
Peritoneal Carcinosis: What the Radiologist Needs to Know
 , , , , , and
, , , , , and
Abstract
:1. Background
2. What Radiologists Should Know about Imaging Techniques
2.1. Ultrasound
2.2. Computed Tomography
2.3. Magnetic-Resonance Imaging
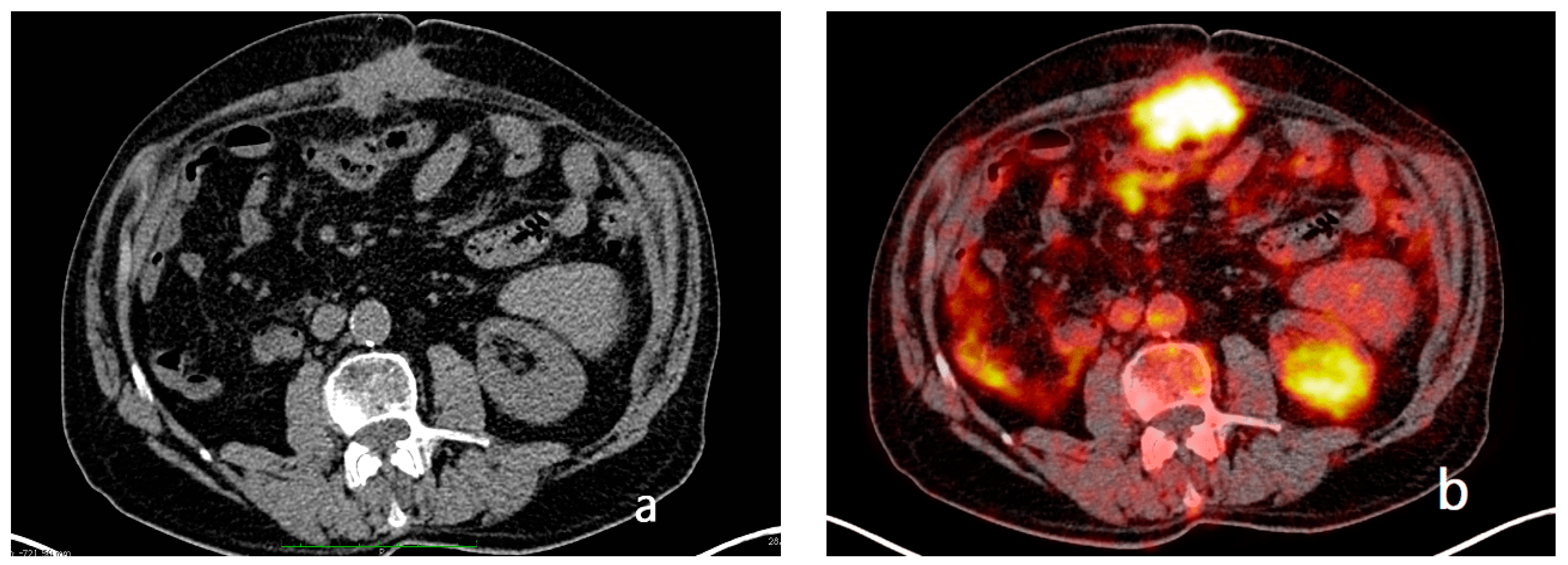
2.4. PET-CT
3. What the Radiologist Should Know about Radiologic Findings
3.1. What Are the Main CT and MRI Findings on Which the Radiologist Should Focus?
3.1.1. Establish the Presence of Peritoneal Metastases
- Nodular pattern: characterized by the presence of nodular implants >5 mm in diameter (Figure 8).
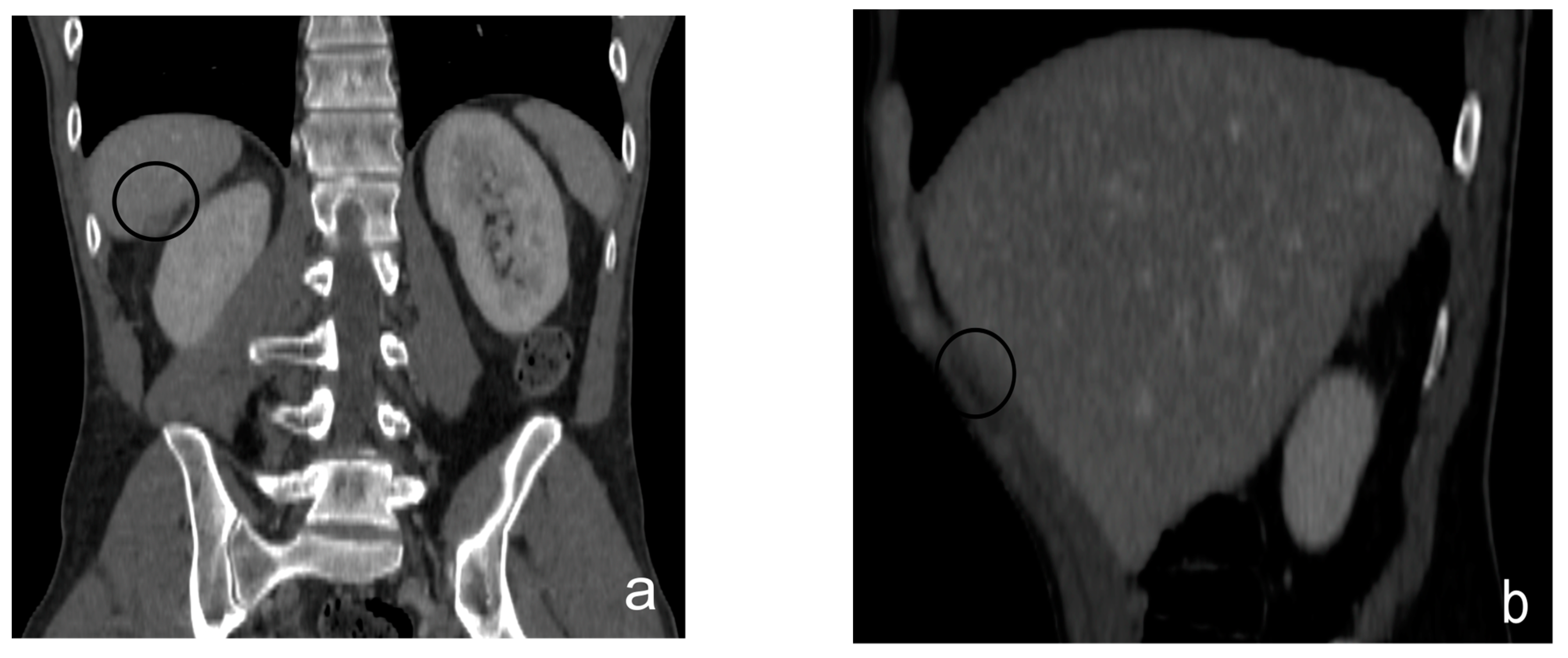
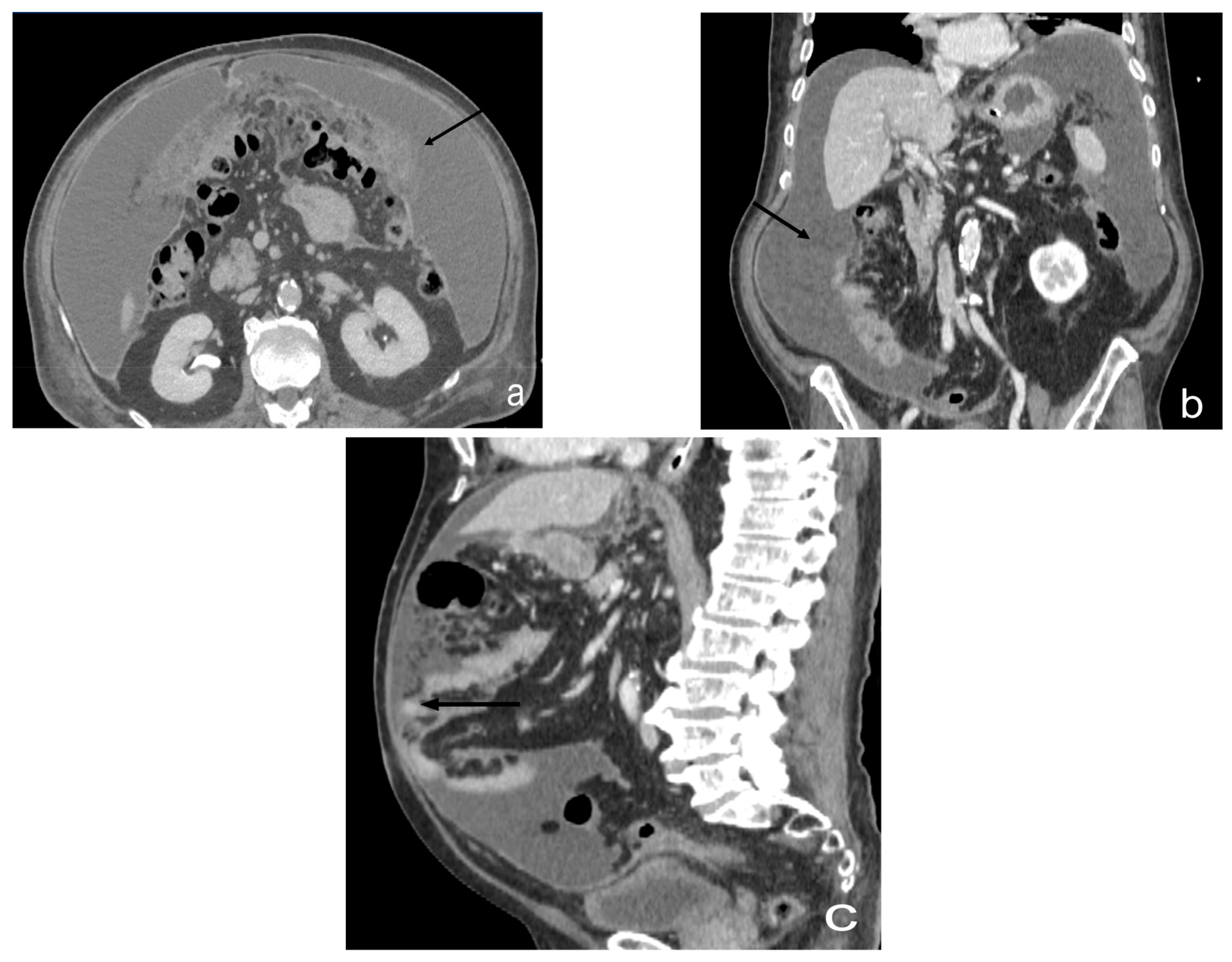
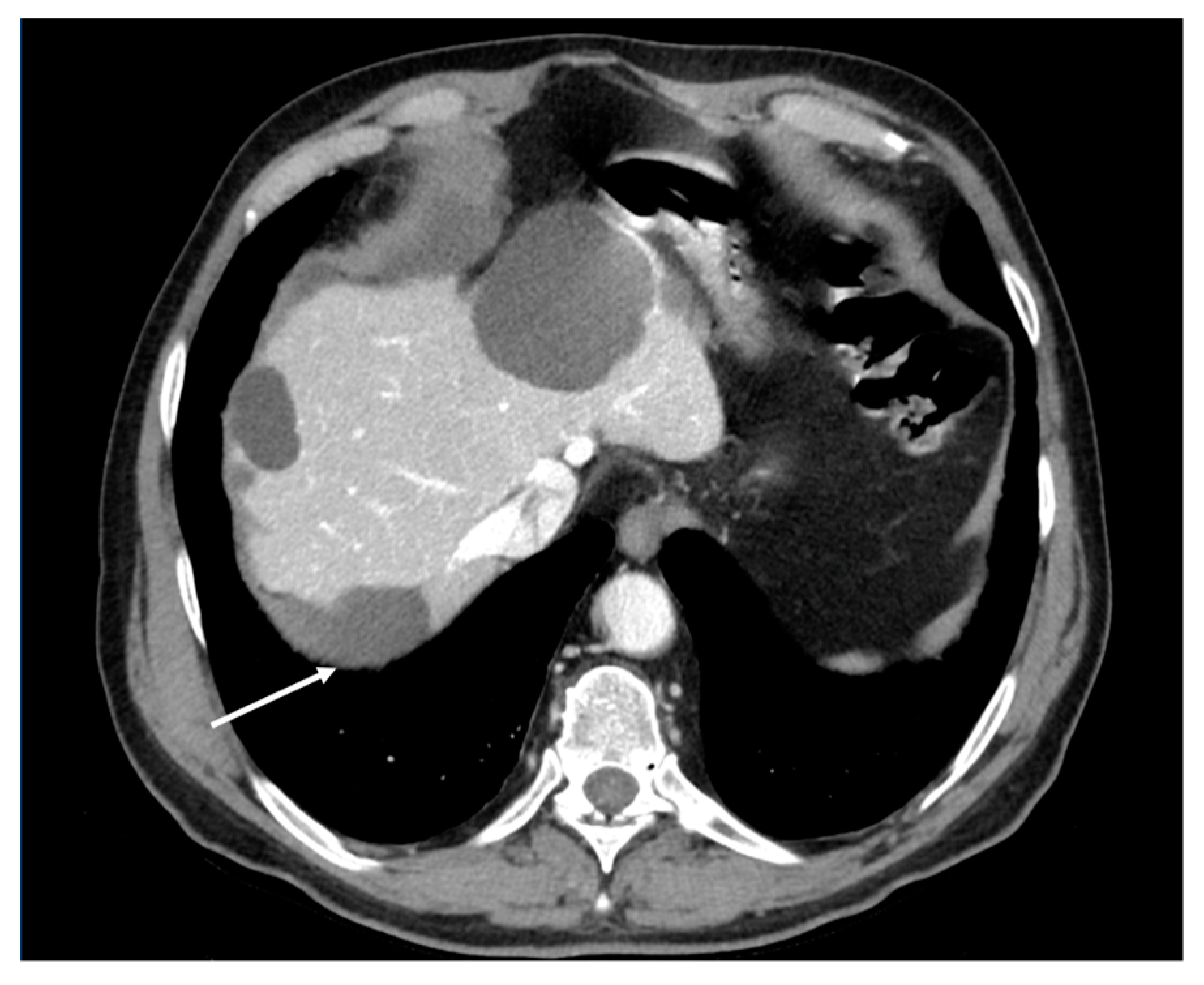
- Plaque pattern: confluent nodular tumor implants that are typically located on the lower surface of the right diaphragm and may manifest as a depression of the liver surface, mimicking capsular or subcapsular liver metastases. They present as areas of low attenuation relative to the parenchyma on postcontrast scans [94,95] (Figure 10).
- Theca pattern: characterized by a nodular thickening of the visceral peritoneum lining the loops of the small bowel. Sometimes, this heteroplasic thickening generates narrowing, with the consequent obstruction and dilation of the proximal loops, a condition also referred to as “frozen pelvis” [95] (Figure 12).
3.1.2. What a Radiologist Needs to Report: “Structured Reporting”
4. What the Radiologist Needs to Know about Treatment
Qualitative Analysis of Lesions and Non-Resectability Criteria
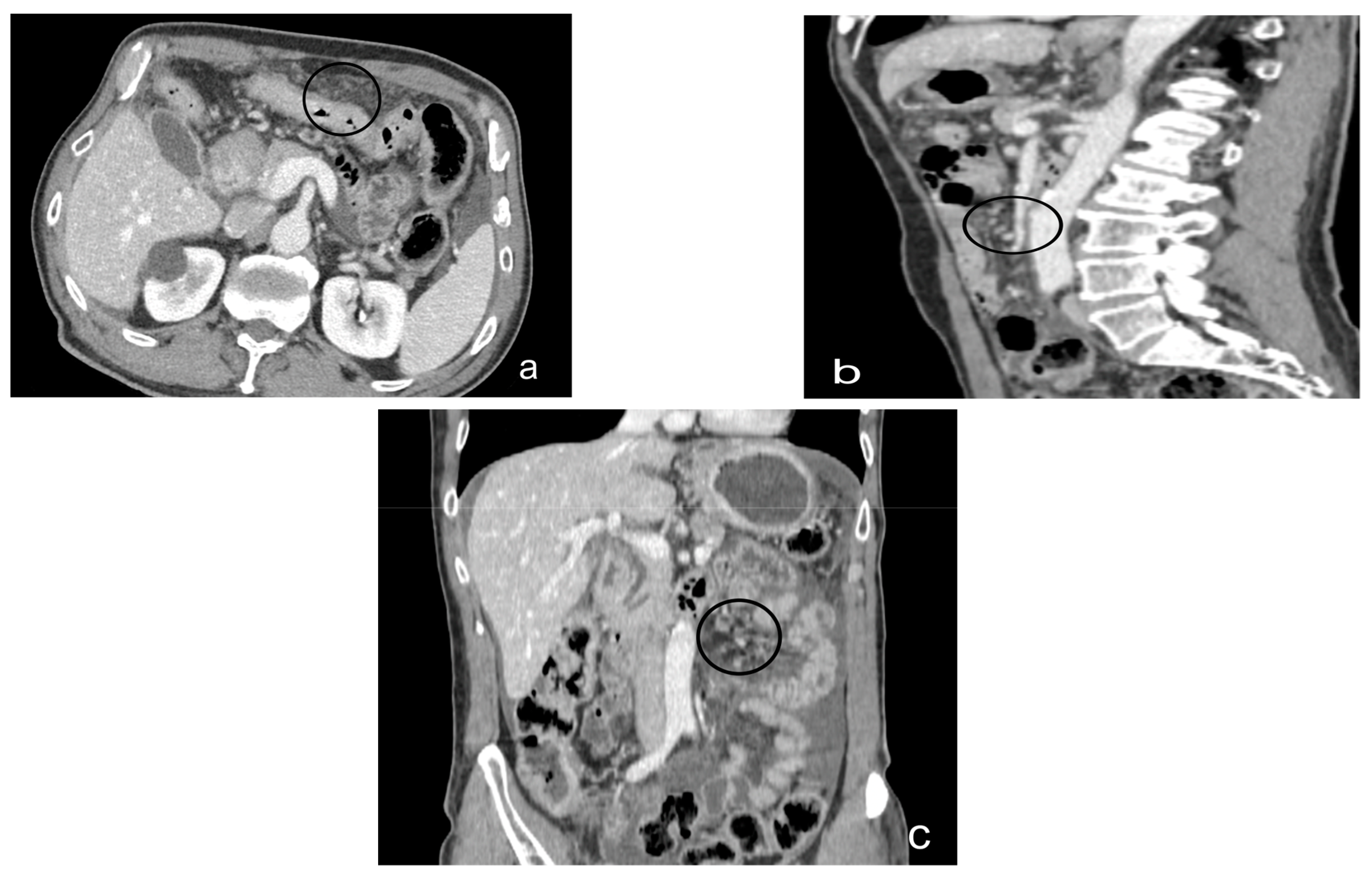
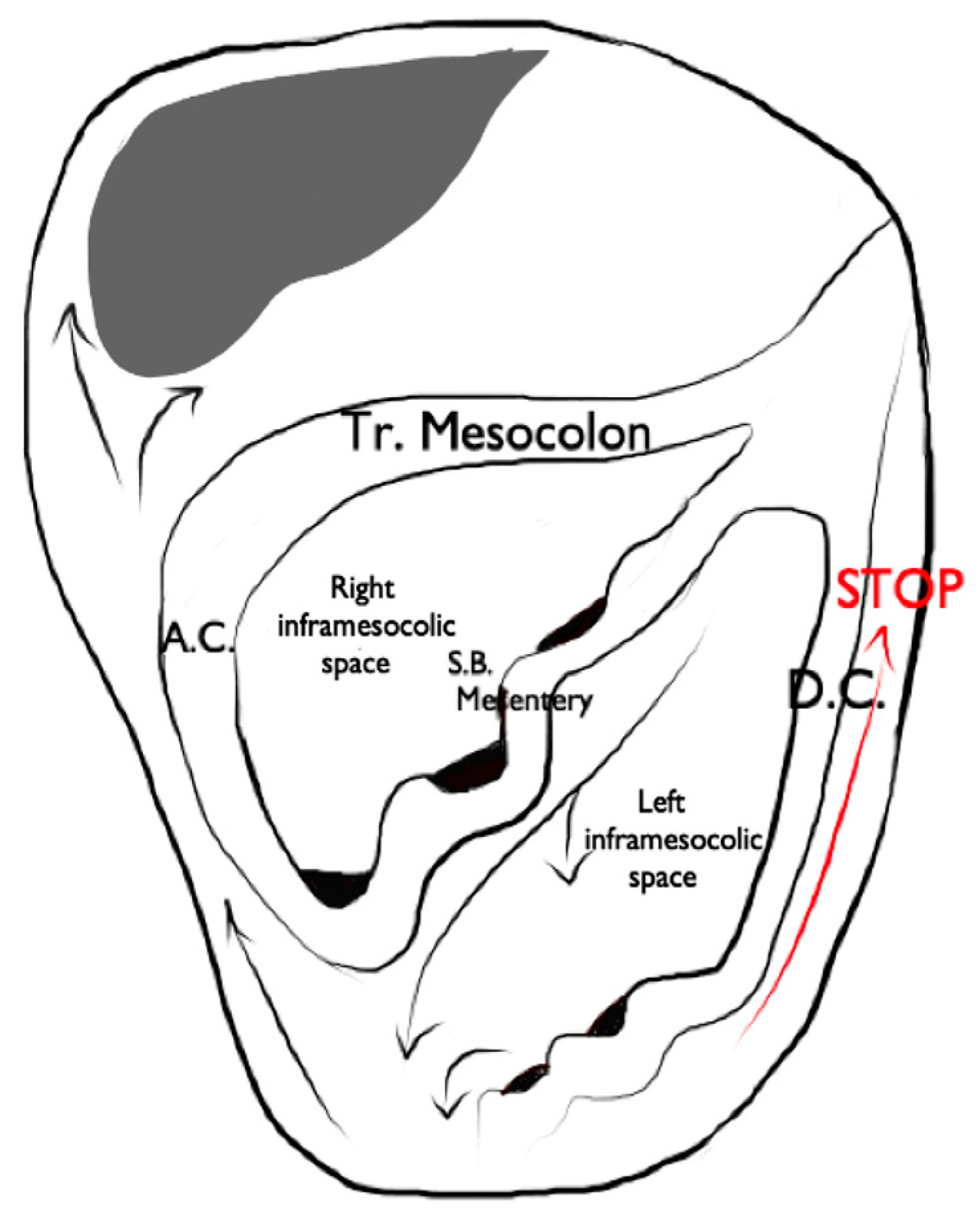
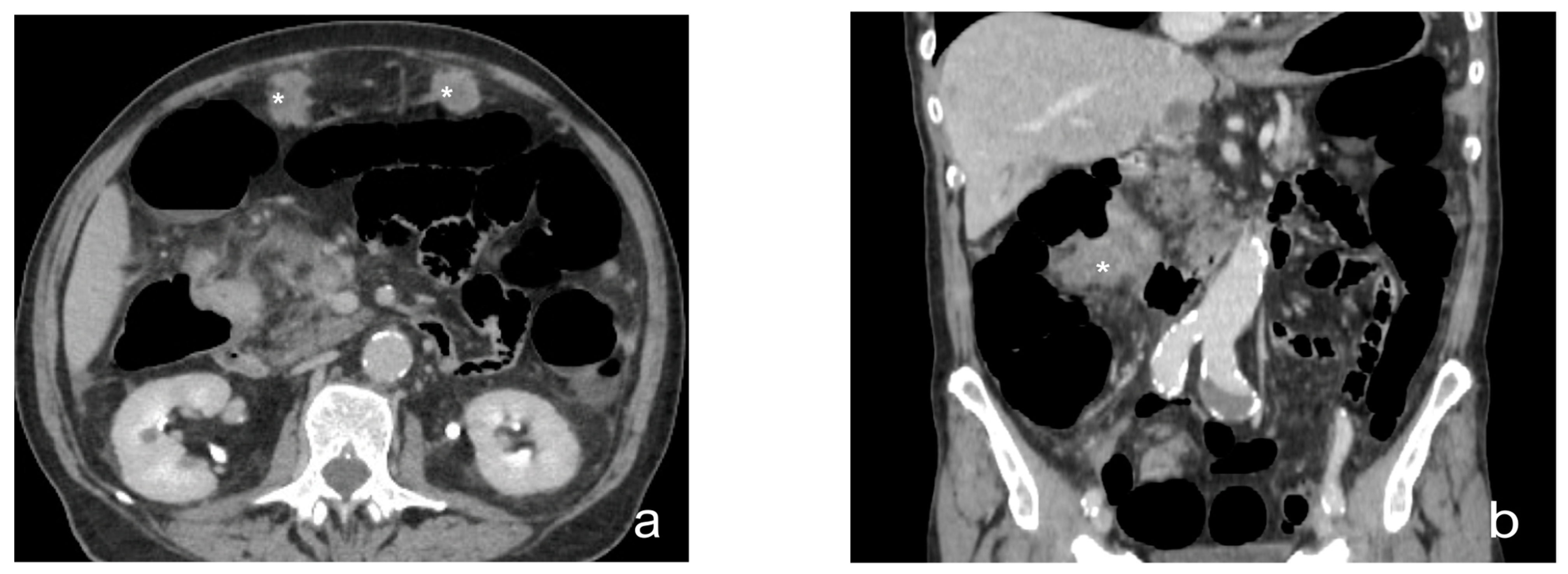
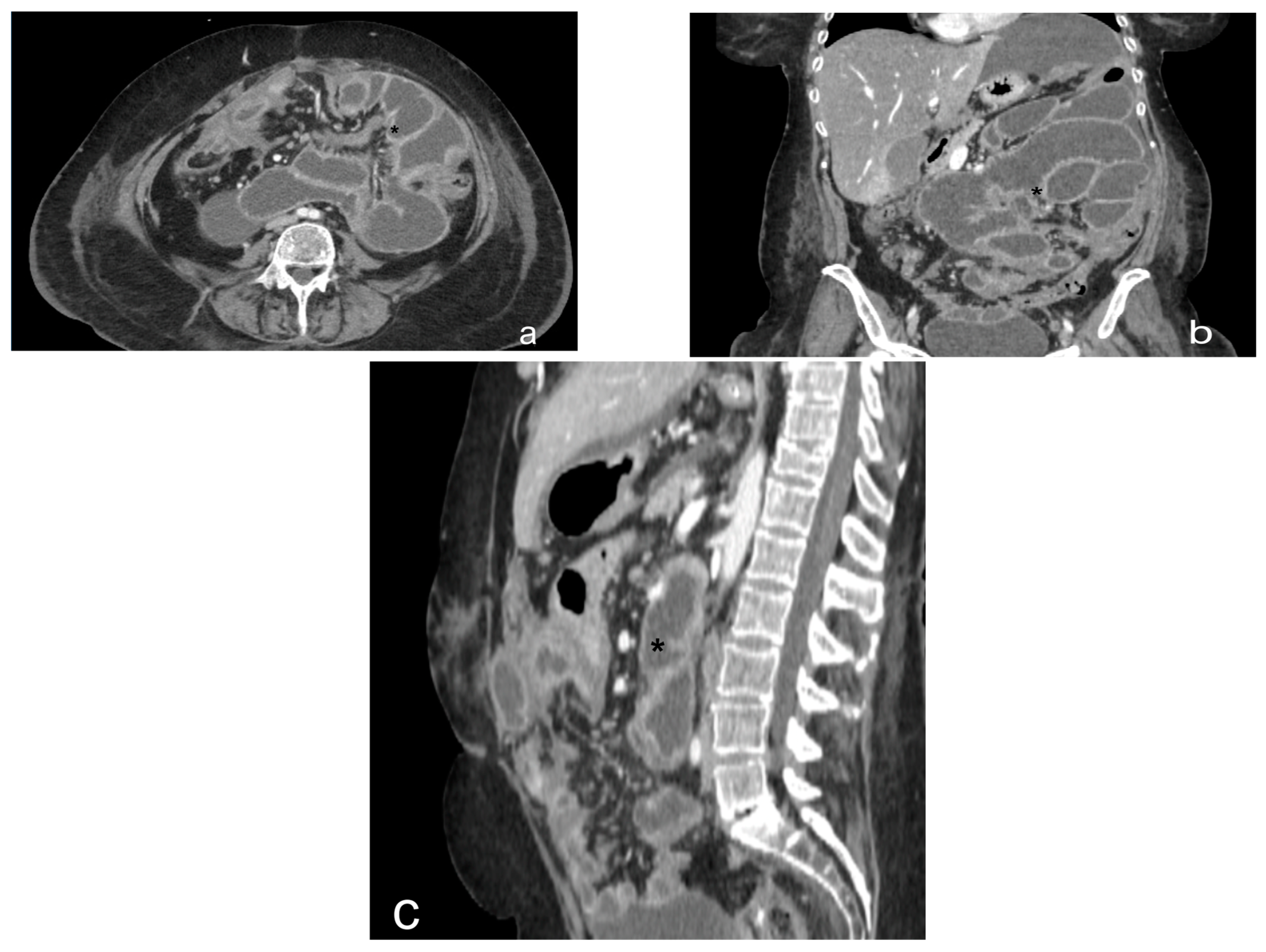
- Mesenteral root involvementDisease in the small bowel and intestinal mesentery constitutes a sentinel and limiting criterion in decision making in CRS. Therefore, the evaluation of small-bowel loops and their mesentery should be a key component in the preoperative imaging evaluation of a patient with PC [24]. The diffuse involvement of the mesentery root is, in fact, a criterion for unresectability. Thin mesenteral tumor sheets are invisible on CT and PET scans [111]. In a study of 30 cases by Dromain et al. [87], CT detected implants in the small bowel in 26% of cases, whereas the true incidence of this disease location at the time of surgery was 83%.Furthermore, MRI has been reported to be superior to CT in the evaluation of the intestinal tract and mesenteric involvement in light of its high capacity in soft-tissue studies [112].Diffuse small-bowel involvement (mesentery and/or intestinal serosa) remains difficult to represent, however, and when present, the radiologist should estimate the extent of involvement as less than or greater than 50%. The radiologist should also describe the number and location of any stenosis of segments of the small intestine, as well as invasion of the colon or gastric system, to produce a complete analysis of the entire digestive tract [69].Indeed, Jacquet et al. [43] found that when preoperative CT showed a tumor causing intestinal obstruction, surgical cytoreduction was suboptimal in 88% of cases. If the tumor obstructing the jejunum or superior ileum was greater than 5 cm in diameter, no subject had a complete CRS.In fact, the two radiologic findings that Sugarbaker et al. [113] reported as most strongly associated with poor outcomes in CRS are the presence of tumor nodules greater than 5 cm on small-bowel surfaces and segmental small-bowel obstruction.Preoperative imaging can aid in patient selection by avoiding surgery for patients whose tumors are excessively large for adequate surgical cytoreduction; in particular MRI using gadolinium and DWI sequences routinely describe tumor-cell sheets involving the serosa of the small intestine and mesentery, which are typically not seen on CT or PET [55] (Figure 14 and Figure 15).
- Hepatic port and hepato-duodenal ligamentThe involvement of the hepato-duodenal ligament or hepatic hilum is a further criterion of unresectability. The radiologist’s task is to evaluate direct signs of tumor infiltration, such as the disappearance of a clear peri-portal fat plane due to tumor replacement and/or indirect signs of biliary and vascular stenosis [66].
- Diffuse infiltrated pelvis (frozen pelvis)A diffusely infiltrated pelvis (known as frozen pelvis) is a condition that precludes cyto-reductive surgery, as well as suggesting the extensive involvement of the bladder and trigonal region. The involvement of the pelvis is best studied with MRI, which is the most sensitive imaging method, thanks to its high-resolution soft-tissue contrast and multi-planar capabilities. In fact, in the absence of ureteral dilatation, this tumor is very difficult to represent on CT or PET-CT [114,115].
5. What Radiologists Need to Know about Key Differential Diagnoses
5.1. Peritoneal Malignant Mesothelioma
5.2. Primary Peritoneal Serous Carcinoma
5.3. Desmoplastic Small Round-Cell Tumor
5.4. Disseminated Peritoneal Leiomyomatosis
5.5. Pseudomyxoma Peritonei
5.6. Lymphomatosiss
5.7. Tuberculosis
6. What Radiologists Need to Know about Radiomics and PCI
7. Conclusions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iafrate, F.; Ciolina, M.; Sammartino, P.; Baldassari, P.; Rengo, M.; Lucchesi, P.; Sibio, S.; Accarpio, F.; Di Giorgio, A.; Laghi, A. Peritoneal carcinomatosis: Imaging with 64-MDCT and 3T MRI with diffusion-weighted imaging. Abdom. Imaging 2012, 37, 616–627. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Fusco, R.; Venanzio Setola, S.; Sassaroli, C.; De Franciscis, S.; Delrio, P.; Danti, G.; Grazzini, G.; Faggioni, L.; Gabelloni, M.; et al. Radiological assessment of peritoneal carcinomatosis: A primer for resident. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 2875–2890. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Stecco, A.; Micci, G.; Sconfienza, L.M.; Colagrande, S.; Reginelli, A.; Grassi, R.; Carriero, A.; Midiri, M.; Lagalla, R.; et al. Whole-body magnetic resonance imaging (WB-MRI) in oncology: An Italian survey. Radiol. Med. 2021, 126, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Macchia, G.; Casà, C.; Ferioli, M.; Lancellotta, V.; Pezzulla, D.; Pappalardi, B.; Laliscia, C.; Ippolito, E.; Di Muzio, J.; Huscher, A.; et al. Observational multicenter Italian study on vulvar cancer adjuvant radiotherapy (OLDLADY 1.2): A cooperation among AIRO Gyn, MITO and MaNGO groups. Radiol. Med. 2022, 127, 1292–1302. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Bhalla, S. Primary neoplasms of peritoneal and sub-peritoneal origin: CT findings. Radiographics 2005, 25, 983–995. [Google Scholar] [CrossRef]
- Avesani, G.; Arshad, M.; Lu, H.; Fotopoulou, C.; Cannone, F.; Melotti, R.; Aboagye, E.; Rockall, A. Radiological assessment of Peritoneal Cancer Index on preoperative CT in ovarian cancer is related to surgical outcome and survival. Radiol. Med. 2020, 125, 770–776. [Google Scholar] [CrossRef]
- Kok, N.F.; de Hingh, I.H. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal metastases of colorectal origin. Br. J. Surg. 2017, 104, 313–315. [Google Scholar] [CrossRef]
- Spiliotis, J.; Halkia, E.; de Bree, E. Treatment of peritoneal surface malignancies with hyperthermic intraperitoneal chemotherapy-current perspectives. Curr. Oncol. 2016, 23, e266–e275. [Google Scholar] [CrossRef] [Green Version]
- Di Giorgio, A.; Naticchioni, E.; Biacchi, D.; Sibio, S.; Accarpio, F.; Rocco, M.; Tarquini, S.; Di Seri, M.; Ciardi, A.; Montruccoli, D.; et al. Cytoreductive surgery (peritonectomy procedures) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) in the treatment of diffuse peritoneal carcinomatosis from ovarian cancer. Cancer 2008, 113, 315–325. [Google Scholar] [CrossRef]
- Huo, Y.R.; Richards, A.; Liauw, W.; Morris, D.L. Hyperthermic intraperitoneal chemotherapy (HIPEC) and cytoreductive surgery (CRS) in ovarian cancer: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2015, 41, 1578–1589. [Google Scholar] [CrossRef]
- Elias, D.; Mariani, A.; Cloutier, A.S.; Blot, F.; Goéré, D.; Dumont, F.; Honoré, C.; Billard, V.; Dartigues, P.; Ducreux, M. Modified selection criteria for complete cytoreductive surgery plus HIPEC based on peritoneal cancer index and small bowel involvement for peritoneal carcinomatosis of colorectal origin. Eur. J. Surg. Oncol. 2014, 40, 1467–1473. [Google Scholar] [CrossRef] [PubMed]
- Fusco, R.; Granata, V.; Sansone, M.; Rega, D.; Delrio, P.; Tatangelo, F.; Romano, C.; Avallone, A.; Pupo, D.; Giordano, M.; et al. Validation of the standardized index of shape tool to analyze DCE-MRI data in the assessment of neo-adjuvant therapy in locally advanced rectal cancer. Radiol. Med. 2021, 126, 1044–1054. [Google Scholar] [CrossRef] [PubMed]
- van ’t Sant, I.; Engbersen, M.P.; Bhairosing, P.A.; Lambregts, D.M.J.; Beets-Tan, R.G.H.; van Driel, W.J.; Aalbers, A.G.J.; Kok, N.F.M.; Lahaye, M.J. Diagnostic performance of imaging for the detection of peritoneal metastases: A meta-analysis. Eur. Radiol. 2020, 30, 3101–3112. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, F.; Berritto, D.; Somma, F.; Cavaliere, C.; Corona, M.; Cozzolino, S.; Fulciniti, F.; Cappabianca, S.; Rotondo, A.; Grassi, R. Magnetic resonance imaging: A new tool for diagnosis of acute ischemic colitis? World J. Gastroenterol. 2012, 18, 1496–1501. [Google Scholar] [CrossRef]
- Rajeev, R.; Turaga, K.K. Hyperthermic Intraperitoneal Chemotherapy and Cytoreductive Surgery in the Management of Peritoneal Carcinomatosis. Cancer Control 2016, 23, 36–46. [Google Scholar] [CrossRef] [Green Version]
- Dohan, A.; Hoeffel, C.; Soyer, P.; Jannot, A.S.; Valette, P.J.; Thivolet, A.; Passot, G.; Glehen, O.; Rousset, P. Evaluation of the peritoneal carcinomatosis index with CT and MRI. Br. J. Surg. 2017, 104, 1244–1249. [Google Scholar] [CrossRef]
- Berritto, D.; Somma, F.; Landi, N.; Cavaliere, C.; Corona, M.; Russo, S.; Fulciniti, F.; Cappabianca, S.; Rotondo, A.; Grassi, R. Seven-Tesla micro-MRI in early detection of acute arterial ischaemia: Evolution of findings in an in vivo rat model. Radiol. Med. 2011, 116, 829–841. [Google Scholar] [CrossRef]
- Klempner, S.J.; Ryan, D.P. HIPEC for colorectal peritoneal metastases. Lancet Oncol. 2021, 22, 162–164. [Google Scholar] [CrossRef]
- Somma, F.; Faggian, A.; Serra, N.; Gatta, G.; Iacobellis, F.; Berritto, D.; Reginelli, A.; Di Mizio, V.; Cappabianca, S.; Di Mizio, R.; et al. Bowel intussusceptions in adults: The role of imaging. Radiol. Med. 2015, 120, 105–117. [Google Scholar] [CrossRef]
- Esquivel, J.; Farinetti, A.; Sugarbaker, P.H. Elective surgery in recurrent colon cancer with peritoneal seeding: When to and when not to proceed. Il G. Di Chir. 1999, 20, 81–86. [Google Scholar]
- Jacquet, P.; Sugarbaker, P.H. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat. Res. 1996, 82, 359–374. [Google Scholar] [CrossRef]
- Duhr, C.D.; Kenn, W.; Kickuth, R.; Kerscher, A.G.; Germer, C.T.; Hahn, D.; Pelz, J.O. Optimizing of preoperative computed tomography for diagnosis in patients with peritoneal carcinomatosis. World J. Surg. Oncol. 2011, 9, 171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nardone, V.; Reginelli, A.; Guida, C.; Belfiore, M.P.; Biondi, M.; Mormile, M.; Banci Buonamici, F.; Di Giorgio, E.; Spadafora, M.; Tini, P.; et al. Delta-radiomics increases multicentre reproducibility: A phantom study. Med. Oncol. 2020, 37, 1–7. [Google Scholar] [CrossRef] [PubMed]
- González-Moreno, S.; González-Bayón, L.; Ortega-Pérez, G.; González-Hernando, C. Imaging of peritoneal carcinomatosis. Cancer J. 2009, 15, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.S.; Liu, C.; Zhang, Y.F.; Sun, L.P.; Xiang, L.H.; Liu, H.; Fang, Y.; Ren, W.W.; Zhao, H.; Sun, X.M.; et al. Contrast-enhanced ultrasound in the assessment of Crohn’s disease activity: Comparison with computed tomography enterography. Radiol. Med. 2022, 127, 1068–1078. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Bhalla, S. Unusual nonneoplastic peritoneal and subperitoneal conditions: CT findings. Radiographics 2005, 25, 719–730. [Google Scholar] [CrossRef] [PubMed]
- Danti, G.; Flammia, F.; Matteuzzi, B.; Cozzi, D.; Berti, V.; Grazzini, G.; Pradella, S.; Recchia, L.; Brunese, L.; Miele, V. Gastrointestinal neuroendocrine neoplasms (GI-NENs): Hot topics in morphological, functional, and prognostic imaging. Radiol. Med. 2021, 126, 1497–1507. [Google Scholar] [CrossRef]
- Hanbidge, A.E.; Lynch, D.; Wilson, S.R. US of the peritoneum. Radiographics 2003, 23, 663–684, discussion 665–684. [Google Scholar] [CrossRef]
- Inadomi, J.; Cello, J.P.; Koch, J. Ultrasonographic determination of ascitic volume. Hepatology 1996, 24, 549–551. [Google Scholar] [CrossRef]
- Goerg, C.; Schwerk, W.B. Peritoneal carcinomatosis with ascites. Am. J. Roentgenol. 1991, 156, 1185–1187. [Google Scholar] [CrossRef] [Green Version]
- Scialpi, M.; Reginelli, A.; D’Andrea, A.; Gravante, S.; Falcone, G.; Baccari, P.; Manganaro, L.; Palumbo, B.; Cappabianca, S. Pancreatic tumors imaging: An update. Int. J. Surg. 2016, 28, S142–S155. [Google Scholar] [CrossRef] [PubMed]
- Yeh, H.C. Ultrasonography of peritoneal tumors. Radiology 1979, 133, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Rioux, M.; Michaud, C. Sonographic detection of peritoneal carcinomatosis: A prospective study of 37 cases. Abdom. Imaging 1995, 20, 47–51, discussion 47–56. [Google Scholar] [CrossRef]
- DeBardeleben, J.; Cohen, M.; Rodgers, S.K. Peritoneal Carcinomatosis Presenting as a Sister Mary Joseph Nodule. Ultrasound Q. 2017, 33, 300–302. [Google Scholar] [CrossRef] [PubMed]
- Di Grezia, G.; Somma, F.; Serra, N.; Reginelli, A.; Cappabianca, S.; Grassi, R.; Gatta, G. Reducing Costs of Breast Examination: Ultrasound Performance and Inter-Observer Variability of Expert Radiologists Versus Residents. Cancer Investig. 2016, 34, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Qi, Z.; Zhang, Y.; Dai, Q.; Xia, Y.; Jiang, Y. Peritoneal Carcinomatosis in Primary Ovarian Cancer: Ultrasound Detection and Comparison with Computed Tomography. Ultrasound Med. Biol. 2017, 43, 1811–1819. [Google Scholar] [CrossRef]
- Liang, L.; Wang, W.; Zhou, N.; Guo, J.; Lu, Y.; Xu, H.; Zhang, S. Value of preoperative ultrasound in evaluating the peritoneal cancer index of pseudomyxoma peritonei. World J. Surg. Oncol. 2019, 17, 192. [Google Scholar] [CrossRef] [Green Version]
- Allah, M.H.; Salama, Z.A.; El-Hindawy, A.; Al Kady, N. Role of peritoneal ultrasonography and ultrasound-guided fine needle aspiration cytology/biopsy of extravisceral masses in the diagnosis of ascites of undetermined origin. Arab. J. Gastroenterol. 2012, 13, 116–124. [Google Scholar] [CrossRef]
- Di Serafino, M.; Vallone, G. The role of point of care ultrasound in radiology department: Update and prospective. A statement of Italian college ultrasound. Radiol. Med. 2021, 126, 636–641. [Google Scholar] [CrossRef]
- Panzironi, G.; Moffa, G.; Galati, F.; Pediconi, F. Ultrasound-guided 8-Gauge vacuum-assisted excision for selected B3 breast lesions: A preliminary experience. Radiol. Med. 2022, 127, 57–64. [Google Scholar] [CrossRef]
- Reginelli, A.; Vanzulli, A.; Sgrazzutti, C.; Caschera, L.; Serra, N.; Raucci, A.; Urraro, F.; Cappabianca, S. Vascular microinvasion from hepatocellular carcinoma: CT findings and pathologic correlation for the best therapeutic strategies. Med. Oncol. 2017, 34, 93. [Google Scholar] [CrossRef] [PubMed]
- Papalexis, N.; Parmeggiani, A.; Facchini, G.; Miceli, M.; Carbone, G.; Cavallo, M.; Spinnato, P. Current concepts in the diagnosis and treatment of adhesive capsulitis: Role of diagnostic imaging and ultrasound-guided interventional procedures. Radiol. Med. 2022, 127, 1390–1399. [Google Scholar] [CrossRef] [PubMed]
- Jacquet, P.; Jelinek, J.S.; Chang, D.; Koslowe, P.; Sugarbaker, P.H. Abdominal computed tomographic scan in the selection of patients with mucinous peritoneal carcinomatosis for cytoreductive surgery. J. Am. Coll. Surg. 1995, 181, 530–538. [Google Scholar]
- Wang, F.H.; Zheng, H.L.; Li, J.T.; Li, P.; Zheng, C.H.; Chen, Q.Y.; Huang, C.M.; Xie, J.W. Prediction of recurrence-free survival and adjuvant therapy benefit in patients with gastrointestinal stromal tumors based on radiomics features. Radiol. Med. 2022, 127, 1085–1097. [Google Scholar] [CrossRef]
- Mistretta, F.; Damiani, N.; Campanella, D.; Mazzetti, S.; Gulino, A.; Cappello, G.; Regge, D. Effect of dose splitting of a low-volume bowel preparation macrogol-based solution on CT colonography tagging quality. Radiol. Med. 2022, 127, 809–818. [Google Scholar] [CrossRef]
- Low, R.N.; Barone, R.M. Imaging for Peritoneal Metastases. Surg. Oncol. Clin. N. Am. 2018, 27, 425–442. [Google Scholar] [CrossRef]
- Mazzei, M.A.; Khader, L.; Cirigliano, A.; Cioffi Squitieri, N.; Guerrini, S.; Forzoni, B.; Marrelli, D.; Roviello, F.; Mazzei, F.G.; Volterrani, L. Accuracy of MDCT in the preoperative definition of Peritoneal Cancer Index (PCI) in patients with advanced ovarian cancer who underwent peritonectomy and hyperthermic intraperitoneal chemotherapy (HIPEC). Abdom. Imaging 2013, 38, 1422–1430. [Google Scholar] [CrossRef] [PubMed]
- Low, R.N. Gadolinium-enhanced MR imaging of liver capsule and peritoneum. Magn. Reson. Imaging Clin. N. Am. 2001, 9, 803–819,vii. [Google Scholar] [CrossRef]
- Low, R.N.; Barone, R.M.; Lacey, C.; Sigeti, J.S.; Alzate, G.D.; Sebrechts, C.P. Peritoneal tumor: MR imaging with dilute oral barium and intravenous gadolinium-containing contrast agents compared with unenhanced MR imaging and CT. Radiology 1997, 204, 513–520. [Google Scholar] [CrossRef]
- Low, R.N.; Sigeti, J.S. MR imaging of peritoneal disease: Comparison of contrast-enhanced fast multiplanar spoiled gradient-recalled and spin-echo imaging. Am. J. Roentgenol. 1994, 163, 1131–1140. [Google Scholar] [CrossRef] [Green Version]
- Rodolfino, E.; Devicienti, E.; Miccò, M.; Del Ciello, A.; Di Giovanni, S.E.; Giuliani, M.; Conte, C.; Gui, B.; Valentini, A.L.; Bonomo, L. Diagnostic accuracy of MDCT in the evaluation of patients with peritoneal carcinomatosis from ovarian cancer: Is delayed enhanced phase really effective? Eur. Rev Med. Pharmacol. Sci. 2016, 20, 4426–4434. [Google Scholar] [PubMed]
- Delgado-Barriga, K.; Medina, C.; Gomez-Quiles, L.; Marco-Domenech, S.F.; Escrig, J.; Llueca, A. CT Enterography for Preoperative Evaluation of Peritoneal Carcinomatosis Index in Advanced Ovarian Cancer. J. Clin. Med. 2022, 11, 476. [Google Scholar] [CrossRef]
- Bagherzadeh, S.; Jabbari, N.; Khalkhali, H.R. Radiation dose and cancer risks from radiation exposure during abdominopelvic computed tomography (CT) scans: Comparison of diagnostic and radiotherapy treatment planning CT scans. Radiat. Environ. Biophys. 2021, 60, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Cicero, G.; Mazziotti, S.; Silipigni, S.; Blandino, A.; Cantisani, V.; Pergolizzi, S.; D’Angelo, T.; Stagno, A.; Maimone, S.; Squadrito, G.; et al. Dual-energy CT quantification of fractional extracellular space in cirrhotic patients: Comparison between early and delayed equilibrium phases and correlation with oesophageal varices. Radiol. Med. 2021, 126, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Darras, K.E.; Clark, S.J.; Kang, H.; Mohammed, M.F.; Barrett, S.; Chang, S.D.; Harris, A.C.; Nicolaou, S.; McLaughlin, P.D. Virtual monoenergetic reconstruction of contrast-enhanced CT scans of the abdomen and pelvis at 40 keV improves the detection of peritoneal metastatic deposits. Abdom. Radiol. 2019, 44, 422–428. [Google Scholar] [CrossRef]
- Rampado, O.; Depaoli, A.; Marchisio, F.; Gatti, M.; Racine, D.; Ruggeri, V.; Ruggirello, I.; Darvizeh, F.; Fonio, P.; Ropolo, R. Effects of different levels of CT iterative reconstruction on low-contrast detectability and radiation dose in patients of different sizes: An anthropomorphic phantom study. Radiol. Med. 2021, 126, 55–62. [Google Scholar] [CrossRef]
- Fusco, R.; Setola, S.V.; Raiano, N.; Granata, V.; Cerciello, V.; Pecori, B.; Petrillo, A. Analysis of a monocentric computed tomography dosimetric database using a radiation dose index monitoring software: Dose levels and alerts before and after the implementation of the adaptive statistical iterative reconstruction on CT images. Radiol. Med. 2022, 127, 733–742. [Google Scholar] [CrossRef]
- Chua, T.C.; Al-Zahrani, A.; Saxena, A.; Glenn, D.; Liauw, W.; Zhao, J.; Morris, D.L. Determining the association between preoperative computed tomography findings and postoperative outcomes after cytoreductive surgery and perioperative intraperitoneal chemotherapy for pseudomyxoma peritonei. Ann. Surg. Oncol. 2011, 18, 1582–1589. [Google Scholar] [CrossRef]
- Koh, J.L.; Yan, T.D.; Glenn, D.; Morris, D.L. Evaluation of preoperative computed tomography in estimating peritoneal cancer index in colorectal peritoneal carcinomatosis. Ann. Surg. Oncol. 2009, 16, 327–333. [Google Scholar] [CrossRef]
- Yang, L.; Sun, J.; Li, J.; Peng, Y. Dual-energy spectral CT imaging of pulmonary embolism with Mycoplasma pneumoniae pneumonia in children. Radiol. Med. 2022, 127, 154–161. [Google Scholar] [CrossRef]
- Nakamura, Y.; Higaki, T.; Honda, Y.; Tatsugami, F.; Tani, C.; Fukumoto, W.; Narita, K.; Kondo, S.; Akagi, M.; Awai, K. Advanced CT techniques for assessing hepatocellular carcinoma. Radiol. Med. 2021, 126, 925–935. [Google Scholar] [CrossRef]
- Zhang, Y.; Yu, J. The role of MRI in the diagnosis and treatment of gastric cancer. Diagn. Interv. Radiol. 2020, 26, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Terrier, F.; Schuknecht, B.; Fretz, C.; Vock, P.; Herschkowitz, N. Magnetic resonance in oncology. Schweiz. Med. Wochenschr. 1990, 120, 1257–1272. [Google Scholar]
- Low, R.N. MR imaging of the peritoneal spread of malignancy. Abdom. Imaging 2007, 32, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Low, R.N. Magnetic resonance imaging of the abdomen: Applications in the oncology patient. Oncology 2000, 14, 5–14. [Google Scholar] [PubMed]
- Low, R.N.; Barone, R.M.; Rousset, P. Peritoneal MRI in patients undergoing cytoreductive surgery and HIPEC: History, clinical applications, and implementation. Eur. J. Surg. Oncol. 2021, 47, 65–74. [Google Scholar] [CrossRef]
- Cappabianca, S.; Granata, V.; Di Grezia, G.; Mandato, Y.; Reginelli, A.; Di Mizio, V.; Grassi, R.; Rotondo, A. The role of nasoenteric intubation in the MR study of patients with Crohn’s disease: Our experience and literature review. Radiol. Med. 2011, 116, 389–406. [Google Scholar] [CrossRef]
- van’t Sant, I.; van Eden, W.J.; Engbersen, M.P.; Kok, N.F.M.; Woensdregt, K.; Lambregts, D.M.J.; Shanmuganathan, S.; Beets-Tan, R.G.H.; Aalbers, A.G.J.; Lahaye, M.J. Diffusion-weighted MRI assessment of the peritoneal cancer index before cytoreductive surgery. Br. J. Surg. 2018, 106, 491–498. [Google Scholar] [CrossRef]
- Low, R.N.; Barone, R.M.; Gurney, J.M.; Muller, W.D. Mucinous appendiceal neoplasms: Preoperative MR staging and classification compared with surgical and histopathologic findings. Am. J. Roentgenol. 2008, 190, 656–665. [Google Scholar] [CrossRef] [Green Version]
- Ricke, J.; Sehouli, J.; Hach, C.; Hänninen, E.L.; Lichtenegger, W.; Felix, R. Prospective evaluation of contrast-enhanced MRI in the depiction of peritoneal spread in primary or recurrent ovarian cancer. Eur. Radiol. 2003, 13, 943–949. [Google Scholar] [CrossRef]
- Low, R.N.; Gurney, J. Diffusion-weighted MRI (DWI) in the oncology patient: Value of breathhold DWI compared to unenhanced and gadolinium-enhanced MRI. J. Magn. Reson. Imaging 2007, 25, 848–858. [Google Scholar] [CrossRef] [PubMed]
- Gitto, S.; Bologna, M.; Corino, V.D.A.; Emili, I.; Albano, D.; Messina, C.; Armiraglio, E.; Parafioriti, A.; Luzzati, A.; Mainardi, L.; et al. Diffusion-weighted MRI radiomics of spine bone tumors: Feature stability and machine learning-based classification performance. Radiol. Med. 2022, 127, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Bicchetti, M.; Simone, G.; Giannarini, G.; Girometti, R.; Briganti, A.; Brunocilla, E.; Cardone, G.; De Cobelli, F.; Gaudiano, C.; Del Giudice, F.; et al. A novel pathway to detect muscle-invasive bladder cancer based on integrated clinical features and VI-RADS score on MRI: Results of a prospective multicenter study. Radiol. Med. 2022, 127, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Cipollari, S.; Pecoraro, M.; Forookhi, A.; Laschena, L.; Bicchetti, M.; Messina, E.; Lucciola, S.; Catalano, C.; Panebianco, V. Biparametric prostate MRI: Impact of a deep learning-based software and of quantitative ADC values on the inter-reader agreement of experienced and inexperienced readers. Radiol. Med. 2022, 127, 1245–1253. [Google Scholar] [CrossRef] [PubMed]
- Bruno, F.; Marrelli, A.; Tommasino, E.; Martinese, G.; Gagliardi, A.; Pertici, L.; Pagliei, V.; Palumbo, P.; Arrigoni, F.; Di Cesare, E.; et al. Advanced MRI imaging of nerve roots in lumbar radiculopathy due to discoradicular conflict: DWI, DTI, and T2 mapping with clinical and neurophysiological correlations. Radiol. Med. 2022, 127, 1270–1276. [Google Scholar] [CrossRef]
- Scaglione, M.; Basilico, R.; Delli Pizzi, A.; Iacobellis, F.; Dick, E.; Wirth, S.; Linsenmaier, U.; Calli, C.; Berger, F.H.; Nieboer, K.H.; et al. Correction to: The practice of emergency radiology throughout Europe: A survey from the European Society of Emergency Radiology on volume, staffing, equipment, and scheduling. Eur. Radiol. 2021, 31, 4407–4408. [Google Scholar] [CrossRef]
- Michielsen, K.; Vergote, I.; Op de Beeck, K.; Amant, F.; Leunen, K.; Moerman, P.; Deroose, C.; Souverijns, G.; Dymarkowski, S.; De Keyzer, F.; et al. Whole-body MRI with diffusion-weighted sequence for staging of patients with suspected ovarian cancer: A clinical feasibility study in comparison to CT and FDG-PET/CT. Eur. Radiol. 2014, 24, 889–901. [Google Scholar] [CrossRef]
- Wang, Y.; Yu, Y.; Han, W.; Zhang, Y.J.; Jiang, L.; Xue, H.D.; Lei, J.; Jin, Z.Y.; Yu, J.C. CT Radiomics for Distinction of Human Epidermal Growth Factor Receptor 2 Negative Gastric Cancer. Acad. Radiol. 2021, 28, e86–e92. [Google Scholar] [CrossRef]
- Yu, X.Y.; Ren, J.; Jia, Y.; Wu, H.; Niu, G.; Liu, A.; Gao, Y.; Hao, F.; Xie, L. Multiparameter MRI Radiomics Model Predicts Preoperative Peritoneal Carcinomatosis in Ovarian Cancer. Front. Oncol. 2021, 11, 765652. [Google Scholar] [CrossRef]
- Bordonaro, V.; Ciancarella, P.; Ciliberti, P.; Curione, D.; Napolitano, C.; Santangelo, T.P.; Natali, G.L.; Rollo, M.; Guccione, P.; Pasquini, L.; et al. Dynamic contrast-enhanced magnetic resonance lymphangiography in pediatric patients with central lymphatic system disorders. Radiol. Med. 2021, 126, 737–743. [Google Scholar] [CrossRef]
- Klumpp, B.D.; Aschoff, P.; Schwenzer, N.; Fenchel, M.; Koenigsrainer, I.; Falch, C.; Bruecher, B.; Claussen, C.D.; Koenigsrainer, A.; Pfannenberg, C.; et al. Peritoneal carcinomatosis: Comparison of dynamic contrast-enhanced magnetic resonance imaging with surgical and histopathologic findings. Abdom. Imaging 2012, 37, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Torkzad, M.R.; Casta, N.; Bergman, A.; Ahlström, H.; Påhlman, L.; Mahteme, H. Comparison between MRI and CT in prediction of peritoneal carcinomatosis index (PCI) in patients undergoing cytoreductive surgery in relation to the experience of the radiologist. J. Surg. Oncol. 2015, 111, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, M.; van der Pol, C.B.; Patlas, M.N.; Udare, A.; Chung, A.D.; Rubino, J. Optimizing the radiologist work environment: Actionable tips to improve workplace satisfaction, efficiency, and minimize burnout. Radiol. Med. 2021, 126, 1255–1257. [Google Scholar] [CrossRef] [PubMed]
- Scialpi, M.; Moschini, T.O.; De Filippis, G. PET/contrast-enhanced CT in oncology: “To do, or not to do, that is the question”. Radiol. Med. 2022, 127, 925–927. [Google Scholar] [CrossRef]
- Sala, E.; Kataoka, M.; Pandit-Taskar, N.; Ishill, N.; Mironov, S.; Moskowitz, C.S.; Mironov, O.; Collins, M.A.; Chi, D.S.; Larson, S.; et al. Recurrent ovarian cancer: Use of contrast-enhanced CT and PET/CT to accurately localize tumor recurrence and to predict patients’ survival. Radiology 2010, 257, 125–134. [Google Scholar] [CrossRef] [Green Version]
- Granata, V.; Fusco, R.; De Muzio, F.; Cutolo, C.; Setola, S.V.; Dell’Aversana, F.; Grassi, F.; Belli, A.; Silvestro, L.; Ottaiano, A.; et al. Radiomics and machine learning analysis based on magnetic resonance imaging in the assessment of liver mucinous colorectal metastases. Radiol. Med. 2022, 127, 763–772. [Google Scholar] [CrossRef]
- Dromain, C.; Leboulleux, S.; Auperin, A.; Goere, D.; Malka, D.; Lumbroso, J.; Schumberger, M.; Sigal, R.; Elias, D. Staging of peritoneal carcinomatosis: Enhanced CT vs. PET/CT. Abdom. Imaging 2008, 33, 87–93. [Google Scholar] [CrossRef]
- Klumpp, B.D.; Schwenzer, N.; Aschoff, P.; Miller, S.; Kramer, U.; Claussen, C.D.; Bruecher, B.; Koenigsrainer, A.; Pfannenberg, C. Preoperative assessment of peritoneal carcinomatosis: Intraindividual comparison of 18F-FDG PET/CT and MRI. Abdom. Imaging 2013, 38, 64–71. [Google Scholar] [CrossRef]
- Hugen, N.; van de Velde, C.J.H.; de Wilt, J.H.W.; Nagtegaal, I.D. Metastatic pattern in colorectal cancer is strongly influenced by histological subtype. Ann. Oncol. 2014, 25, 651–657. [Google Scholar] [CrossRef]
- Audollent, R.; Eveno, C.; Dohan, A.; Sarda, L.; Jouvin, I.; Soyer, P.; Pocard, M. Pitfalls and mimickers on (18)F-FDG-PET/CT in peritoneal carcinomatosis from colorectal cancer: An analysis from 37 patients. J. Visc. Surg. 2015, 152, 285–291. [Google Scholar] [CrossRef]
- Levy, A.D.; Shaw, J.C.; Sobin, L.H. Secondary tumors and tumorlike lesions of the peritoneal cavity: Imaging features with pathologic correlation. Radiographics 2009, 29, 347–373. [Google Scholar] [CrossRef] [PubMed]
- Foti, G.; Lombardo, F.; Guerriero, M.; Rodella, T.; Cicciò, C.; Faccioli, N.; Serra, G.; Manenti, G. Management of vertebral compression fractures: The role of dual-energy CT in clinical practice. Radiol. Med. 2022, 127, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Ganesh, H.; DiSantis, D.J. Omental cake. Abdom. Radiol. 2016, 41, 2080–2081. [Google Scholar] [CrossRef]
- Walkey, M.M.; Friedman, A.C.; Sohotra, P.; Radecki, P.D. CT manifestations of peritoneal carcinomatosis. Am. J. Roentgenol. 1988, 150, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- Pannu, H.K.; Bristow, R.E.; Montz, F.J.; Fishman, E.K. Multidetector CT of peritoneal carcinomatosis from ovarian cancer. Radiographics 2003, 23, 687–701. [Google Scholar] [CrossRef]
- Amendola, M.A. The role of CT in the evaluation of ovarian malignancy. Crit. Rev. Diagn. Imaging 1985, 24, 329–368. [Google Scholar] [PubMed]
- Meyers, M.A. Distribution of intra-abdominal malignant seeding: Dependency on dynamics of flow of ascitic fluid. Am. J. Roentgenol. Radium Ther. Nucl. Med. 1973, 119, 198–206. [Google Scholar] [CrossRef] [Green Version]
- Tsuyoshi, H.; Inoue, D.; Kurokawa, T.; Yoshida, Y. Hyperthermic intraperitoneal chemotherapy (HIPEC) for gynecological cancer. J. Obstet. Gynaecol. Res. 2020, 46, 1661–1671. [Google Scholar] [CrossRef]
- McMullen, J.R.W.; Selleck, M.; Wall, N.R.; Senthil, M. Peritoneal carcinomatosis: Limits of diagnosis and the case for liquid biopsy. Oncotarget 2017, 8, 43481–43490. [Google Scholar] [CrossRef] [Green Version]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Tixier, F.; Le Rest, C.C.; Hatt, M.; Albarghach, N.; Pradier, O.; Metges, J.P.; Corcos, L.; Visvikis, D. Intratumor heterogeneity characterized by textural features on baseline 18F-FDG PET images predicts response to concomitant radiochemotherapy in esophageal cancer. J. Nucl. Med. 2011, 52, 369–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosmans, J.M.; Neri, E.; Ratib, O.; Kahn, C.E., Jr. Structured reporting: A fusion reactor hungry for fuel. Insights Imaging 2015, 6, 129–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roviello, F.; Pinto, E.; Corso, G.; Pedrazzani, C.; Caruso, S.; Filippeschi, M.; Petrioli, R.; Marsili, S.; Mazzei, M.A.; Marrelli, D. Safety and potential benefit of hyperthermic intraperitoneal chemotherapy (HIPEC) in peritoneal carcinomatosis from primary or recurrent ovarian cancer. J. Surg. Oncol. 2010, 102, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Ueno, Y.; Forghani, B.; Forghani, R.; Dohan, A.; Zeng, X.Z.; Chamming’s, F.; Arseneau, J.; Fu, L.; Gilbert, L.; Gallix, B.; et al. Endometrial Carcinoma: MR Imaging-based Texture Model for Preoperative Risk Stratification-A Preliminary Analysis. Radiology 2017, 284, 748–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giurazza, F.; Corvino, F.; Silvestre, M.; Cangiano, G.; De Magistris, G.; Cavaglià, E.; Amodio, F.; Niola, R. Embolization of peripheral arteriovenous malformations and fistulas with precipitating hydrophobic injectable liquid (PHIL(®)). Radiol. Med. 2021, 126, 474–483. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, J.Q.; Liu, J.L.; Tian, L. Issues on peritoneal metastasis of gastric cancer: An update. World J. Surg. Oncol. 2019, 17, 215. [Google Scholar] [CrossRef] [Green Version]
- Aherne, E.A.; Fenlon, H.M.; Shields, C.J.; Mulsow, J.J.; Cronin, C.G. What the Radiologist Should Know About Treatment of Peritoneal Malignancy. Am. J. Roentgenol. 2017, 208, 531–543. [Google Scholar] [CrossRef]
- Chua, T.C.; Moran, B.J.; Sugarbaker, P.H.; Levine, E.A.; Glehen, O.; Gilly, F.N.; Baratti, D.; Deraco, M.; Elias, D.; Sardi, A.; et al. Early- and long-term outcome data of patients with pseudomyxoma peritonei from appendiceal origin treated by a strategy of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. J. Clin. Oncol. 2012, 30, 2449–2456. [Google Scholar] [CrossRef] [Green Version]
- Coccolini, F.; Gheza, F.; Lotti, M.; Virzì, S.; Iusco, D.; Ghermandi, C.; Melotti, R.; Baiocchi, G.; Giulini, S.M.; Ansaloni, L.; et al. Peritoneal carcinomatosis. World J. Gastroenterol. 2013, 19, 6979–6994. [Google Scholar] [CrossRef]
- Heiss, M.M.; Murawa, P.; Koralewski, P.; Kutarska, E.; Kolesnik, O.O.; Ivanchenko, V.V.; Dudnichenko, A.S.; Aleknaviciene, B.; Razbadauskas, A.; Gore, M.; et al. The trifunctional antibody catumaxomab for the treatment of malignant ascites due to epithelial cancer: Results of a prospective randomized phase II/III trial. Int. J. Cancer 2010, 127, 2209–2221. [Google Scholar] [CrossRef] [Green Version]
- Di Giuliano, F.; Minosse, S.; Picchi, E.; Ferrazzoli, V.; Da Ros, V.; Muto, M.; Pistolese, C.A.; Garaci, F.; Floris, R. Qualitative and quantitative analysis of 3D T1 Silent imaging. Radiol. Med. 2021, 126, 1207–1215. [Google Scholar] [CrossRef]
- Low, R.N.; Semelka, R.C.; Worawattanakul, S.; Alzate, G.D. Extrahepatic abdominal imaging in patients with malignancy: Comparison of MR imaging and helical CT in 164 patients. J. Magn. Reson. Imaging 2000, 12, 269–277. [Google Scholar] [CrossRef]
- Sugarbaker, P.H. Managing the peritoneal surface component of gastrointestinal cancer. Part 2. Perioperative intraperitoneal chemotherapy. Oncology 2004, 18, 207–219, discussion 220–202, 227–208, 230. [Google Scholar]
- Cotton, F.; Pellet, O.; Gilly, F.N.; Granier, A.; Sournac, L.; Glehen, O. MRI evaluation of bulky tumor masses in the mesentery and bladder involvement in peritoneal carcinomatosis. Eur. J. Surg. Oncol. 2006, 32, 1212–1216. [Google Scholar] [CrossRef]
- Mazzola, R.; Cuccia, F.; Figlia, V.; Rigo, M.; Nicosia, L.; Giaj-Levra, N.; Ricchetti, F.; Vitale, C.; Mantoan, B.; Di Paola, G.; et al. Stereotactic body radiotherapy for oligometastatic castration sensitive prostate cancer using 1.5 T MRI-Linac: Preliminary data on feasibility and acute patient-reported outcomes. Radiol. Med. 2021, 126, 989–997. [Google Scholar] [CrossRef] [PubMed]
- Ganeshan, D.; Duong, P.T.; Probyn, L.; Lenchik, L.; McArthur, T.A.; Retrouvey, M.; Ghobadi, E.H.; Desouches, S.L.; Pastel, D.; Francis, I.R. Structured Reporting in Radiology. Acad. Radiol. 2018, 25, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Levy, A.D.; Arnáiz, J.; Shaw, J.C.; Sobin, L.H. From the archives of the AFIP: Primary peritoneal tumors: Imaging features with pathologic correlation. Radiographics 2008, 28, 583–607, quiz 582–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussein, M.A.M.; Cafarelli, F.P.; Paparella, M.T.; Rennie, W.J.; Guglielmi, G. Phosphaturic mesenchymal tumors: Radiological aspects and suggested imaging pathway. Radiol. Med. 2021, 126, 1609–1618. [Google Scholar] [CrossRef]
- Attanoos, R.L.; Gibbs, A.R. Pathology of malignant mesothelioma. Histopathology 1997, 30, 403–418. [Google Scholar] [CrossRef]
- Roggli, V.L.; Sharma, A.; Butnor, K.J.; Sporn, T.; Vollmer, R.T. Malignant mesothelioma and occupational exposure to asbestos: A clinicopathological correlation of 1445 cases. Ultrastruct. Pathol. 2002, 26, 55–65. [Google Scholar] [CrossRef]
- Guest, P.J.; Reznek, R.H.; Selleslag, D.; Geraghty, R.; Slevin, M. Peritoneal mesothelioma: The role of computed tomography in diagnosis and follow up. Clin. Radiol. 1992, 45, 79–84. [Google Scholar] [CrossRef]
- Jeong, Y.J.; Kim, S.; Kwak, S.W.; Lee, N.K.; Lee, J.W.; Kim, K.I.; Choi, K.U.; Jeon, T.Y. Neoplastic and nonneoplastic conditions of serosal membrane origin: CT findings. Radiographics 2008, 28, 801–817, discussion 808–817; quiz 912. [Google Scholar] [CrossRef]
- Puvaneswary, M.; Chen, S.; Proietto, T. Peritoneal mesothelioma: CT and MRI findings. Australas. Radiol. 2002, 46, 91–96. [Google Scholar] [CrossRef]
- Stafford-Johnson, D.B.; Bree, R.L.; Francis, I.R.; Korobkin, M. CT appearance of primary papillary serous carcinoma of the peritoneum. Am. J. Roentgenol. 1998, 171, 687–689. [Google Scholar] [CrossRef]
- Gerald, W.L.; Miller, H.K.; Battifora, H.; Miettinen, M.; Silva, E.G.; Rosai, J. Intra-abdominal desmoplastic small round-cell tumor. Report of 19 cases of a distinctive type of high-grade polyphenotypic malignancy affecting young individuals. Am. J. Surg. Pathol. 1991, 15, 499–513. [Google Scholar] [CrossRef] [PubMed]
- Bellah, R.; Suzuki-Bordalo, L.; Brecher, E.; Ginsberg, J.P.; Maris, J.; Pawel, B.R. Desmoplastic small round cell tumor in the abdomen and pelvis: Report of CT findings in 11 affected children and young adults. AJR. Am. J. Roentgenol. 2005, 184, 1910–1914. [Google Scholar] [CrossRef] [PubMed]
- Pickhardt, P.J.; Fisher, A.J.; Balfe, D.M.; Dehner, L.P.; Huettner, P.C. Desmoplastic small round cell tumor of the abdomen: Radiologic-histopathologic correlation. Radiology 1999, 210, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Deering, S.; Miller, B.; Kopelman, J.N.; Reed, M. Recurrent leiomyomatosis peritonealis disseminata exacerbated by in vitro fertilization. Am. J. Obstet. Gynecol. 2000, 182, 725–726. [Google Scholar] [CrossRef] [PubMed]
- Papadatos, D.; Taourel, P.; Bret, P.M. CT of leiomyomatosis peritonealis disseminata mimicking peritoneal carcinomatosis. Am. J. Roentgenol. 1996, 167, 475–476. [Google Scholar] [CrossRef] [Green Version]
- Fulcher, A.S.; Szucs, R.A. Leiomyomatosis peritonealis disseminata complicated by sarcomatous transformation and ovarian torsion: Presentation of two cases and review of the literature. Abdom. Imaging 1998, 23, 640–644. [Google Scholar] [CrossRef]
- Cho, J.H.; Kim, S.S. Peritoneal Carcinomatosis and Its Mimics: Review of CT Findings for Differential Diagnosis. J. Belg. Soc. Radiol. 2020, 104, 8. [Google Scholar] [CrossRef] [Green Version]
- Yeh, H.C.; Shafir, M.K.; Slater, G.; Meyer, R.J.; Cohen, B.A.; Geller, S.A. Ultrasonography and computed tomography in pseudomyxoma peritonei. Radiology 1984, 153, 507–510. [Google Scholar] [CrossRef]
- Seshul, M.B.; Coulam, C.M. Pseudomyxoma peritonei: Computed tomography and sonography. Am. J. Roentgenol. 1981, 136, 803–806. [Google Scholar] [CrossRef] [PubMed]
- Pai, R.K.; Longacre, T.A. Pseudomyxoma peritonei syndrome: Classification of appendiceal mucinous tumours. Cancer Treat. Res. 2007, 134, 71–107. [Google Scholar] [CrossRef] [PubMed]
- Bechtold, R.E.; Chen, M.Y.; Loggie, B.W.; Jackson, S.L.; Geisinger, K. CT appearance of disseminated peritoneal adenomucinosis. Abdom. Imaging 2001, 26, 406–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pestieau, S.R.; Esquivel, J.; Sugarbaker, P.H. Pleural extension of mucinous tumor in patients with pseudomyxoma peritonei syndrome. Ann. Surg. Oncol. 2000, 7, 199–203. [Google Scholar] [CrossRef]
- Kim, Y.; Cho, O.; Song, S.; Lee, H.; Rhim, H.; Koh, B. Peritoneal lymphomatosis: CT findings. Abdom. Imaging 1998, 23, 87–90. [Google Scholar] [CrossRef]
- Karaosmanoglu, D.; Karcaaltincaba, M.; Oguz, B.; Akata, D.; Ozmen, M.; Akhan, O. CT findings of lymphoma with peritoneal, omental and mesenteric involvement: Peritoneal lymphomatosis. Eur. J. Radiol. 2009, 71, 313–317. [Google Scholar] [CrossRef]
- Haddad, F.S.; Ghossain, A.; Sawaya, E.; Nelson, A.R. Abdominal tuberculosis. Dis. Colon Rectum 1987, 30, 724–735. [Google Scholar] [CrossRef]
- Hulnick, D.H.; Megibow, A.J.; Naidich, D.P.; Hilton, S.; Cho, K.C.; Balthazar, E.J. Abdominal tuberculosis: CT evaluation. Radiology 1985, 157, 199–204. [Google Scholar] [CrossRef]
- Ha, H.K.; Jung, J.I.; Lee, M.S.; Choi, B.G.; Lee, M.G.; Kim, Y.H.; Kim, P.N.; Auh, Y.H. CT differentiation of tuberculous peritonitis and peritoneal carcinomatosis. Am. J. Roentgenol. 1996, 167, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Gurgitano, M.; Angileri, S.A.; Rodà, G.M.; Liguori, A.; Pandolfi, M.; Ierardi, A.M.; Wood, B.J.; Carrafiello, G. Interventional Radiology ex-machina: Impact of Artificial Intelligence on practice. Radiol. Med. 2021, 126, 998–1006. [Google Scholar] [CrossRef]
- Scapicchio, C.; Gabelloni, M.; Barucci, A.; Cioni, D.; Saba, L.; Neri, E. A deep look into radiomics. Radiol. Med. 2021, 126, 1296–1311. [Google Scholar] [CrossRef] [PubMed]
- Schick, U.; Lucia, F.; Dissaux, G.; Visvikis, D.; Badic, B.; Masson, I.; Pradier, O.; Bourbonne, V.; Hatt, M. MRI-derived radiomics: Methodology and clinical applications in the field of pelvic oncology. Br. J. Radiol. 2019, 92, 20190105. [Google Scholar] [CrossRef]
- Sun, Y.; Hu, P.; Wang, J.; Shen, L.; Xia, F.; Qing, G.; Hu, W.; Zhang, Z.; Xin, C.; Peng, W.; et al. Radiomic features of pretreatment MRI could identify T stage in patients with rectal cancer: Preliminary findings. J. Magn. Reson. Imaging 2018. [Google Scholar] [CrossRef] [PubMed]
- Sutton, E.J.; Onishi, N.; Fehr, D.A.; Dashevsky, B.Z.; Sadinski, M.; Pinker, K.; Martinez, D.F.; Brogi, E.; Braunstein, L.; Razavi, P.; et al. A machine learning model that classifies breast cancer pathologic complete response on MRI post-neoadjuvant chemotherapy. Breast Cancer Res. 2020, 22, 57. [Google Scholar] [CrossRef]
- Satake, H.; Ishigaki, S.; Ito, R.; Naganawa, S. Radiomics in breast MRI: Current progress toward clinical application in the era of artificial intelligence. Radiol. Med. 2022, 127, 39–56. [Google Scholar] [CrossRef]
- Gregucci, F.; Fiorentino, A.; Mazzola, R.; Ricchetti, F.; Bonaparte, I.; Surgo, A.; Figlia, V.; Carbonara, R.; Caliandro, M.; Ciliberti, M.P.; et al. Radiomic analysis to predict local response in locally advanced pancreatic cancer treated with stereotactic body radiation therapy. Radiol. Med. 2022, 127, 100–107. [Google Scholar] [CrossRef]
- Reiazi, R.; Abbas, E.; Famiyeh, P.; Rezaie, A.; Kwan, J.Y.Y.; Patel, T.; Bratman, S.V.; Tadic, T.; Liu, F.F.; Haibe-Kains, B. The impact of the variation of imaging parameters on the robustness of Computed Tomography radiomic features: A review. Comput. Biol. Med. 2021, 133, 104400. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Häggström, I.; Szczypiński, P.; Gibbs, P.; Cook, G. Introduction to Radiomics. J. Nucl. Med. 2020, 61, 488–495. [Google Scholar] [CrossRef]
- Karmazanovsky, G.; Gruzdev, I.; Tikhonova, V.; Kondratyev, E.; Revishvili, A. Computed tomography-based radiomics approach in pancreatic tumors characterization. Radiol. Med. 2021, 126, 1388–1395. [Google Scholar] [CrossRef]
- Nardone, V.; Reginelli, A.; Grassi, R.; Boldrini, L.; Vacca, G.; D’Ippolito, E.; Annunziata, S.; Farchione, A.; Belfiore, M.P.; Desideri, I.; et al. Delta radiomics: A systematic review. Radiol. Med. 2021, 126, 1571–1583. [Google Scholar] [CrossRef]
- Gao, W.; Wang, W.; Song, D.; Yang, C.; Zhu, K.; Zeng, M.; Rao, S.X.; Wang, M. A predictive model integrating deep and radiomics features based on gadobenate dimeglumine-enhanced MRI for postoperative early recurrence of hepatocellular carcinoma. Radiol. Med. 2022, 127, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Agazzi, G.M.; Ravanelli, M.; Roca, E.; Medicina, D.; Balzarini, P.; Pessina, C.; Vermi, W.; Berruti, A.; Maroldi, R.; Farina, D. CT texture analysis for prediction of EGFR mutational status and ALK rearrangement in patients with non-small cell lung cancer. Radiol. Med. 2021, 126, 786–794. [Google Scholar] [CrossRef] [PubMed]
- Chiti, G.; Grazzini, G.; Flammia, F.; Matteuzzi, B.; Tortoli, P.; Bettarini, S.; Pasqualini, E.; Granata, V.; Busoni, S.; Messserini, L.; et al. Gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs): A radiomic model to predict tumor grade. Radiol. Med. 2022, 127, 928–938. [Google Scholar] [CrossRef]
- Huang, J.; Chen, Y.; Zhang, Y.; Xie, J.; Liang, Y.; Yuan, W.; Zhou, T.; Gao, R.; Wen, R.; Xia, Y.; et al. Comparison of clinical-computed tomography model with 2D and 3D radiomics models to predict occult peritoneal metastases in advanced gastric cancer. Abdom. Radiol. 2022, 47, 66–75. [Google Scholar] [CrossRef]
- Mirniaharikandehei, S.; Heidari, M.; Danala, G.; Lakshmivarahan, S.; Zheng, B. Applying a random projection algorithm to optimize machine learning model for predicting peritoneal metastasis in gastric cancer patients using CT images. Comput. Methods Programs Biomed. 2021, 200, 105937. [Google Scholar] [CrossRef]
- Zhou, N.; Dou, R.; Zhai, X.; Fang, J.; Wang, J.; Ma, R.; Xu, J.; Cui, B.; Liang, L. Radiomics analysis based on CT’s greater omental caking for predicting pathological grading of pseudomyxoma peritonei. Sci. Rep. 2022, 12, 4401. [Google Scholar] [CrossRef] [PubMed]
- Song, X.L.; Ren, J.L.; Yao, T.Y.; Zhao, D.; Niu, J. Radiomics based on multisequence magnetic resonance imaging for the preoperative prediction of peritoneal metastasis in ovarian cancer. Eur. Radiol. 2021, 31, 8438–8446. [Google Scholar] [CrossRef]
- Kelly, C.J.; Karthikesalingam, A.; Suleyman, M.; Corrado, G.; King, D. Key challenges for delivering clinical impact with artificial intelligence. BMC Med. 2019, 17, 195. [Google Scholar] [CrossRef] [Green Version]
- Saw, S.N.; Ng, K.H. Current challenges of implementing artificial intelligence in medical imaging. Phys. Med. 2022, 100, 12–17. [Google Scholar] [CrossRef] [PubMed]
- van der Lubbe, M.; Vaidyanathan, A.; de Wit, M.; van den Burg, E.L.; Postma, A.A.; Bruintjes, T.D.; Bilderbeek-Beckers, M.A.L.; Dammeijer, P.F.M.; Bossche, S.V.; Van Rompaey, V.; et al. A non-invasive, automated diagnosis of Menière’s disease using radiomics and machine learning on conventional magnetic resonance imaging: A multicentric, case-controlled feasibility study. Radiol. Med. 2022, 127, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Palatresi, D.; Fedeli, F.; Danti, G.; Pasqualini, E.; Castiglione, F.; Messerini, L.; Massi, D.; Bettarini, S.; Tortoli, P.; Busoni, S.; et al. Correlation of CT radiomic features for GISTs with pathological classification and molecular subtypes: Preliminary and monocentric experience. Radiol. Med. 2022, 127, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Masci, G.M.; Ciccarelli, F.; Mattei, F.I.; Grasso, D.; Accarpio, F.; Catalano, C.; Laghi, A.; Sammartino, P.; Iafrate, F. Role of CT texture analysis for predicting peritoneal metastases in patients with gastric cancer. Radiol. Med. 2022, 127, 251–258. [Google Scholar] [CrossRef]
- Han, D.; Yu, N.; Yu, Y.; He, T.; Duan, X. Performance of CT radiomics in predicting the overall survival of patients with stage III clear cell renal carcinoma after radical nephrectomy. Radiol. Med. 2022, 127, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, D.; Bicci, E.; Cavigli, E.; Danti, G.; Bettarini, S.; Tortoli, P.; Mazzoni, L.N.; Busoni, S.; Pradella, S.; Miele, V. Radiomics in pulmonary neuroendocrine tumours (NETs). Radiol. Med. 2022, 127, 609–615. [Google Scholar] [CrossRef]
- Caruso, D.; Polici, M.; Rinzivillo, M.; Zerunian, M.; Nacci, I.; Marasco, M.; Magi, L.; Tarallo, M.; Gargiulo, S.; Iannicelli, E.; et al. CT-based radiomics for prediction of therapeutic response to Everolimus in metastatic neuroendocrine tumors. Radiol. Med. 2022, 127, 691–701. [Google Scholar] [CrossRef]
- Autorino, R.; Gui, B.; Panza, G.; Boldrini, L.; Cusumano, D.; Russo, L.; Nardangeli, A.; Persiani, S.; Campitelli, M.; Ferrandina, G.; et al. Radiomics-based prediction of two-year clinical outcome in locally advanced cervical cancer patients undergoing neoadjuvant chemoradiotherapy. Radiol. Med. 2022, 127, 498–506. [Google Scholar] [CrossRef]
- De Robertis, R.; Geraci, L.; Tomaiuolo, L.; Bortoli, L.; Beleù, A.; Malleo, G.; D’Onofrio, M. Liver metastases in pancreatic ductal adenocarcinoma: A predictive model based on CT texture analysis. Radiol. Med. 2022, 127, 1079–1084. [Google Scholar] [CrossRef]
- Chen, Y.; Xi, W.; Yao, W.; Wang, L.; Xu, Z.; Wels, M.; Yuan, F.; Yan, C.; Zhang, H. Dual-Energy Computed Tomography-Based Radiomics to Predict Peritoneal Metastasis in Gastric Cancer. Front. Oncol. 2021, 11, 659981. [Google Scholar] [CrossRef]
- Pinker, K.; Chin, J.; Melsaether, A.N.; Morris, E.A.; Moy, L. Precision Medicine and Radiogenomics in Breast Cancer: New Approaches toward Diagnosis and Treatment. Radiology 2018, 287, 732–747. [Google Scholar] [CrossRef] [PubMed]
- Neri, E.; Coppola, F.; Miele, V.; Bibbolino, C.; Grassi, R. Artificial intelligence: Who is responsible for the diagnosis? Radiol. Med. 2020, 125, 517–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacEachern, S.J.; Forkert, N.D. Machine learning for precision medicine. Genome 2021, 64, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Vicini, S.; Bortolotto, C.; Rengo, M.; Ballerini, D.; Bellini, D.; Carbone, I.; Preda, L.; Laghi, A.; Coppola, F.; Faggioni, L. A narrative review on current imaging applications of artificial intelligence and radiomics in oncology: Focus on the three most common cancers. Radiol. Med. 2022, 127, 819–836. [Google Scholar] [CrossRef] [PubMed]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Field | Detail | Admitted Values |
|---|---|---|
| Clinical | symptoms | nausea |
| vomiting | ||
| abdominal pain | ||
| other | ||
| laboratory | CEA | |
| CA 19.9 | ||
| other | ||
| Lesions | Number simptoms | numeric value |
| Morphology | round | |
| oval | ||
| other | ||
| Volume | numeric value | |
| Density o intensity | numeric value | |
| Findings | Multifocal nodules | yes/no |
| Infiltrating peritoneal cavity masses | yes/no | |
| Fat stranding | yes/no | |
| Ascitis or free peritoneal fluid liquido peritoneale libero | yes/no | |
| Nodular peritoneal thickening | yes/no | |
| Peritoneal Enhancement | yes/no | |
| Patterns | Micronodular | yes/no |
| Nodular | yes/no | |
| Omental cake | yes/no | |
| Plaque pattern | yes/no | |
| Mass like pattern | yes/no | |
| Theca pattern | yes/no | |
| Areas most affected | Douglas rectum-bladder excavation yes/no | yes/no |
| Right lower quadrant | yes/no | |
| Lower part of the right infracolic space around the root of the mesentery of the small intestine, the sigmoid colon, right paracolic groove | yes/no | |
| Contraindications to cytoreduction | Involvement of the root of the mesentery | yes/no |
| Involvement of the hepatic hilum and hepatoduodenal ligament | yes/no | |
| Pelvis diffusely infiltrated | yes/no | |
| PCI | The Peritoneal Cancer Index (PCI) is a quantitative scoring system that incorporates both the size and distribution of carcinoma implantation in 13 specific regions within the abdomen and pelvis. These regions, numbered 0 to 8, divide the abdomen and pelvis using lines. Additionally, the small intestine is further divided into four regions: regions 9 and 10 represent the upper and lower portions of the jejunum, while regions 11 and 12 represent the upper and lower portions of the ileum. The size of the largest implant, known as the lesion size (LS), is assessed using a scale ranging from 0 to 3 | LS-0 means that there are no plants visible in any of the areas. LS-1 refers to implants that are visible up to 0.5 cm in maximum diameter. LS-2 identifies nodules larger than 0.5 cm and up to 5 cm. LS-3 refers to implants with a diameter of 5 cm or greater. If an organ is extensively covered by tumor or if there are tissue adhesions, the region or site is also evaluated as LS-3. The lesion sizes are then summed for all abdominopelvic regions. A numerical score from 0 to 39 indicates the extent of the disease in all regions. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reginelli, A.; Giacobbe, G.; Del Canto, M.T.; Alessandrella, M.; Balestrucci, G.; Urraro, F.; Russo, G.M.; Gallo, L.; Danti, G.; Frittoli, B.; et al. Peritoneal Carcinosis: What the Radiologist Needs to Know. Diagnostics 2023, 13, 1974. https://doi.org/10.3390/diagnostics13111974
Reginelli A, Giacobbe G, Del Canto MT, Alessandrella M, Balestrucci G, Urraro F, Russo GM, Gallo L, Danti G, Frittoli B, et al. Peritoneal Carcinosis: What the Radiologist Needs to Know. Diagnostics. 2023; 13(11):1974. https://doi.org/10.3390/diagnostics13111974
Chicago/Turabian StyleReginelli, Alfonso, Giuliana Giacobbe, Maria Teresa Del Canto, Marina Alessandrella, Giovanni Balestrucci, Fabrizio Urraro, Gaetano Maria Russo, Luigi Gallo, Ginevra Danti, Barbara Frittoli, and et al. 2023. "Peritoneal Carcinosis: What the Radiologist Needs to Know" Diagnostics 13, no. 11: 1974. https://doi.org/10.3390/diagnostics13111974