman, A.; Keefer, C.H.; Leiderman, P.H.; Brazelton, T.B. Child Care and Culture: Lessons from Africa; Harvard University Press: Cambridge, MA, USA, 1994. [Google Scholar]
- Kosonen, M. Siblings as Providers of Support and Care during Middle Childhood: Children’s Perceptions. Child. Soc. 1996, 10, 267–279. [Google Scholar] [CrossRef]
- Yi, S.; Poudel, K.C.; Yasuoka, J.; Palmer, P.H.; Yi, S.; Yanagisawa, S.; Jimba, M. Sibling care, school performance, and depression among adolescent caretakers in Cambodia. Asian J. Psychiatry 2012, 5, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Morrongiello, B.A.; Schell, S.L.; Keleher, B. Advancing our understanding of sibling supervision and injury risk for young children. Soc. Sci. Med. 2013, 96, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Liu, X.-X.; Liu, Y.-X.; Lin, Y.; Shen, M. Incidence and risk factors of non-fatal injuries in Chinese children aged 0-6 years: A case-control study. Injury 2010, 42, 521–524. [Google Scholar] [CrossRef] [PubMed]
- Morrongiello, B.A.; MacIsaac, T.J.; Klemencic, N. Older siblings as supervisors: Does this influence young children’s risk of unintentional injury? Soc. Sci. Med. 2007, 64, 807–817. [Google Scholar] [CrossRef] [PubMed]
- Halawa, E.F.; Barakat, A.; Rizk, H.I.I.; Moawad, E.M.I. Epidemiology of non-fatal injuries among Egyptian children: A community-based cross-sectional survey. BMC Public Health 2015, 15, 1248. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Casares, M.; Heymann, J. Children home alone unsupervised: Modeling parental decisions and associated factors in Botswana, Mexico, and Vietnam. Child Abus. Negl. 2009, 33, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Vandivere, S.; Tour, K.; Zaslow, M.; Calkins, J.; Capizzano, J. Unsupervised time. Family and child factors associated with self-care. In Occasional Paper Number 71; The Urban Institute: Washington, DC, USA, 2003. [Google Scholar]
- Casper, L.M.; Smith, K.E. Self-Care: Why do Parents Leave Their Children Unsupervised? Demography 2004, 41, 285–301. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.; Casper, L. Home alone: Reasons parents leave their children unsupervised. In Unpublished Paper Presented at the Annual Meetings of the Population Association of America; Population Association of America: New York, NY, USA, 1999. [Google Scholar]
- Hofferth, S.L.; Jankuniene, Z.; Brandon, P. Self-Care among School-Age Children. Unpublished work. 2000. [Google Scholar]
- Casper, L.M.; Smith, K.E. Dispelling the myths: Self-care, class, and race. J. Fam. Issues 2002, 23, 716–727. [Google Scholar] [CrossRef]
- Cain, V.S.; Hofferth, S.L. Parental Choice of Self-Care for School-Age Children. J. Marriage Fam. 1989, 51, 65–77. [Google Scholar] [CrossRef]
- Cohen, D.A.; Farley, T.A.; Taylor, S.N.; Martin, D.H.; Schuster, M.A. When and Where Do Youths Have Sex? The Potential Role of Adult Supervision. Pediatrics 2002, 110, e66. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Multiple Indicator Cluster Surveys; UNICEF: New York, NY, USA, 2015. [Google Scholar]
- MEASURE DHS. Journalists’ Guide to the Demographic and Health Surveys; MEASURE DHS: Rockville, MD, USA, 2012. [Google Scholar]
- Hancioglu, A.; Arnold, F. Measuring Coverage in MNCH: Tracking Progress in Health for Women and Children Using DHS and MICS Household Surveys. PLoS Med. 2013, 10, e1001391. [Google Scholar] [CrossRef] [PubMed]
- Larsen, K.; Merlo, J. Appropriate Assessment of Neighborhood Effects on Individual Health: Integrating Random and Fixed Effects in Multilevel Logistic Regression. Am. J. Epidemiol. 2005, 161, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Merlo, J.; Chaix, B.; Ohlsson, H.; Beckman, A.; Johnell, K.; Hjerpe, P.; Råstam, L.; Larsen, K. A brief conceptual tutorial of multilevel analysis in social epidemiology: Using measures of clustering in multilevel logistic regression to investigate contextual phenomena. J. Epidemiol. Community Health 2006, 60, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Rabe-Hesketh, S.; Skrondal, A.; Pickles, A. Maximum likelihood estimation of limited and discrete dependent variable models with nested random effects. J. Econom. 2005, 128, 301–323. [Google Scholar] [CrossRef] [Green Version]
- Textor, J.; van der Zander, B.; Gilthorpe, M.S.; Liśkiewicz, M.; Ellison, G.T.H. Robust causal inference using directed acyclic graphs: The R package ‘dagitty’. Int. J. Epidemiol. 2016, 45, 1887–1894. [Google Scholar] [CrossRef] [PubMed]
- Westreich, D.; Greenland, S. The table 2 fallacy: Presenting and interpreting confounder and modifier coefficients. Am. J. Epidemiol. 2013, 177, 292–298. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Statistical Software: Release 14; StataCorp LP: College Station, TX, USA, 2015. [Google Scholar]
- Smith, K. Who’s Minding the Kids? Child Care Arrangements: Spring 1997; U.S. Census Bureau: Washington, DC, USA, 2002; pp. 70–86.
- O’Connell, M.; Casper, L.M. Where have all the hours gone? Uncovering and resolving problems in questionnaire design: The case of estimating children’s self-care. In Annual Meeting of the Population Association of America; Population Association of America: San Francisco, CA, USA, 1995. [Google Scholar]
- Kerrebrock, N.; Lewitt, E.M. Children in self-care. Future Child. 1999, 9, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Evans, R. Sibling caringscapes: Time-space practices of caring within youth-headed households in Tanzania and Uganda. Geoforum 2012, 43, 824–835. [Google Scholar] [CrossRef]
- Miconi, D.; Robert, E.; Beeman, I.; Beatson, J.; Ruiz-Casares, M. Child Supervision in Low- and Middle-Income Countries: A Scoping Review. Child. Youth Serv. Rev. 2018, 89, 226–242. [Google Scholar] [CrossRef]
- Morrongiello, B.A.; Dawber, T. Parental Influences on Toddlers’ Injury-Risk Behaviors: Are Sons and Daughters Socialized Differently? J. Appl. Dev. Psychol. 1999, 20, 227–251. [Google Scholar] [CrossRef]
- Stewart, S.M.; Bond, M.H.; Abdullah, A.S.M.; Ma, S.S.L. Gender, Parenting, and Adolescent Functioning in Bangladesh. Merrill-Palmer Q. 2000, 46, 540–564. [Google Scholar]
- Leroy, J.L.; Gadsden, P.; Guijarro, M. The impact of daycare programmes on child health, nutrition and development in developing countries: A systematic review. J. Dev. Eff. 2012, 4, 472–496. [Google Scholar] [CrossRef]
- World Bank. Rural Population (% of Total Population); World Bank Group: Washington, DC, USA, 2018. [Google Scholar]
- Tronick, E.Z.; Morelli, G.A.; Winn, S. Multiple Caretaking of Efe (Pygmy) Infants. Am. Anthropol. 1987, 89, 96–106. [Google Scholar] [CrossRef]
- Winn, S.A. Non-Maternal Infant Care among the Efe and Lese of Zaire: How Much and by Whom. Ph.D. Thesis, 1896—February 2014. University of Massachusetts Amherst, Amherst, MA, USA, 1991. Available online: https://scholarworks.umass.edu/dissertations_1/3238 (accessed on 24 July 2018).
- Rheinländer, T.; Samuelsen, H.; Dalsgaard, A.; Konradsen, F. Teaching minority children hygiene: Investigating hygiene education in kindergartens and homes of ethnic minority children in northern Vietnam. Ethn. Health 2015, 20, 258–272. [Google Scholar] [CrossRef] [PubMed]
- Hafford, C. Sibling caretaking in immigrant families: Understanding cultural practices to inform child welfare practice and evaluation. Eval. Program Plan. 2010, 33, 294–302. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Inequities in Early Childhood Development. What the Data Say: Evidence from the Multiple Indicator Cluster Surveys; UNICEF: New York, NY, USA, 2012. [Google Scholar]
- Coope, C.M.; Theobald, S. Children at Risk of Neglect: Challenges Faced by Child Protection Practitioners in Guatemala City. Child Abus. Negl. Int. J. 2006, 30, 523–536. [Google Scholar] [CrossRef] [PubMed]
- WORLD Policy Analysis Center. Do Families Receive Benefits for Child Care or School Costs? UCLA’s WORLD Policy Analysis Center: Los Angeles, CA, USA, 2012. [Google Scholar]
- Amdi, V. The Cause of Child Abuse and Neglect and Their Effects on the Development of Children in Samaru Zaria, Nigeria. Early Child Dev. Care 1990, 58, 31–43. [Google Scholar] [CrossRef]
- Van Niekerk, A.; Seedat, M.; Menckel, E.; Laflamme, L. Caregiver experiences, contextualizations and understandings of the burn injury to their child. Accounts from low-income settings in South Africa. Child Care Health Dev. 2007, 33, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Abebe, T.; Aase, A. Children, AIDS and the politics of orphan care in Ethiopia: The extended family revisited. Soc. Sci. Med. 2007, 64, 2058–2069. [Google Scholar] [CrossRef] [PubMed]
- Bryant, B.K. The Child’s Perspective of Sibling Caretaking and Its Relevance to Understanding Social-Emotional Functioning and Development. In Sibling Interaction across Cultures: Theoretical and Methodological Issues; Zukow, P.G., Ed.; Springer: New York, NY, USA, 1989; pp. 143–164. [Google Scholar]
- Garner, P.W.; Jones, D.C.; Miner, J.L. Social Competence among Low-Income Preschoolers: Emotion Socialization Practices and Social Cognitive Correlates. Child Dev. 1994, 65, 622–637. [Google Scholar] [CrossRef] [PubMed]
- Morrongiello, B.A.; Sandomierski, M.; Schwebel, D.C.; Hagel, B. Are parents just treading water? The impact of participation in swim lessons on parents’ judgments of children’s drowning risk, swimming ability, and supervision needs. Accid. Anal. Prev. 2013, 50, 1169–1175. [Google Scholar] [CrossRef] [PubMed]
- Munro, S.A.; Van Niekerk, A.; Seedat, M. Childhood unintentional injuries: The perceived impact of the environment, lack of supervision and child characteristics. Child Care Health Dev. 2006, 32, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Gaines, J.; Schwebel, D.C. Recognition of home injury risks by novice parents of toddlers. Accid. Anal. Prev. 2009, 41, 1070–1074. [Google Scholar] [CrossRef] [PubMed]
- Korioth, T. Determining when your child is ready to stay home alone. AAP News, 29 January 2012; 33. [Google Scholar]
- Morrongiello, B.A.; Ondejko, L.; Littlejohn, A. Understanding Toddlers’ In-Home Injuries: II. Examining Parental Strategies, and Their Efficacy, for Managing Child Injury Risk. J. Pediatr. Psychol. 2004, 29, 433–446. [Google Scholar] [CrossRef] [PubMed]
- Petrass, L.; Blitvich, J.D.; Finch, C.F. Parent/Caregiver Supervision and Child Injury: A Systematic Review of Critical Dimensions for Understanding This Relationship. Fam. Community Health 2009, 32, 123–135. [Google Scholar] [CrossRef] [PubMed]
- Pant, P.R.; Towner, E.; Pilkington, P.; Ellis, M.; Manandhar, D. Community perceptions of unintentional child injuries in Makwanpur district of Nepal: A qualitative study. BMC Public Health 2014, 14, 476. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Casares, M.; Rousseau, C. Between freedom and fear: Children’s views on home alone. Br. J. Soc. Work 2010, 40, 2560–2577. [Google Scholar] [CrossRef]
- Skovdal, M.; Andreouli, E. Using Identity and Recognition as a Framework to Understand and Promote the Resilience of Caregiving Children in Western Kenya. J. Soc. Policy 2011, 40, 613–630. [Google Scholar] [CrossRef]
- Cassidy, T.; Giles, M.; McLaughlin, M. Benefit finding and resilience in child caregivers. Br. J. Health Psychol. 2013, 19, 606–618. [Google Scholar] [CrossRef] [PubMed]
- Sanyang, E.; Peek-Asa, C.; Young, T.; Fuortes, L. Child Supervision and Burn Outcome among Admitted Patients at Major Trauma Hospitals in the Gambia. Int. J. Environ. Res. Public Health 2017, 14, 856. [Google Scholar] [CrossRef] [PubMed]
- Gamlin, J.; Camacho, A.Z.; Ong, M.; Hesketh, T. Is domestic work a worst form of child labour? The findings of a six-country study of the psychosocial effects of child domestic work. Child. Geogr. 2015, 13, 212–225. [Google Scholar] [CrossRef]
- Brown, J. Morals and maladies: Life histories of socially distributed care among Aaumbo women in Namibia, Southern Africa. J. Crit. South. Stud. 2013, 1, 60–79. [Google Scholar]
- Padilla, M.L.; Landreth, G.L. Latchkey Children: A Review of the Literature. Child Welf. 1989, 68, 445–454. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | Country | Survey | Language(s) of Survey | Children Aged <5 Years at Home Alone | Children Aged <5 Years at Home Supervised by Another Child <10 Years | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Days/Week (%) | N | Days/Week (%) | N | ||||||||
| 0 | 1≥ | 3≥ | 0 | 1≥ | 3≥ | ||||||
| East Asia and Pacific (EAP) | Cambodia | DHS VII—2014 | Khmer | 95.9 | 4.1 | 2.2 | 7004 | 92.9 | 7.1 | 4.3 | 6991 |
| Lao People’s Democratic Republic | MICS 4—2012 | Lao | 94.5 | 5.5 | 1.6 | 10,988 | 89.2 | 10.8 | 5.4 | 10,807 | |
| Mongolia | MICS 5—2014 | Mongolian | 95.8 | 4.2 | 0.9 | 6051 | 91.8 | 8.3 | 1.7 | 6045 | |
| Myanmar | DHS VII—2016 | Myanmar | 93.3 | 6.7 | 3.2 | 4666 | 88.6 | 11.4 | 5.9 | 4664 | |
| Thailand | MICS 4—2013 | Thai | 98.5 | 1.5 | 0.4 | 9703 | 96.2 | 3.8 | 1 | 9687 | |
| Vietnam | MICS 5—2014 | Vietnamese | 98.4 | 1.6 | 0.6 | 3317 | 94 | 6 | 2 | 3318 | |
| Eastern and Southern Africa (ESA) | Madagascar | MICS 4—2012 | Malagasy | 83.2 | 16.8 | 11.0 | 2983 | 75.6 | 24.4 | 16.6 | 2982 |
| Malawi | MICS 5—2014 | Chichewa; Tumbuka | 82.6 | 17.4 | 7.8 | 18,941 | 66.2 | 33.8 | 17.4 | 18,905 | |
| Rwanda | DHS VII—2015 | Kinyarwanda | 93 | 7 | 3.8 | 7604 | 69.4 | 30.6 | 20.3 | 7580 | |
| Somalia | MICS 4—2011 | Somali | 86.8 | 13.2 | 5.9 | 4674 | 75.7 | 24.3 | 15.1 | 4607 | |
| Swaziland | MICS 5—2014 | siSwati | 93.5 | 6.5 | 3.2 | 2675 | 89.2 | 10.8 | 4.9 | 2679 | |
| Zimbabwe | MICS 5—2014 | Shona; Ndebele | 95.2 | 4.8 | 1.3 | 9883 | 83.9 | 16.1 | 5.7 | 9880 | |
| Europe and Central Asia (ECA) | Belarus | MICS 4—2012 | Russian | 99.5 | 0.6 | 0.1 | 3442 | 96.7 | 3.3 | 0.8 | 3441 |
| Bosnia and Herzegovina | MICS 4—2012 | Bosnian; Serbian; Latin and Cyrillic alphabets | 99.4 | 0.6 | 0.2 | 2296 | 98.6 | 1.4 | 0.9 | 2293 | |
| Kazakhstan | MICS 5—2015 | Kazakh; [Russian] | 99.3 | 0.7 | 0.2 | 5504 | 96.4 | 3.6 | 0.9 | 5503 | |
| Kosovo under UNSC res. 1244 1 | MICS 5—2014 | Albanian; Serbian | 95.9 | 4.1 | 1.1 | 1646 | 96.4 | 3.7 | 0.5 | 1646 | |
| Kyrgyzstan | MICS 5—2014 | Kyrgyz; Russian | 99.3 | 0.7 | 0.2 | 4564 | 96.4 | 3.6 | 1.3 | 4559 | |
| Macedonia | MICS 4—2011 | Macedonian; Albanian | 98.2 | 1.8 | 1 | 1367 | 96.8 | 3.2 | 1.1 | 1359 | |
| Moldova | MICS 4—2012 | Romanian; [Russian] | 98.6 | 1.5 | 0.3 | 1868 | 95 | 5 | 1.6 | 1864 | |
| Montenegro | MICS 5—2013 | Montenegrin | 99 | 1 | 0.4 | 1417 | 98 | 2.1 | 0.6 | 1417 | |
| Serbia | MICS 5—2014 | Serbian | 99.9 | 0.1 | 0 | 2718 | 99.2 | 0.9 | 0.1 | 2718 | |
| Turkmenistan | MICS 5—2016 | Turkmen; Russian | 99.2 | 0.8 | 0 | 3618 | 99.6 | 0.5 | 0.1 | 3757 | |
| Ukraine | MICS 4—2012 | Ukranian; Russian | 98.4 | 1.6 | 0.5 | 4378 | 94.0 | 6.0 | 2.5 | 4376 | |
| Latin America and Caribbean (LAC) | Argentina | MICS 4—2012 | Spanish | 94.3 | 5.7 | 1.7 | 34,137 | 96.1 | 3.9 | 0.7 | 32,727 |
| Barbados | MICS 4—2012 | English | 99.1 | 0.9 | 0.7 | 461 | 99.8 | 0.2 | 0.2 | 461 | |
| Belize | MICS 4—2011 | English | 99.2 | 0.8 | 0.1 | 1941 | 98.2 | 1.8 | 0.8 | 1939 | |
| Costa Rica | MICS 4—2011 | Spanish | 98.2 | 1.8 | 0.6 | 2262 | 97.7 | 2.3 | 1.4 | 2259 | |
| Cuba | MICS 5—2014 | Spanish | 97.7 | 2.3 | 0.9 | 5627 | 99.5 | 0.6 | 0.2 | 5626 | |
| Dominican Republic | MICS 5—2014 | Spanish | 98 | 2 | 0.7 | 19,835 | 97.5 | 2.5 | 0.9 | 19,648 | |
| El Salvador | MICS 5—2014 | Spanish | 97.8 | 2.2 | 0.7 | 7333 | 98.6 | 1.4 | 0.2 | 7333 | |
| Guyana | MICS 5—2014 | English | 96.5 | 3.6 | 1.3 | 3355 | 96.6 | 3.4 | 1.2 | 3351 | |
| Honduras | DHS VI—2012 | Spanish | 98.1 | 1.9 | 0.5 | 9973 | 95.8 | 4.3 | 1 | 9961 | |
| Jamaica | MICS 4—2011 | English | 98.8 | 1.2 | 0.4 | 1638 | 99.2 | 0.8 | 0.4 | 1632 | |
| Mexico | MICS 5—2015 | Spanish | 97.2 | 2.8 | 0.3 | 8059 | 96.3 | 3.7 | 0.8 | 8054 | |
| Panama | MICS 5—2013 | Spanish | 98.6 | 1.3 | 0.1 | 5797 | 97.6 | 2.4 | 0.6 | 5794 | |
| St Lucia | MICS 4—2012 | English | 97.3 | 2.7 | 0 | 292 | 97.3 | 2.7 | 0 | 292 | |
| Suriname | MICS 4—2010 | Dutch | 97.4 | 2.6 | 0.4 | 3287 | 96.1 | 3.9 | 0.6 | 3224 | |
| Uruguay | MICS 4—2013 | Spanish | 97.3 | 2.9 | 1.2 | 1599 | 97.6 | 2.5 | 0.5 | 1600 | |
| Middle East and North Africa (MENA) | Algeria | MICS 4—2013 | French | 96.5 | 3.5 | 1 | 14,593 | 96.9 | 3.1 | 1 | 14,562 |
| Egypt | DHS VI—2014 | Arabic | 97.6 | 2.4 | 1 | 15,843 | 98 | 2.0 | 1 | 15,843 | |
| Iraq | MICS 4—2011 | Arabic; Kurdish | 95.5 | 4.5 | 1.9 | 36,309 | 93.7 | 6.3 | 3 | 36,299 | |
| Jordan | DHS VI—2012 | Arabic | 97.9 | 2.2 | 0.5 | 10,284 | 93 | 7 | 1.4 | 10,284 | |
| Palestine | MICS 5—2014 | Arabic | 95.8 | 4.2 | 1.1 | 7816 | 88.5 | 11.5 | 3.3 | 7813 | |
| Tunisia | MICS 4—2012 | Arabic (Tunisian) | 93.9 | 6.1 | 1.8 | 2893 | 89.3 | 10.7 | 3.5 | 2889 | |
| South Asia (SA) | Afghanistan | MICS 4—2011 | Dari; Pashto | 71.5 | 28.5 | 11.1 | 14,442 | 71.0 | 29.0 | 14.9 | 14,127 |
| Bangladesh | MICS 5—2013 | Bengali; [English] | 90.7 | 9.3 | 4.7 | 20,712 | 92.0 | 8.0 | 4.5 | 20,692 | |
| Bhutan | MICS 4—2010 | English (Dzongkha, Lhotshamkha, Sharchopkha) | 93.3 | 6.7 | 2.7 | 6241 | 90.1 | 9.9 | 4.1 | 6236 | |
| Nepal | MICS 5—2014 | Nepali; Maithili; Bhojpuri | 86.8 | 13.2 | 8.2 | 5333 | 83.3 | 16.8 | 11.1 | 5307 | |
| West and Central Africa (WCA) | Benin | MICS 5—2014 | French | 72.5 | 27.6 | 11.1 | 12,232 | 79.1 | 20.9 | 7.6 | 12,234 |
| Cameroon | MICS 5—2014 | French | 85.8 | 14.2 | 7.6 | 7015 | 73.3 | 26.7 | 16.0 | 7004 | |
| Central African Republic | MICS 4—2010 | French | 77.7 | 22.3 | 14.6 | 10,220 | 49.5 | 50.6 | 37.0 | 10,025 | |
| Chad | DHS VII—2015 | English | 64.7 | 35.3 | 20.3 | 10,619 | 51.7 | 48.3 | 31.9 | 10,405 | |
| Congo Democratic Republic | DHS VI—2014 | Kikongo; Lingala; Swahili; Tshiluba | 81.1 | 18.9 | 11 | 8025 | 54.1 | 45.9 | 33.5 | 7890 | |
| Ghana | MICS 4—2011 | English | 83.5 | 16.5 | 10.7 | 7518 | 85.8 | 14.3 | 9.6 | 7531 | |
| Guinea-Bissau | MICS 5—2014 | Portuguese | 78.7 | 21.3 | 16.7 | 7445 | 80.4 | 19.6 | 14.5 | 7395 | |
| Mali | MICS 5—2015 | French (Bamanan; other national languages) | 75.2 | 24.8 | 12.3 | 16,100 | 77.5 | 22.5 | 10.1 | 16,061 | |
| Mauritania | MICS 4—2011 | Arabic | 89.2 | 10.8 | 4.2 | 8954 | 82.1 | 17.9 | 9.3 | 8852 | |
| Nigeria 2 | MICS 4—2011 | English | 76.1 | 23.9 | 12.2 | 25,044 | 64.6 | 35.4 | 19.2 | 24,855 | |
| Sao Tome and Principe | MICS 5—2014 | Portuguese | 92.5 | 7.5 | 2.6 | 2016 | 86.4 | 13.6 | 6.3 | 1991 | |
| Sierra Leone | MICS 4—2010 | English | 79.0 | 21.0 | 11.3 | 8342 | 81.5 | 18.5 | 9.9 | 8290 | |
| Togo | DHS VI—2014 | Adja; Akébou; Akposso; Ana-Ifè; Bassar; Ewé; Kabyè; Kotokoli; Lamba; Mina; Moba; Nawdem; Tchokossi | 82.8 | 17.2 | 10.4 | 6660 | 76.6 | 23.4 | 13.5 | 6611 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz-Casares, M.; Nazif-Muñoz, J.I.; Iwo, R.; Oulhote, Y. Nonadult Supervision of Children in Low- and Middle-Income Countries: Results from 61 National Population-Based Surveys. Int. J. Environ. Res. Public Health 2018, 15, 1564. https://doi.org/10.3390/ijerph15081564
Ruiz-Casares M, Nazif-Muñoz JI, Iwo R, Oulhote Y. Nonadult Supervision of Children in Low- and Middle-Income Countries: Results from 61 National Population-Based Surveys. International Journal of Environmental Research and Public Health. 2018; 15(8):1564. https://doi.org/10.3390/ijerph15081564
Chicago/Turabian StyleRuiz-Casares, Mónica, José Ignacio Nazif-Muñoz, René Iwo, and Youssef Oulhote. 2018. "Nonadult Supervision of Children in Low- and Middle-Income Countries: Results from 61 National Population-Based Surveys" International Journal of Environmental Research and Public Health 15, no. 8: 1564. https://doi.org/10.3390/ijerph15081564