The Dynamic Universal Profiles of Spiritual Awareness: A Latent Profile Analysis

Spirituality Mind Body Institute, Teachers College, Columbia University, New York, NY 10027, USA
*
Author to whom correspondence should be addressed.
Religions 2020, 11(6), 288; https://doi.org/10.3390/rel11060288
Submission received: 12 May 2020
/
Revised: 3 June 2020
/
Accepted: 7 June 2020
/
Published: 12 June 2020
(This article belongs to the Special Issue Spiritual Development over the Lifespan)
Abstract
:The aim of the current investigation was to identify universal profiles of lived spirituality. A study on a large sample of participants (N = 5512) across three countries, India, China, and the United States, suggested there are at least five cross-cultural phenotypic dimensions of personal spiritual capacity—spiritual reflection and commitment; contemplative practice; perception of interconnectedness; perception of love; and practice of altruism—that are protective against pathology in a community sample and have been replicated in matched clinical and non-clinical samples. Based on the highest frequency combinations of these five capacities in the same sample, we explored potentially dynamic profiles of spiritual engagement. We inductively derived five profiles using Latent Profile Analysis (LPA): non-seeking; socially disconnected; spiritual emergence; virtuous humanist; and spiritually integrated. We also examined, in this cross-sectional data, covariates external to the LPA model which measure disposition towards meaning across two dimensions: seeking and fulfillment, of which the former necessarily precedes the latter. These meaning covariates, in conjunction with cross-profile age differences, suggest the profiles might represent sequential phases along an emergent path of spiritual development. Subsequent regression analyses conducted to predict depression, anxiety, substance-related disorders, and positive psychology based on spiritual engagement profiles revealed the spiritually integrated profile was most protected against psychopathology, while the spiritual emergence profile was at highest risk. While this developmental process may be riddled with struggle, as evidenced by elevated rates of psychopathology and substance use in the intermediate phases, this period is a transient one that necessarily precedes one of mental wellness and resilience—the spiritual development process is ultimately buoyant and protective.
1. Introduction
A large body of research shows that spirituality functions by and large as a protective factor against various forms of psychopathology—specifically, depressive disorders (Barton et al. 2013; Koenig 2009; Koenig et al. 1998; Miller et al. 2012; Miller et al. 2014; Nelson et al. 2002; Rasic et al. 2011), anxiety disorders (Azhar et al. 1994; Kaplan et al. 2005), and substance-related disorders (Miller and Gur 2002; Harden 2010). A systematic evidence-based review of the past 20 years of research also revealed religious and spiritual involvement predicts lower rates of depression, alcohol and substance abuse, stress-related disorders, and dementia (review by Bonelli and Koenig 2013). Biological markers further confirm the protective benefit of spiritual engagement. For instance, there is strong evidence linking a high level of spirituality with better daily regulation of cortisol, cardiovascular health, and immune functioning (Dedert et al. 2004; Seeman et al. 2003). Spiritual practices have also been purported to reduce arousal in the hypothalamic-pituitary-adrenal axis (HPA) and the sympathetic nervous system (SNS), structures whose hyperactivity has been closely associated with mental illness (Benson 1997; Benson et al. 1974; Chen et al. 2008; Curiati et al. 2005; John et al. 2011; Krygier et al. 2013; Pariante and Lightman 2008; Phongsuphap et al. 2008; Tang et al. 2009; Thayer and Lane 2007; Thoresen 1999; Veith et al. 1994).
A clinical and theoretical literature on spiritual and personality development, however, suggests progress towards individuation—wholeness as an indivisible unit of being—and well-being is not linearly positive, but rather, necessarily replete with struggle—a rite of passage. Carl Jung theorized that before one achieves individuation, one unavoidably ought to encounter darkness and descent. He states, “the confrontation is the first test of courage on the inner way, a test sufficient to frighten off most people, for the meeting with ourselves belongs to the more unpleasant things” (Jung 1968). William James and Abraham Maslow similarly conceptualized personality development as a spiritual process, “gradual or sudden, by which a self hitherto divided becomes unified” (James 1902; Maslow 1999). They also depicted the unavoidable yet necessary phase of struggle in this process. William James, for instance, experienced severe “melancholia” and “neurasthenia,” which were the reported consequences of a “spiritual crisis” (Perry 1935).
This theme of descent preceding spiritual individuation is also prevalent amongst numerous philosophical and religious texts and traditions. Perhaps even before the encounter with darkness, one experiences the distracted, unexamined life—the denial and projection of one’s own darkness. During this phase, the Buddha, due to his father’s overprotection, lived a life of luxury, pleasure, and distraction, and St. Augustine similarly “looked for pleasure, beauty, and truth not in [God] but in [himself] and his other creatures, [which] led instead to pain, confusion, and error” (Augustine 1876). The next phase is the inevitable encounter with darkness, descent, and tribulation that Jung referred to—the cessation of projection and the direct confrontation of one’s own shadow self. Jesus’ temptation of Christ, Buddha’s encounter with Mara under the Bodhi tree, Arjuna’s despair and turmoil, and Muhammad’s opposition and year of sorrow, among many others, illustrate this phase of descent. After the encounter with darkness, the last phase involves the completion of the individuation process—the integration of the shadow self. Through this universal process, the religious traditions and early psychological and philosophical theories suggest one ultimately discovers wholeness in the self, transcendence, and salvation. The alternative pathway involves the one who “never met the dragon, or who, if once he saw it, declared afterwards that he saw nothing”—continuing to live the unexamined life (Jaffé 1986). With this pathway in mind, Carl Jung states, “people will do anything in order to avoid facing their own souls… One does not become enlightened by imagining figures of light, but by making the darkness conscious” (Jung 2014). Despite this earlier emphasis on the development of the self in the context of spiritual growth, however, subsequent modern iterations of developmental theories often neglected this progressive or process-oriented framework, and instead, exclusively examined development in the context of attachment, object relations, self-schemas, or systems (Poll and Smith 2003).
More recently, however, a growing body of literature confirms this earlier insight—developmental psychopathology is often not simply an isolated case of illness but a necessary part of the individuation process (Ghaemi 2006). Recent magnetic resonance imaging (MRI) evidence, for instance, suggests spirituality and depression share a biological substrate—the same brain regions where thicker cortices were associated with importance of religion and spirituality were thinner for those with familial risk of depression (Miller 2013; Miller et al. 2014). This suggests spirituality and suffering may in fact be “two sides of the same coin” (Miller et al. 2014). Young adults considered to be highly spiritual had one-fourth the risk of recurrence of major depression; among young adults with a depressed parent, high spirituality had an even greater protective effect against depression, reducing the risk to one-tenth (Miller et al. 2012). In the same study, highly spiritual young adults were 2.5-times more likely than young adults with lower levels of spirituality to have been depressed in adolescence, strongly suggesting a period of struggle precedes one of well-being for those on a spiritual path (Miller et al. 2012). Moreover, genes for dopamine (DRD2) were associated with both spirituality and an elevated risk for depression, further corroborating a common underlying pathway between spirituality and depression (Anderson et al. 2017). The increasingly well-documented phenomena of spiritual emergence, spiritual emergency, and transpersonal crisis have also discerned conventional mental illness from this struggle-laden stage of healthy spiritual development (Grof and Grof 1986; Nadal et al. 2018; Prevatt and Park 1989; Sinclair et al. 2016; Yonker et al. 2012). These findings confirm the insight of early psychologists and cross-cultural faith traditions alike—developmental pathology is an opportunity for spiritual growth within a normative developmental trajectory. While this body of research has developed considerably, there still is a dearth of empirical evidence in the current literature. To address this, we hope to explore empirically-based profiles of spirituality that might illuminate possible phases of spiritual development.
In addition to findings of spiritual individuation, previous research has shown that a personal spirituality is an innate human faculty, findings which open up the possibility that cross-cultural profiles of spirituality might exist. Genetic epidemiologic twin studies show that 30% of the variance in the strength of personal spirituality is attributed to broad heritability (Kendler et al. 1997). Innate spirituality is independent of personality, with the exception of a small association with openness to experience, which suggests spirituality is a distinctive, independent construct (Francis 1999; Kendler et al. 1999; Piedmont 1999). Moreover, spiritual awareness surges in late adolescence with physical puberty—heritable contribution of spiritual awareness increases by 50% in emerging adulthood compared with middle adolescence (Koenig et al. 2005; Button et al. 2011). Specific single genes linked to neurochemical systems, including Vesicular Monoamine Transporter 2 (VMAT2), Serotonin (5-HT1B and 5-HT2A), Dopamine (DRD2), Oxytocin (OT), and Monoamine Vesicular Transporter (VMAT1), have additionally been associated with a predisposition towards spirituality and spiritual experiences (Anderson et al. 2017; Hamer 2005). While upbringing may impact the manifestation and expression of spirituality, this growing body of literature strongly suggests humans have an inborn propensity towards spiritual awareness and transcendence. These findings led to an additional emerging hypothesis that universal profiles of spirituality across different cultures might exist.
Although the phenotypic dimensions of an innate spiritual capacity—the observable manifestations of spirituality—has recently been derived, the potential dynamic profiles based on these dimensions have not been examined. McClintock et al. (2016) conducted a multi-national cross-sectional study, in which five phenotypic dimensions of universal spiritual experience were inductively derived: love, unifying interconnectedness, altruism, contemplative practice, and spiritual reflection and commitment. To extend this study, we seek to identify the profiles based on these dimensions of spirituality by utilizing a person-centered analysis (Latent Profile Analysis). We hope to discover potential dynamic profiles of innate spiritual awareness across cultures.
Previous research that used person-centered analyses to examine spiritual profiles has identified subgroups representing the overall level of religiosity or spirituality (i.e., high, medium, low) and mainly focused on religion-oriented indicator variables (Klemmack et al. 2007; Nadal et al. 2018; Park et al. 2013; Roh et al. 2014). One study using latent class analysis found that spirituality and positive psychology indicator variables were highly correlated with each other in homogenous subgroups, and both were protective against depressive symptomology (Barton and Miller 2015). However, to date, there has not been an examination of potentially universal profiles of innate spiritual awareness and how they might address stages in the spiritual developmental theory. The present study seeks to fill this important gap using an exploratory mixture modeling method. Based on the universal dimensions of innate spiritual capacity established by McClintock et al. (2016), we utilize a cross-cultural dataset to establish these profiles. Once the exploratory profiles are established, we examine the hypothesis, formulated post-hoc, that profiles represent stages in a dynamic process by examining potential differences in age along with covariates measuring dispositional meaning seeking and meaning fulfillment behavior. Once covariates are established, we examine whether profiles predict clinical outcomes.
2. Materials and Methods
2.1. Participants
From June of 2014 to February of 2015, 5512 participants (41% women, mean age = 29.0 years, age range: 18–75 years) were recruited from the crowdsourcing websites Zhubajie.com and Mturk.com among residents of China (N = 3150), India (N = 863), and the United States (N = 1499). The extensive online questionnaire included a number of spiritual, clinical, and psychological instruments, as well as sociodemographic questions. For the sample living in China, the questionnaire was translated from English to Chinese. Following guidelines from previous international studies (Squires et al. 2013; World Health Organization 2009), a committee of bilingual translators translated, back-translated, and pretested the full survey instrument over several iterations to ensure conceptual equivalence across cultures. The institutional review board of Teachers College, Columbia University, approved the study.
2.2. Measures
2.2.1. Spirituality Measures
For concepts that are broad and not easily defined, maximizing the heterogeneity of indicators optimizes representation of multivariate constructs (Little et al. 1999). As a result, we reviewed the empirical literature on spirituality and religion, and collected more than 150 published self-report measures that have direct relevance to personal spiritual experience, whether as perceptions of reality, transcendent or sacred practices, views, or expressions. After several rounds of qualitative analyses, we narrowed down the pool to 54 previously validated measures based on comprehensiveness and appropriateness for a multi-national and multi-religious sample. Forty such measures showed adequate or better reliability in the current sample (alpha coefficients 0.65–0.97) and were included in the analyses.
The Fetzer Multidimensional Measurement of Religiousness/Spirituality assessed overall spirituality, overall religiosity, private religious/spiritual practices, negative religious coping, forgiveness, daily spiritual experiences, overall religious coping, and religious commitment (Fetzer Institute/National Institute on Aging Working Group 1999). The Intrinsic Religiosity subscale of the Duke University Religion Index assessed intrinsic religiosity and spirituality (Koenig and Büssing 2010). Salience of spiritual beliefs was measured with the Belief Salience Scale (Blaine and Crocker 1995). Mystical experience was measured with the Mysticism Scale (Hood 1975). Compassion was assessed by the Compassion subscale of the Dispositional Positive Emotions Scale (Shiota et al. 2006). Sitting and moving contemplative practice frequency were each assessed by the average number of sessions per month and number of total months of practice. Two items assessed the presence and importance of spiritual role models, and seven items were used to measure spirituality in nature. Positive morality was measured by the Positive Morality subscale of the Prague Spirituality Questionnaire (Rican and Janosova 2010). Spiritual quest was measured by the Quest scale (Batson and Ventis 1982). Religious meaning was measured with the Religious Meaning Scale (Krause 2003). Experiences of ontological, psychological, social, and religious love were assessed by respective subscales within the Sorkin Multidimensional Index of Love Experience (Levin 2000). Spiritual self-discovery, spiritual relations, sense of sacredness, and eco-awareness were assessed by respective dimensions within the Spirituality Scale (Delaney 2005). The Universality, Prayer Fulfillment, and Connectedness subscales of the Spiritual Transcendence Scale assessed a sense of unity in life, contentment with prayer, and connection to others, respectively (Piedmont 1999). The Spiritual Transcendence Index was a measure of spiritual transcendence (Seidlitz et al. 2002). Humanistic engagement, religious engagement, existential engagement, spiritual study and practice, and gratitude and awe were assessed by subscales of the SpREUK-P Questionnaire (Büssing et al. 2005). Self-transcendence was assessed with the Self-Transcendence subscale of the Temperament and Character Inventory (Cloninger 1999). Purpose in life and personal growth were measured by subscales of the Psychological Well-being scale (Ryff 2014).
2.2.2. Psychopathology Measures
Psychiatric symptoms were assessed with the Patient Health Questionnaire (PHQ-9; Kroenke et al. 2001), the General Anxiety Disorder scale (GAD-7; Spitzer et al. 2006), and Monitoring the Future (Johnston 2010). Cut-off scores were then used to dichotomize the variables as clinically significant and non-significant levels. Based on previous studies (Löwe et al. 2008; Manea et al. 2012), major depression was defined as a score of 10 or greater on the PHQ-9, and generalized anxiety was defined as a score of 10 or greater on the GAD-7. Alcohol-related disorder was defined as being “drunk or very high from alcohol” six or more times in the past 30 days, and cannabis-related disorder was defined as using cannabis six or more times in the past 30 days. The Positive Emotion, Engagement, Relationships, Meaning, and Accomplishment (PERMA) positive psychology scale was also initially divided into a high and low groups at the 75th percentile point. After odds ratios were examined, the continuous scales were used as well.
2.3. Statistical Analyses
The raw data were analyzed using SPSS 22.0 (SPSS I 2011) and Mplus 7.0 (Muthén and Muthén 2012). First, a series of inductive Exploratory Factor Analysis (EFA) and cross-validating Exploratory Structural Equation Modeling (ESEM) were conducted. The specific methodology of factor structure creation and factor loadings can be found in the Frontiers in Psychology article by McClintock, Lau, and Miller (McClintock et al. 2016). The factor scores in five continuous dimensions of spirituality (i.e., spiritual reflection and commitment, contemplative practice, unifying interconnectedness, love, and altruism) produced by the ESEM were then used as continuous cluster indicators to conduct a Latent Profile Analysis (LPA). LPA is a form of mixture modeling, which determines the degree to which there are subgroups, or in the present study—phenotypic subtypes—in a heterogeneous sample (Jung and Wickrama 2008; Muthén 2002). In other words, LPA uses a bottom-up, data-driven approach to identify groups of people in a sample based on how they answer survey questions (i.e., grouping people who have similar patterns of behavior, traits, etc.). The following is a practical example of how LPA might be used: we obtain survey data on drinking behavior (e.g., how often do you drink socially, how often do you drink alone, how much does drinking hinder work and relationships), and the LPA identifies several subgroups of alcoholism based on how people answer these questions (alcoholic, social drinker, abstinent). Latent profiles in the present study were derived from the LPA, which represent distinct homogeneous subgroups in the sample. After running an initial LPA without covariates, we found residual variance that was not explained by the model. As a result, we included an overall latent factor as an internal covariate to account for the portion of the variance unexplained by the latent factor. Furthermore, we included country as a covariate in the model to influence the mass probability of belonging to a certain profile. In essence, when determining phenotypic profile classification, the model adjusted for differences in the variables of country and the latent factor of the indicator variables. After a model of best fit was established, we utilized the estimated posterior probabilities of profile membership to conduct a series of multiple linear regression and logistic regression analyses to predict distal outcomes, including rates of depression, anxiety, substance-related disorders, and positive psychology.
The model of best fit was determined by evaluating an increasing number of profiles. This iterative process involved using a different number of profiles in each model to determine best relative model fit. Relative fit for each model was assessed using the Aikaike information criterion (AIC), Bayesian information criterion (BIC), sample-size adjusted Bayesian information criterion (SABIC), Lo-Mendell-Rubin likelihood ratio test (LMR), entropy, bootstrap likelihood ratio test (BLRT), theoretical interpretability, and parsimony. While the criteria for establishing the best fitting model was heavily considered, parsimony and substantive theoretical interpretability were ultimately used in determining the best number of profiles.
Previous literature suggests the BIC performs the best of the information criteria indices, and the BLRT is also a consistent indicator in model fit (Collins et al. 1993; Nylund et al. 2007). BIC is a criterion for model selection, wherein a lower value reflects better comparative fit (Schwarz 1978). In contrast, the BLRT estimates the difference distribution with a significance test, where a significant p-value signifies a superior model fit for k classes compared with k − 1 classes (McLachlan et al. 2019). Other simulation studies have suggested SABIC to be superior than the other information criteria, particularly when utilizing latent profile analysis for qualitative phenotype identification (Yang 1998, 2006). The SABIC replaces the sample size with an adjusted value, whereby drawbacks of the original BIC are mitigated. With the information criteria indices, the model was run with increasing number of profiles until the lowest value was observed. Others have argued that the LMR adjusted likelihood test is another efficacious method in determining model fit (Lo 2005; Lo et al. 2001; Tofighi and Enders 2006). The LMR adjusted likelihood test, similar to the BLRT, is a significance test comparing model fit for k classes with k − 1 classes. With the hypothesis tests (i.e., LMR test, BLRT), models with an increasing number of profiles were run until the p-value was non-significant.
Once the model of best fit was determined, distal outcomes, including depression, anxiety, alcohol-related disorder, cannabis-related disorder, and positive psychology, were predicted using logistic regression analyses. After observing odds ratios, we conducted multiple linear regression analyses to identify more sensitive, clinical effects and to examine variance in the mid-section of the scales. Conditional probabilities for each profile were used as the independent variables in these distal outcome analyses. Upon examining the LPA probability graph and distal outcomes, we noticed that a given profile, regardless of absolute probability values, tended to predict better mental health if the factor score of contemplative practice was relatively less compared with the factor scores of love and altruism, and vice versa. Contemplative practice reflects an individual’s level of meaning seeking (as it is the amount of time spent practicing), while love and altruism reflect an individual’s level of meaning fulfillment (as they are intrinsically rewarding and meaningful). As a result, we hypothesized post hoc that differences in profiles and their relationship to mental health might be related to one’s levels of meaning seeking and meaning fulfillment. To test this hypothesis, we examined the influence of covariates external to the model—specifically, existential engagement, personal growth, and purpose in life—on profile assignment using multinomial logistic regression analyses. Existential engagement represents dispositional meaning seeking behavior, because it measures an effort to gain insight into oneself and the meaning of life. Personal growth and purpose in life, in contrast, reflect meaning fulfillment, because they measure the extents to which one’s potential is being realized and to which one feels there is a deep sense of meaning in one’s life. These external covariates did not adjust for differences when determining phenotypic classification, but rather, predicted profile classification after the latent profile model was established. Because meaning seeking necessarily precedes meaning fulfillment, significant differences in these covariates along with cross-profile age differences may provide evidence for the hypothesis that profiles are stages in a dynamic process of spiritual development.
3. Results
3.1. Sample Characteristics
The included population was religiously diverse across countries (see Table 1). The United States participants identified predominantly as Christian (48.8%), whereas a smaller fraction of the population identified as Buddhist (2.4%), Jewish (1.3%), Muslim (0.8%), and Hindu (0.4%). In China, a large majority of the population identified as Buddhist (33.7%) or Non-Religious (45.0%). Minority religious groups in China identified as Christian (8.7%), Muslim (0.5%), Jewish (0.3%), and Hindu (0.1%). In India, over half the population identified as Hindu (70.7%), with minority denominations comprising of Christian (17.0%), Muslim (8.8%), Jewish (0.1%), and Buddhism (0.1%). A large majority of individuals identified as Atheist or Non-Religious in the United States (39.4%) and China (45.0%). By comparison, only (2.5%) stated the same in India.
In terms of psychiatric outcomes, the United States (M = 6.16, SD = 6.14) exhibited a mild level of depression, while China (M = 9.01, SD = 4.88) and India (M = 9.60, SD = 7.08) exhibited significantly higher levels of depression in the borderline between the mild and moderate ranges. Differences in anxiety levels across countries reflected those of depression—the United States (M = 4.80, SD = 5.27) presented a mild level of anxiety, while China (M = 6.39, SD = 4.28) and India (M = 6.32, SD = 5.60) displayed moderate levels of anxiety. Although research has suggested the rates of clinical diagnosis for mental illness are generally lower for Asian countries, the greatest burden of mental disorders, as defined by the most years of life lost due to the disability, is relatively high in countries such as China and India (Ferrari et al. 2013; World Health Organization 2017). This mismatch in findings may be due to the lower prevalence of mental health professionals per capita, as well as a strong stigma for mental illness in these countries. Our findings in the context of past research suggest there is perhaps a large portion of undiagnosed depression and anxiety in China and India. There were differences between countries on demographic variables (age, sex, socioeconomic status, education, religion) as well.
3.2. Latent Profile Analysis
Latent profile analysis was used to determine five phenotypic subtypes of spirituality. Once the model of best fit was established, we examined whether covariates external to the model—existential engagement, personal growth, and purpose in life—predicted profile membership using multinomial logistic regression. We subsequently examined whether conditional probabilities of profile membership predicted distal outcomes—depression, anxiety, alcohol-related disorder, cannabis-related disorder, and positive psychology—using multiple linear regression and multiple logistic regression analyses (Figure 1).
To determine model of best fit, we ran unconditional LPA models in ascending profile enumeration starting from a one-profile model until each of the LPA statistics (i.e., AIC, BIC, SABIC, LMR, and BLRT) indicated best fitting model. While adjusting for differences in country and latent spirituality, LPA statistics in conjunction with theoretical interpretability suggested a five-profile model as the model of best fit (Table 2). The first non-significant LMR statistic was found in the six-profile model, which suggests the five-profile model (k − 1) was the model of best fit (Lo et al. 2001). The information criteria statistics continued to decrease with ascending profile enumeration, an occurrence which has been commonly cited in studies with a larger sample size (Chih 2014; Grunschel et al. 2013; Kemperman and Timmermans 2006; Zhang et al. 2014). While the information criteria statistics continued to decrease to an uninterpretable number of profiles, prevailing studies that encountered this scenario utilized the LMR test and a scree plot (i.e., inflection point) of the information criteria statistics to determine model of best fit (Chih 2014; Gibson-Nylund and Choi 2018; Nylund et al. 2007; Wilson et al. 2016). The LMR test indicated the first non-significant p-value (p = 0.146) for the six-profile model, suggesting the five-profile model (k − 1) had the best fit. The LMR test tends to be a relatively parsimonious estimate of profile number determination, which prevents model over-interpretation (Graves and Bowers 2018; Tofighi and Enders 2008) Furthermore, scree plots of the AIC, BIC, and SABIC suggest the point of inflection to be present in the six-profile model, which confirms the five-profile model to be the model of best fit. The five-profile model also exhibited a sufficiently high entropy value of 0.78. While the BLRT remained significant to an uninterpretable number of profiles, based on the information criteria statistics, LMR test, entropy value, and consideration of parsimony and substantive theoretical interpretability, the five-profile model best fit this cross-cultural sample.
The five profiles (Figure 2) were named as follows: virtuous humanist, spiritual emergence, socially disconnected, spiritually integrated, and non-seeking. The virtuous humanist profile (profile 1, Figure 3) comprised 14.3% of the sample and exhibited low levels of spiritual reflection and commitment, contemplative practice, and interconnectedness and slightly above average levels of love and altruism. The spiritual emergence profile (profile 2, Figure 4) consisted of 18.4% of the sample and manifested high levels of spiritual reflection and commitment and contemplative practice, average levels of interconnectedness and love, and slightly above average rate of altruism. The socially disconnected profile (profile 3, Figure 5) comprised 8.7% of the sample and exhibited low levels of spiritual reflection and commitment, interconnectedness, and altruism, slightly above average rate of contemplative practice, and a very low rate of love. The spiritually integrated profile (profile 4, Figure 6) consisted of 15.1% of the sample and displayed a very high rate of spiritual reflection and commitment, slightly above average levels of contemplative practice and interconnectedness, and high levels of love and altruism. The non-seeking profile (profile 5, Figure 7) consisted of 43.6% of the sample and reflected those slightly below average on spiritual reflection and commitment, contemplative practice, and altruism, average on love, and slightly above average on interconnectedness.
A one-way ANOVA was first conducted to examine potential differences in age between profiles. The analysis revealed significant differences in age between profiles (F(4 5403) = 217.95, p < 0.001). LSD post hoc tests further suggested significant differences in age between each profile except between the spiritual emergence and the socially disconnected profiles (Table 3). The spiritually integrated profile was oldest (M = 35.14), followed by the virtuous humanist profile (M = 31.22), the spiritual emergence profile (M = 29.50), the socially disconnected profile (M = 28.97), and the non-seeking profile (M = 25.83).
3.3. Regression Analyses
We then conducted a series of multinomial logistic regression analyses to examine the influence of external covariates—existential engagement, personal growth, and purpose in life—in predicting profile assignment. The logistic regression analyses revealed existential engagement, personal growth, and purpose in life all significantly predicted profile assignment ((4) = 708.94, p < 0.001; (4) = 158.53, p < 0.001; (4) = 983.27, p < 0.001). Post hoc analyses were conducted by running a regression analysis for each of the profiles as the reference category (Table 4). They revealed those with higher levels of existential engagement and lower levels of personal growth and purpose in life were more likely to be in the spiritual emergence profile. Participants with higher levels of personal growth and purpose in life were more likely to be in the spiritually integrated profile. Those with lower levels of existential engagement were more likely to be in the virtuous humanist profile as well.
A series of logistic regression analyses were conducted to examine whether profile assignment probabilities predicted distal outcomes, specifically, depression, anxiety, alcohol-related disorder, cannabis-related disorder, and positive psychology. Controlling for country, the profiles significantly predicted each of the distal outcome measures ((6) = 211.65, p < 0.001; (6) = 142.40, p < 0.001; (6) = 182.59, p < 0.001; (6) = 196.81, p < 0.001; (6) = 455.65, p < 0.001). Furthermore, there were significant differences between profiles (Table 5). The spiritually integrated and virtuous humanist profiles were most protected from depression, while the spiritual emergence profile was at highest risk. The spiritually integrated, virtuous humanist, and non-seeking profiles were protected from anxiety, while the spiritual emergence profile exhibited the highest risk. Moreover, the spiritually integrated profile and the non-seeking profiles were most protected against alcohol-related disorder, while the spiritually integrated profile alone was most protected against cannabis-related disorder. The spiritual emergence profile exhibited the highest levels of risk for both substance-related disorders.
In order to examine variance in the mid-section of the measures, we subsequently conducted a series of multiple linear regression analyses. As the substance disorder measures were obtained as binary scales, they were excluded from these analyses. The conditional probabilities of the profiles significantly predicted depression, anxiety, and positive psychology (F(4 5325) = 82.75, p < 0.001; F(4 5341) = 45.09, p < 0.001; F(4 5014) = 122.28, p < 0.001). Moreover, the conditional probability of each profile differed from one another in predicting rate of depression (Table 6; Figure 8). Those who had a higher conditional probability of belonging to the spiritually integrated profile had significantly reduced risk of depression and greater rate of positive psychology compared with all other profiles. Those who had a higher conditional probability of belonging to the spiritually integrated and the virtuous humanist profiles exhibited reduced risk of anxiety compared with other profiles. In contrast, those more likely to be in the spiritual emergence profile displayed a dichotomy in mental health outcomes—the highest rates of depression and anxiety and second to highest rate of positive psychology. A summary of the profiles is displayed in Figure 9.
4. Discussion
The present study sought to identify potentially dynamic universal profiles of spiritual capacity in a multinational dataset with participants from China, India, and the United States. Using a person-centered analytic method—latent profile analysis—we found five distinct cross-cultural profiles: non-seeking; socially disconnected; spiritual emergence; virtuous humanist; and spiritually integrated. A one-way ANOVA indicated significant age differences between profiles. While the present study was cross-sectional, differences in age and corresponding differences in meaning seeking and meaning fulfillment covariates—existential engagement, personal growth, and purpose in life—strongly suggest the profiles may be dynamic stages in an emergent path, as dispositional meaning seeking behavior necessarily precedes meaning fulfillment. Specifically, higher levels of existential engagement along with lower levels of personal growth and purpose in life increased odds of belonging to the spiritual emergence profile. In contrast, higher rates of personal growth and purpose in life increased odds of belonging to the spiritually integrated profile. A lower level of existential engagement increased odds of belonging to the virtuous humanist profile. The conditional probabilities of the profiles significantly predicted three distal outcomes—depression, anxiety, and positive psychology; profile assignment also predicted cannabis and alcohol dependence. Participants more likely to belong in the spiritually integrated profile exhibited the lowest rate of depression, cannabis dependence, and alcohol dependence, along with the highest rate of positive psychology. Those more likely to be in the spiritually integrated and virtuous humanist profiles exhibited the lowest rates of anxiety. The spiritual emergence profile, however, predicted the highest rate of depression, anxiety, and substance dependence. Compared to the spiritually integrated profile, the spiritual emergence profile was 14 times more likely to be dependent on alcohol and nearly 20 times more likely to be dependent on cannabis. We therefore propose the five profiles as stages in the developmental process of spirituality in young adults; these stages offer a partial explanation into the mechanism of developmental psychopathology.
We propose the emergent path begins with the non-seeking profile. Our results suggest this profile is the youngest (M = 25.83), with slightly below average levels of spiritual reflection and commitment, contemplative practice, and altruism, an average level of love, and a slightly above average level of interconnectedness. Those in this profile likely have not reflected significantly on existential or spiritual matters. Their slightly above average rate of interconnectedness may reflect the relatively recent trend of younger adults to explore spirituality via “ecospirituality”—spirituality in nature—relationally, or communally outside of religion (Harris and Moran 1998; Tacey 2003). This hypothesis is supported by the religious demographic of the non-seeking profile, which consisted mostly of atheist, non-religious, or Buddhist participants. Covariates revealed the non-seeking profile has a lower rate of meaning seeking (i.e., existential engagement) and average rates of meaning fulfillment (i.e., personal growth and purpose in life), which suggest a dearth of existential reflection. Those in the non-seeking profile exhibited relatively high levels of depression and anxiety, along with a low level of positive psychology. Indeed, Socrates proclaimed, “the unexamined life is not worth living” (West and Platon 1979). The non-seeking profile therefore likely mirrors the beginning of the individuative-reflective stage in Fowler’s stages of faith, wherein the young adult begins to question and starts to become disenchanted with one’s old belief system (Fowler and Levin 1984).
Once those in the non-seeking profile begin to explore and question their spirituality, they progress into the second stage of the developmental process—either the spiritual emergence or the socially disengaged profile. Both profiles are slightly older (M = 29.5; M = 29.0, respectively). While the spiritual emergence profile exhibited very high levels of spiritual reflection and commitment and contemplative practice, average levels of interconnectedness and love, and slightly above average levels of altruism, the socially disengaged profile exhibited low levels of spiritual reflection and commitment, interconnectedness, and altruism, slightly above average rate of contemplative practice, and a very low rate of love. While both profiles differ in these ways, they uniquely share significantly higher rates of contemplative practice relative to rates of love and altruism, a distinction which might suggest an effort-reward imbalance.
Those in the spiritual emergence profile embody Carl Jung’s description of the shadow self, St. John of the Cross’ dark night of the soul, and the Book of Jonah’s belly of the whale alike (Campbell 2008; Jung 1963; Starr 2003). While those in this profile are in desperate search for meaning and transcendence, as evidenced by very high levels of spiritual reflection and commitment and contemplative practice, the fruits of their spiritual efforts—love and altruism—lag behind. The covariates support this hypothesis: this profile exhibited the highest level of existential engagement but also the lowest levels of personal growth and purpose in life. While they desperately reflect on their existence and spirituality, they lack a sense of progress or clear meaning. This drastic increase in meaning-seeking behavior relative to the non-seeking profile, along with the fact that the spiritual emergence profile is significantly older, may suggest a dynamic shift in profile assignment. This descent has not only been widely cited in the scientific literature but also been taught by a multitude of religious and spiritual traditions for millennia as a necessary and normative step in the developmental path of spirituality (Durà-Vilà and Dein 2009; Grof and Grof 1986; Miller 2013; O’Connor 2002). For instance, after witnessing the “four sights”, the Buddha, at the age of 29, embarks on the spiritual path, which is fraught with suffering, before attaining enlightenment at the age of 35. Even after many trials and tribulations, the Buddha is continuously tested by Mara, the demonic king hoping to prevent the Buddha from attaining enlightenment. Upon facing this inevitable challenge by Mara, the Buddha claims, “none but the brave will conquer them to gain bliss by the victory… Better I die in battle now than choose to live on in defeat” (Guruge 1997). After going through this period of descent, the Buddha ultimately finds enlightenment. Similarly, before his baptism, Jesus endures the “temptation of Christ”, where he confronts trials and temptation by the devil. “After fasting forty days and forty nights, [Jesus] was hungry,” and after a series of temptations, “the devil left him, and angels came and attended him” (Bible 1984). Joseph Campbell described this process when he affirmed, “the dark night of the soul comes just before revelation… when everything is lost, and all seems darkness, then comes the new life and all that is needed” (Campbell 2011).
This process of descent has been cited in the scientific literature as well. Novice spiritual or meditation practitioners often experience a heightened sense of anxiety, depression, or distress due either to the meditation technique, over-meditation, or rise of repressed trauma into conscious awareness (Compson 2014; Engler 1984; Epstein 1990; Lazarus 1976; Michalon 2001; Otis 1973). Those in the spiritual emergence profile consequently exhibited clinically significant levels of psychopathology in our sample—the highest of all profiles. Their high rates of substance dependence may especially reflect a deep-set desire for self-transcendence (Burris et al. 2011; Martinotti et al. 2006). Simultaneously, they displayed a high rate of positive psychology, which suggests presence of positive emotions and engagement with life—phenomenology not typically found in depressive disorders (Beblo et al. 2012; Seligman et al. 2006). Evidently, the presence of positive emotions, engagement with life, and meaning-seeking behavior strongly suggest the spiritual emergence profile is not undergoing a prototypical case of Major Depressive Disorder, characterized by the lack of these positive traits. Rather, the manifested positive emotions may be a product of an unwavering sense of calling for meaning discovery. While this sense of calling may be strong, the spiritual emergence profile is in the process of integrating and executing a yet unformulated ideal, which may contribute to a high level of psychopathology (Blatt et al. 1976; Higgins et al. 1985). The presence of positive emotions and engagement alongside pathological symptoms may provide further evidence that the spiritual emergence profile is undergoing a dynamic process of developmental depression that is categorically distinguishable from typical conceptualizations of Major Depressive Disorder.
Those in the socially disengaged profile experience a relatively high level of psychopathology and a low level of positive psychology. This profile exhibits a lower rate of existential engagement and generally low rates of personal growth and purpose in life. Instead of seeking meaning and lacking fulfillment, those in the socially disengaged profile forgo spiritual meaning seeking to a large extent. Based upon age differences and meaning-related covariates, it is possible that the socially disengaged profile diverges developmentally from the spiritual emergence profile. While participants in this profile engaged in a moderately high level of contemplative practice, they exhibited an extremely low rate of love—while they seek alleviation through spiritual practice, they are utterly disconnected from love, both socially and ontologically. Mother Teresa aptly described that “the most terrible poverty is loneliness and the feeling of being unloved.” Spiritual practice, in this case, may function as a compulsive protective mechanism without a deeper sense of existential reflection (Epstein 1990). Understandably, those in this profile suffer from the lowest rate of positive psychology as well. Some claim that more modern forms of spirituality practiced by Westerners may be linked to higher rates of individualism and selfishness that hinder positive social contribution (Bruce 2002; Carrette and King 2005). Other studies have suggested that younger adults who partake in the New Age spirituality and self-spirituality movements sacralize the self while disparaging social institutions, which in turn may explain this profile’s disconnection from love, altruism, and relationships (Aupers and Houtman 2006; Sutcliffe and Gilhus 2014). Furthermore, those in these groups were more likely to have experienced parental rejection and role reversal, which might influence one’s capacity and conceptualization of love as well (Granqvist et al. 2007). The socially disengaged profile likely abandons existential reflection and meaning seeking altogether; they struggle to experience love and connection with others and themselves.
After the inevitable yet normative struggles, we suggest those in the spiritual emergence and socially disconnected profiles ultimately grow into the spiritually integrated (M = 35.1) and virtuous humanist (M = 31.2) profiles, respectively, in their early- to mid-30s. The spiritually integrated profile exhibits an extremely high rate of spiritual reflection and commitment, above average rates of contemplative practice and interconnectedness, and high rates of love and altruism. In this developmental model, those in the spiritual emergence profile likely experience a period of spiritual awakening after one of struggle and adversity, which leads to a dynamic profile shift. The Buddha captured this transition when he asserted, “when you dig a well, there’s no sign of water until you reach it, only rocks and dirt to move out of the way. You have removed enough; soon the pure water will flow” (Tuward 2016). Those in the spiritually integrated profile consequently presented the highest levels of personal growth, purpose in life, and positive psychology. The data suggest the spiritually integrated profile is existentially and spiritually fulfilled. This explains the lower rate of dispositional meaning seeking behavior of this group compared to that of the spiritual emergence group, along with the lowest levels of depression, anxiety, and substance dependence. Those in the spiritually integrated profile are evidently most protected against psychopathology. There is a large body of literature that confirms the protective and thriving benefit of spiritual integration (Ciarrocchi 2012; Elmer et al. 2003; Koenig 2010; Maslow 1962; Miller et al. 2014; Miller and Kelley 2005; Vaughan 2002). Those in the spiritually integrated profile find transcendence and harvest the fruits of labor—spiritual connection, love, and altruism—that the spiritual emergence profile yearns for. Perhaps this hypothesis explains the relatively lower rate of contemplative practice in this profile, as contemplative practice often signifies spiritual effort. Contemplative practice has been shown to effect a profound trait-level shift rather than a state-level shift over a longer period of practice; as a result, allotted periods of practice may be unnecessary (Davidson and Lutz 2008; Goleman and Davidson 2017). As purported in various spiritual and religious texts, we suggest that this developmental path is ultimately buoyant and protective as a permanent trait-level shift but necessitates a period of struggle and stagnation (Friedman et al. 2010; Suzuki 2012).
The likely optimistic avenue of development for the socially disconnected profile is the virtuous humanist profile. The virtuous humanist profile exhibits very low levels of spiritual reflection and commitment, contemplative practice, and interconnectedness and slightly above average levels of love and altruism. Those in this profile displayed the lowest rate of existential engagement, signifying the complete forsaking of meaning seeking within a conventionally spiritual or religious framework (synonymous to the social disengaged profile). Those in the socially disengaged profile abandon spiritual reflection and practice but adopt a human-centered life of love and altruism to develop into the virtuous humanist profile. It is evident from the meaning-related covariates that participants in the path to the virtuous humanist profile have increasingly forgone existential engagement (i.e., meaning seeking). Importantly, however, they discovered meaning fulfillment in their early 30s through a humanistic approach to life—love and altruism. Meaning is therefore found in this profile not through introspection but through the selfless devotion to and connection with others. As Mahatma Gandhi stated, “the best way to find yourself is to lose yourself in the service of others.” The virtuous humanist profile was equally protected against anxiety as the spiritually integrated profile and exhibited a lower rate of depression than all profiles except the spiritually integrated. Previous literature has also found a typology that presents with a low level of conventional spirituality but higher rates of mental health and positive psychology (Barton and Miller 2015; Menkel-Meadow 2001; Westgate 1996). The increasingly popular movement, secular humanism, has been defined as a philosophical stance that values human life, compassion, logic, and reason while rejecting religious dogmatism (Grünbaum 2013). The virtuous humanist profile in the present sample exhibited high rates of atheism and non-religiousness, which further suggests this profile may partake in an ideological stance similar to that of secular humanists.
It is important to note that based on the spiritual profiles in the present study, a higher rate of contemplative practice relative to the rate of love and altruism seems to predict higher levels of psychopathology. In contrast, those who exhibit relatively higher rates of love and altruism compared with rate of contemplative practice are more protected from psychopathology and substance-related disorders. While rate of contemplative practice reflects an individual’s effort in spiritual pursuits (as the factor captures time spent on practicing), love and altruism are intrinsically rewarding domains (Beauregard et al. 2009; Post 2005; Schwartz et al. 2003; Traupmann and Hatfield 1981). It is possible that an effort-reward imbalance in domains of spirituality may play a role in mental health outcomes (Siegrist et al. 2004). We hypothesize that while there is an effort-reward imbalance for emergent profiles, they may ultimately discover spiritual integration and transcendence.
The cross-sectional design does not allow for causal inferences and, therefore, profiles may alter the risk of clinical symptoms, the symptoms may affect profile assignment, or a third factor may influence both. An additional explanation for elevated levels of pathology for those in the spiritual emergence profile may be that individuals with mental illness are more likely to seek coping strategies such as those offered in spiritual, religious, or transcendence-focused contexts. Moreover, due to the cross-sectional design, the hypothesis of profiles as stages in spiritual development is not empirically validated. While there may surely be a group of people who develop into the spiritually integrated and virtuous humanist profiles, there may be others who never progress and confront their shadow self. The significant differences in age amongst profiles represent differences in the mean; as such, there are likely many who become older while remaining in the profiles associated with higher pathology. As mentioned in the introduction, Jung describes this encounter as a “test sufficient to frighten off most people,” and Jaffe explains that most continue to live the unexamined life (Jaffé 1986; Jung 1968). However, corresponding levels of meaning-related covariates and differences in age are strong pieces of evidence that support the hypothesis that it may be normative for people to progress through this developmental path. Future directions might include a longitudinal design incorporating Latent Transition Analysis (LTA) to empirically confirm this hypothesis. An LTA will show the proportion of people who remain in the earlier stage and the proportion of people who progress into subsequent stages. While the present data do not indicate what factors might lead to progression or hindrance in this path, a commonality amongst those who have discovered individuation across traditions seem to be a deep sense of calling, persistence, psychological-mindedness, and courage. A longitudinal study might also examine this question.
The large sample size captured a wide cross-section of the population, yet was limited to people with access to the internet. Nevertheless, large-scale internet-based samples that draw on crowdsourcing have been shown in studies to generate samples more representative of the population than in-person convenience samples (Berinsky et al. 2012; Paolacci and Chandler 2014). In terms of measures, the method of data acquisition relied on self-report instruments rather than behavioral ratings, or clinician-administered interviews. The instruments we employed, however, have shown high validity and high concordance with clinician administered DSM-IV-TR diagnoses in previous studies (Löwe et al. 2008; Manea et al. 2012). Overall, this study presents the first cross-cultural examination of the dynamic profiles of spiritual capacity. We offer data to support previous theoretical explorations on a non-pathological developmental model of spiritual emergence and adult individuation. Pathology in early adulthood may not simply be an illness, but rather, an opportunity for spiritual awakening. Although periods of darkness are inevitable in this path, it is ultimately protective and buoyant.
5. Conclusions
The current study identified potentially dynamic universal profiles of innate spiritual capacity across three countries—China, India, and the United States—using latent profile analysis. We found five profiles across these cultures: non-seeking; socially disconnected; spiritual emergence; virtuous humanist; and spiritually integrated. An examination of the covariates—existential engagement, personal growth, and purpose in life—along with differences in age between profiles suggested that the profiles may represent dynamic stages of an emergent path of spirituality. Regression analyses specifically suggested higher levels of existential engagement along with lower levels of personal growth and purpose in life increased odds of belonging to the spiritual emergence profile, while higher rates of personal growth and purpose in life increased odds of belonging to the spiritually integrated profile. Furthermore, a lower level of existential engagement increased odds of belonging to the virtuous humanist profile. We further examined whether profile assignment significantly predicts distal outcomes including depression, anxiety, positive psychology, and substance dependence. The findings suggested participants more likely to belong in the spiritually integrated profile exhibited the lowest rate of depression, cannabis dependence, and alcohol dependence, along with the highest rate of positive psychology, while those more likely to be in the spiritually integrated and virtuous humanist profiles exhibited the lowest rates of anxiety. The spiritual emergence profile, in contrast, predicted the highest rate of depression, anxiety, and substance dependence. The spiritual emergence profile exhibited 14-times increased likelihood in being dependent on alcohol and almost 20-times increased likelihood in being dependent on cannabis. The present study represents an initial identification and examination of five profiles as stages in the developmental process of spirituality in young adults using an empirical person-centered analytic technique. These potential stages might address some of the mechanisms underlying developmental psychopathology. While struggle is a necessary rite of passage in this developmental path, it ultimately matures into well-being and protection against psychopathology. Developmental depression, anxiety, and substance dependence in young adults may therefore represent a period of normal, non-pathological spiritual growth.
Author Contributions
S.H.C., C.H.-Y.M., E.L., L.M.; methodology, S.H.C., C.H.-Y.M., E.L., L.M.; software, S.H.C., C.H.-Y.M.; validation, S.H.C., C.H.-Y.M., E.L., formal analysis, S.H.C., C.H.-Y.M.; investigation, S.H.C., C.H.-Y.M., E.L., L.M.; resources, L.M.; data curation, S.H.C., C.H.-Y.M., E.L.; writing—original draft preparation, S.H.C.; writing—review and editing, S.H.C., C.H.-Y.M., E.L., L.M.; visualization, S.H.C., L.M.; supervision, L.M.; project administration, S.H.C., C.H.-Y.M., E.L.; funding acquisition, L.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by BOT Trust.
Acknowledgments
The authors would like to thank Jingyi Gu, Diheng Zhang, and Xiao Yang for their assistance with translating survey instruments into Chinese; Jennifer Park, Veronica Kim, Annie Kate Reeder, and Jenny Wang for their assistance with the literature review; and the BOT Trust for their financial support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Anderson, Micheline R., Lisa Miller, Priya Wickramaratne, Connie Svob, Zagaa Odgerel, Ruixin Zhao, and Myrna. M. Weissman. 2017. Genetic correlates of spirituality/religion and depression: A study in offspring and grandchildren at high and low familial risk for depression. Spirituality in Clinical Practice 4: 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Augustine, S. T. 1876. The Confessions. Edinburgh: Clark. [Google Scholar]
- Aupers, Stef, and Houtman Dick. 2006. Beyond the spiritual supermarket: The social and public significance of new age spirituality. Journal of Contemporary Religion 21: 201–22. [Google Scholar] [CrossRef]
- Azhar, M. Z., S. L. Varma, and A. S. Dharap. 1994. Religious psychotherapy in anxiety disorder patients. Acta Psychiatrica Scandinavica 90: 1–3. [Google Scholar] [CrossRef] [PubMed]
- Barton, Yakov A., and Miller Lisa. 2015. Spirituality and positive psychology go hand in hand: An investigation of multiple empirically derived profiles and related protective benefits. Journal of Religion and Health 54: 829–43. [Google Scholar] [CrossRef] [PubMed]
- Barton, Yakov A., Lisa Miller, Priya Wickramaratne, Marc. J Gameroff, and Myrna M. Weissman. 2013. Religious attendance and social adjustment as protective against depression: A 10-year prospective study. Journal of Affective Disorders 146: 53–57. [Google Scholar] [CrossRef] [Green Version]
- Batson, C. Daniel, and Ventis W. Larry. 1982. The Religious Experience: A Social-Psychological Perspective. New York: Oxford University Press. [Google Scholar]
- Beauregard, Mario, Jerome Courtemanche, Vincent Paquette, and Évelyn. Landry St-Pierre. 2009. The neural basis of unconditional love. Psychiatry Research: Neuroimaging 172: 93–98. [Google Scholar] [CrossRef]
- Beblo, Thomas, Silvia Fernando, Sabrina Klocke, Julia Griepenstroh, Steffen Aschenbrenner, and Martin Driessen. 2012. Increased suppression of negative and positive emotions in major depression. Journal of Affective Disorders 141: 23–479. [Google Scholar] [CrossRef]
- Benson, Herbert. 1997. The relaxation response: Therapeutic effect. Science 278: 1693–97. [Google Scholar] [CrossRef]
- Benson, Herbert, John F. Beary, and Mark P. Carol. 1974. The relaxation response. Psychiatry 37: 37–46. [Google Scholar] [CrossRef]
- Berinsky, Adam J., Gregory A. Huber, and Gabriel S. Lenz. 2012. Evaluating online labor markets for experimental research: Amazon. Com’s Mechanical Turk. Political Analysis 20: 351–68. [Google Scholar] [CrossRef] [Green Version]
- Bible, Holy. 1984. New International Version. Grand Rapids: Zondervan. [Google Scholar]
- Blaine, Bruce, and Jennifer Crocker. 1995. Religiousness, race, and psychological well-being: Exploring social psychological mediators. Personality and Social Psychology Bulletin 21: 1031–41. [Google Scholar] [CrossRef] [Green Version]
- Blatt, Sidney J., Joseph P. D’Afflitti, and Donald M. Quinlan. 1976. Experiences of depression in normal young adults. Journal of Abnormal Psychology 85: 4. [Google Scholar] [CrossRef]
- Bonelli, Raphael M., and Harold G. Koenig. 2013. Mental disorders, religion and spirituality 1990 to 2010: A systematic evidence-based review. Journal of Religion and Health 52: 657–73. [Google Scholar] [CrossRef] [PubMed]
- Bruce, Steve. 2002. God is Dead: Secularization in the West. Oxford: Blackwell, vol. 3. [Google Scholar]
- Burris, Jessica L., Shannon E. Sauer, and Charles R. Carlson. 2011. A test of religious commitment and spiritual transcendence as independent predictors of underage alcohol use and alcohol-related problems. Psychology of Religion and Spirituality 3: 3. [Google Scholar] [CrossRef]
- Büssing, Arndt, Thomas Ostermann, and Peter F Matthiessen. 2005. Role of religion and spirituality in medical patients: Confirmatory results with the SpREUK questionnaire. Health and Quality of Life Outcomes 3: 10. [Google Scholar] [CrossRef] [Green Version]
- Button, Tanya M. M., Michael C. Stallings, Soo Hyun Rhee, Robin P. Corley, and John K. Hewitt. 2011. The etiology of stability and change in religious values and religious attendance. Behavior Genetics 41: 201–10. [Google Scholar] [CrossRef] [Green Version]
- Campbell, Joseph. 2008. The Hero with a Thousand Faces. Novato: New World Library, vol. 17. [Google Scholar]
- Campbell, Joseph. 2011. A Joseph Campbell Companion: Reflections on the Art of Living. New York: Joseph Campbell Foundation. [Google Scholar]
- Carrette, Jeremy R., and Richard King. 2005. Selling Spirituality: The Silent Takeover of Religion. Hove: Psychology Press. [Google Scholar]
- Chen, Kuei Min, Jong Ni Lin, Huey Shin Lin, Hui Chan Wu, Wen Ting Chen, Chun Huw Li, and Sing Kai Lo. 2008. The effects of a Simplified Tai-Chi Exercise Program (STEP) on the physical health of older adults living in long-term care facilities: A single group design with multiple time points. International Journal of Nursing Studies 45: 501–7. [Google Scholar] [CrossRef]
- Chih, Ming Yuan. 2014. Exploring the use patterns of a mobile health application for alcohol addiction before the initial lapse after detoxification. In AMIA Annual Symposium Proceedings. Bethesda: American Medical Informatics Association, vol. 2014, p. 385. [Google Scholar]
- Ciarrocchi, Joseph. W. 2012. 27 Positive Psychology and Spirituality: A Virtue-Informed Approach to Well-Being. In The Oxford Handbook of Psychology and Spirituality. New York: Oxford University Press, p. 425. [Google Scholar]
- Cloninger, Claude Robert. 1999. The Temperament and Character Inventory–Revised. St Louis: Center for Psychobiology of Personality, Washington, DC: Washington University. [Google Scholar]
- Collins, Linda M., Penny L. Fidler, Stuart E. Wugalter, and Jefferey D. Long. 1993. Goodness-of-fit testing for latent class models. Multivariate Behavioral Research 28: 375–89. [Google Scholar] [CrossRef]
- Compson, Jane. 2014. Meditation, trauma and suffering in silence: Raising questions about how meditation is taught and practiced in Western contexts in the light of a contemporary trauma resiliency model. Contemporary Buddhism 15: 274–97. [Google Scholar] [CrossRef]
- Curiati, José Antonio, Edimar Bocchi, José Octávio Freire, Ana Claudia Arantes, Márcia Braga, Yolanda Garcia, Guilherme Guimarães, and Wilson Jacob Fo. 2005. Meditation reduces sympathetic activation and improves the quality of life in elderly patients with optimally treated heart failure: A prospective randomized study. Journal of Alternative & Complementary Medicine 11: 465–72. [Google Scholar]
- Davidson, Richard J., and Antoine Lutz. 2008. Buddha’s brain: Neuroplasticity and meditation [in the spotlight]. IEEE Signal Processing Magazine 25: 176–74. [Google Scholar] [CrossRef]
- Dedert, Eric A., Jamie L. Studts, Inka Weissbecker, Paul G. Salmon, Phyllis L. Banis, and Sandra E. Sephton. 2004. Religiosity may help preserve the cortisol rhythm in women with stress-related illness. The International Journal of Psychiatry in Medicine 34: 61–77. [Google Scholar] [CrossRef] [PubMed]
- Delaney, Colleen. 2005. The spirituality scale development and psychometric testing of a holistic instrument to assess the human spiritual dimension. Journal of Holistic Nursing 23: 145–67. [Google Scholar] [CrossRef] [PubMed]
- Durà-Vilà, Glòria, and Simon Dein. 2009. The Dark Night of the Soul: Spiritual distress and its psychiatric implications. Mental Health, Religion and Culture 12: 543–59. [Google Scholar] [CrossRef]
- Elmer, Lori D., Douglas A. MacDonald, and Harris L. Friedman. 2003. Transpersonal psychology, physical health, and mental health: Theory, research, and practice. The Humanistic Psychologist 31: 159–81. [Google Scholar] [CrossRef]
- Engler, Jack. 1984. Therapeutic aims in psychotherapy and meditation: Developmental stages in the representation of self. Journal of Transpersonal Psychology 16: 25–61. [Google Scholar]
- Epstein, Mark. 1990. Psychodynamics of meditation: Pitfalls on the spiritual path. Journal of Transpersonal Psychology 22: 17–34. [Google Scholar]
- Ferrari, Alize J., Fiona J. Charlson, Rosana E. Norman, Scott B. Patten, Greg Freedman, Christopher J. L. Murray, Theo Vos, and Harvey A. Whiteford. 2013. Burden of depressive disorders by country, sex, age, and year: Findings from the global burden of disease study 2010. PLoS Medicine 10: e1001547. [Google Scholar] [CrossRef] [Green Version]
- Fetzer Institute/National Institute on Aging Working Group. 1999. Multidimensional Measurement of Religiousness/Spirituality for Use in Health Research. Kalamazoo: Fetzer Institute. [Google Scholar]
- Fowler, James W., and Robin W. Levin. 1984. Stages of Faith: The Psychology of Human Development and the Quest for Meaning. International Journal for Philosophy of Religion 15: 89–92. [Google Scholar]
- Francis, Leslie. J. 1999. Personality and attitude toward Christianity among undergraduates. Journal of Research on Christian Education. 8: 179–95. [Google Scholar] [CrossRef]
- Friedman, Harris, Stanley Krippner, Linda Riebel, and Chad Johnson. 2010. Transpersonal and other models of spiritual development. International Journal of Transpersonal Studies 29: 1. [Google Scholar] [CrossRef]
- Ghaemi, S. Nassir. 2006. Feeling and time: The phenomenology of mood disorders, depressive realism, and existential psychotherapy. Schizophrenia Bulletin 33: 122–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson-Nylund, Karen, and Andrew Young Choi. 2018. Ten frequently asked questions about latent class analysis. Translational Issues in Psychological Science 4: 440. [Google Scholar] [CrossRef]
- Goleman, Daniel, and Richard J. Davidson. 2017. Altered Traits: Science Reveals How Meditation Changes Your Mind, Brain, and Body. New York: Penguin. [Google Scholar]
- Granqvist, Pehr, Tord Ivarsson, Anders G. Broberg, and Berit Hagekull. 2007. Examining relations among attachment, religiosity, and new age spirituality using the Adult Attachment Interview. Developmental Psychology 43: 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graves, Kenneth Edward, and Alex J. Bowers. 2018. Toward a Typology of Technology-Using Teachers in the “New Digital Divide”: A Latent Class Analysis of the NCES Fast Response Survey System Teachers’ Use of Educational Technology in US Public Schools 2009 (FRSS 95). Teachers College Record 120: 1–42. [Google Scholar]
- Grof, Christina, and Stanislav Grof. 1986. Spiritual emergency: The understanding and treatment of transpersonal crises. Revision. [Google Scholar] [CrossRef]
- Grünbaum, Adolf. 2013. Collected Works, Volume I: Scientific Rationality, the Human Condition, and 20th Century Cosmologies. Oxford: Oxford University Press, vol. 1. [Google Scholar]
- Grunschel, Carola, Justine Patrzek, and Stefan Fries. 2013. Exploring different types of academic delayers: A latent profile analysis. Learning and Individual Differences 23: 225–33. [Google Scholar] [CrossRef]
- Guruge, Ananda W. 1997. The Buddha’s Encounters with Måra the Tempter. Kandy: Buddhist Publication Society. [Google Scholar]
- Hamer, Dean H. 2005. The God Gene: How Faith is Hardwired into Our Genes. New York: Anchor. [Google Scholar]
- Harden, K. Paige. 2010. Does religious involvement protect against early drinking? A behavior genetic approach. The Journal of Child Psychology and Psychiatry 51: 763–71. [Google Scholar] [CrossRef]
- Harris, Maria, and Gabriel Moran. 1998. Reshaping Religious Education: Conversations on Contemporary Practice. Louisville: Westminster John Knox Press. [Google Scholar]
- Higgins, E. Tory, Ruth Klein, and Timothy Strauman. 1985. Self-concept discrepancy theory: A psychological model for distinguishing among different aspects of depression and anxiety. Social Cognition 3: 51–76. [Google Scholar] [CrossRef]
- Hood, Ralph W., Jr. 1975. The construction and preliminary validation of a measure of reported mystical experience. Journal for the Scientific Study of Religion 14: 29–41. [Google Scholar] [CrossRef]
- Jaffé, Aniela. 1986. The Myth of Meaning in the Work of CG Jung. Madrid: Daimon. [Google Scholar]
- James, William. 1902. The Variety of Religious Experience. New York: Library of America. [Google Scholar]
- John, Shaji, Satish Kumar Verma, and Gulshan L. Khanna. 2011. The effect of mindfulness meditation on HPA-Axis in pre-competition stress in sports performance of elite shooters. National Journal of Integrated Research in Medicine 2: 15–21. [Google Scholar]
- Johnston, Lloyd D. 2010. Monitoring the Future: National Survey Results on Drug Use 1975–2008: Vol. II: College Students and Adults Ages 19–50. Collingdale: Diane Publishing. [Google Scholar]
- Jung, Carl Gustav. 1963. Mysterium Coniunctionis. London: Routledge. [Google Scholar]
- Jung, Carl Gustav. 1968. The Archetypes and the Collective Unconscious. Translated by R. F. C. Hull. Princeton: Princeton University Press, vol. 9. [Google Scholar]
- Jung, Carl Gustav. 2014. Psychology and Alchemy. London: Routledge. [Google Scholar]
- Jung, Tony, and K. A. S. Wickrama. 2008. An introduction to latent class growth analysis and growth mixture modeling. Social and Personality Psychology Compass 2: 302–17. [Google Scholar] [CrossRef]
- Kaplan, Zeev, Michael A. Matar, Ram Kamin, Tamar Sadan, and Hagit Cohen. 2005. Stress-related responses after 3 years of exposure to terror in Israel: Are ideological-religious factors associated with resilience? The Journal of Clinical Psychiatry 66: 1146–54. [Google Scholar] [CrossRef] [PubMed]
- Kemperman, Astrid D., and Harry J. Timmermans. 2006. Preferences, benefits, and park visits: A latent class segmentation analysis. Tourism Analysis 11: 221–30. [Google Scholar] [CrossRef]
- Kendler, Kenneth. S., Charles O. Gardner, and Carol A. Prescott. 1997. Religion, psychopathology, and substance use and abuse: A multimeasure, genetic-epidemiologic study. The American Journal of Psychiatry 154: 322–29. [Google Scholar] [CrossRef]
- Kendler, Kenneth S., Charles O. Gardner, and Carol A. Prescott. 1999. Clarifying the relationship between religiosity and psychiatric illness: The impact of covariates and the specificity of buffering effects. Twin Research and Human Genetics 2: 137–44. [Google Scholar] [CrossRef]
- Klemmack, David. L., Lucinda Lee Roff, Michael. W. Parker, Harold G. Koenig, Patricia Sawyer, and Richard M. Allman. 2007. A cluster analysis typology of religiousness/spirituality among older adults. Research on Aging 29: 163–83. [Google Scholar] [CrossRef]
- Koenig, Harold G. 2009. Research on religion, spirituality, and mental health: A review. The Canadian Journal of Psychiatry 54: 283–91. [Google Scholar] [CrossRef] [Green Version]
- Koenig, Harold G. 2010. Spirituality and mental health. International Journal of Applied Psychoanalytic Studies 7: 116–22. [Google Scholar] [CrossRef]
- Koenig, Harold G., and Arndt Büssing. 2010. The Duke University Religion Index (DUREL): A five-item measure for use in epidemiological studies. Religions 1: 78–85. [Google Scholar] [CrossRef] [Green Version]
- Koenig, Harold G., Linda K. George, and Bercedis L. Peterson. 1998. Religiosity and remission of depression in medically ill older patients. The American Journal of Psychiatry 155: 536–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koenig, Laura B., Matt McGue, Robert F. Krueger, and Thomas J. Bouchard. 2005. Genetic and environmental influences on religiousness: Findings for retrospective and current religiousness ratings. Journal of Personality 73: 471–88. [Google Scholar] [CrossRef] [PubMed]
- Krause, Neal. 2003. Religious meaning and subjective well-being in late life. The Journals of Gerontology Series B 58: S160–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kroenke, Kurt, Robert L. Spitzer, and Janet B. Williams. 2001. The Phq-9. Journal of General Internal Medicine 16: 606–13. [Google Scholar] [CrossRef] [PubMed]
- Krygier, Jonathan R., James A. J. Heathers, Sara Shahrestani, Maree Abbott, James J. Gross, and Andrew H. Kemp. 2013. Mindfulness meditation, well-being, and heart rate variability: A preliminary investigation into the impact of intensive Vipassana meditation. International Journal of Psychophysiology 89: 305–13. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, Arnold A. 1976. Psychiatric problems precipitated by transcendental meditation. Psychological Reports 39: 601–2. [Google Scholar] [CrossRef]
- Levin, Jeff. 2000. A prolegomenon to an epidemiology of love: Theory, measurement, and health outcomes. Journal of Social and Clinical Psychology 19: 117. [Google Scholar] [CrossRef]
- Little, Todd D., Ulman Lindenberger, and John R. Nesselroade. 1999. On selecting indicators for multivariate measurement and modeling with latent variables: When “good” indicators are bad and “bad” indicators are good. Psychological Methods 4: 192. [Google Scholar] [CrossRef]
- Lo, Yungtai. 2005. Likelihood ratio tests of the number of components in a normal mixture with unequal varian. Statistics & Probability Letters 71: 225–35. [Google Scholar]
- Lo, Yungtai, Nancy R. Mendell, and Donald B. Rubin. 2001. Testing the number of components in a normal mixture. Biometrika 88: 767–78. [Google Scholar] [CrossRef]
- Löwe, Bernd, Oliver Decker, Stefanie Müller, Elmar Brähler, Dieter Schellberg, Wolfgang Herzog, and Philipp Y. Herzberg. 2008. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Medical Care 46: 266–74. [Google Scholar] [CrossRef] [PubMed]
- Manea, Laura, Simon Gilbody, and Dean McMillan. 2012. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. Canadian Medical Association Journal 184: E191–96. [Google Scholar] [CrossRef] [Green Version]
- Martinotti, Giovanni, Sara Andreoli, Emanuela Giametta, Valeria Poli, Pietro Bria, and Luigi Janiri. 2006. The dimensional assessment of personality in pathologic and social gamblers: The role of novelty seeking and self-transcendence. Comprehensive Psychiatry 47: 350–56. [Google Scholar] [CrossRef] [PubMed]
- Maslow, Abraham H. 1962. Some basic propositions of a growth and self-actualization psychology. In Perceiving, Behaving, Becoming: A New Focus for Education. Washington, DC: Association for Supervision and Curriculum Development, pp. 34–49. [Google Scholar]
- Maslow, Abraham H. 1999. Peak-experiences as acute identity experiences. In Toward a Psychology of Being, 3rd ed. Edited by A. H. Maslow. New York: Wiley, pp. 113–25. [Google Scholar]
- McClintock, Clayton Hoi-Yun, Elsa Lau, and Lisa Miller. 2016. Phenotypic dimensions of spirituality: Implications for mental health in China, India, and the United States. Frontiers in Psychology 7: 1600. [Google Scholar] [CrossRef] [Green Version]
- McLachlan, Geoffrey J., Sharon X. Lee, and Suren I. Rathnayake. 2019. Finite mixture models. Annual Review of Statistics and Its Application 6: 355–78. [Google Scholar] [CrossRef]
- Menkel-Meadow, Carrie. 2001. And now a word about secular humanism, spirituality, and the practice of justice and conflict resolution. Fordham Urban Law Journal 28: 1073. [Google Scholar] [CrossRef] [Green Version]
- Michalon, Max. 2001. “Selflessness” in the service of the ego: Contributions, limitations and dangers of Buddhist psychology for western psychotherapy. American Journal of Psychotherapy 55: 202–18. [Google Scholar] [CrossRef] [Green Version]
- Miller, Lisa. 2013. Spiritual awakening and depression in adolescents: A unified pathway or “two sides of the same coin”. Bulletin of the Menninger Clinic 77: 332–48. [Google Scholar] [CrossRef] [PubMed]
- Miller, Lisa, and Merav Gur. 2002. Religiosity, depression, and physical maturation in adolescent girls. Journal of the American Academy of Child and Adolescent Psychiatry 41: 206–14. [Google Scholar] [CrossRef]
- Miller, Lisa, and Brien S. Kelley. 2005. Relationships of religiosity and spirituality with mental health and psychopathology. In Handbook of the Psychology of Religion and Spirituality. Edited by Raymond F. Paloutzian and Crystal L. Park. New York: The Guilford Press, pp. 460–78. [Google Scholar]
- Miller, Lisa, Priya Wickramaratne, Marc J. Gameroff, Mia Sage, Craig E. Tenke, and Myrna M. Weissman. 2012. Religiosity and major depression in adults at high risk: A ten-year prospective study. The American Journal of Psychiatry 169: 89–94. [Google Scholar] [CrossRef]
- Miller, Lisa, Ravi Bansal, Priya Wickramaratne, Xuejun Hao, Craig E. Tenke, Myrna M. Weissman, and Bradley S. Peterson. 2014. Neuroanatomical correlates of religiosity and spirituality: A study in adults at high and low familial risk for depression. JAMA Psychiatry 71: 128–35. [Google Scholar] [CrossRef] [Green Version]
- Muthén, Bengt O. 2002. Beyond SEM: General latent variable modeling. Behaviormetrika 29: 81–117. [Google Scholar] [CrossRef]
- Muthén, Linda K., and Bengt O. Muthén. 2012. Mplus: The Comprehensive Modeling Program for Applied Researchers. User’s Guide, [Version 7.0]. Los Angeles: Muthén & Muthén. [Google Scholar]
- Nadal, Amber R., Sam A. Hardy, and Carolyn McNamara Barry. 2018. Understanding the roles of religiosity and spirituality in emerging adults in the united states. Psychology of Religion and Spirituality 10: 1. [Google Scholar] [CrossRef]
- Nelson, Christian J., Barry Rosenfeld, William Breitbart, and Michele Galietta. 2002. Spirituality, religion, and depression in the terminally ill. Psychosomatics 43: 213–20. [Google Scholar] [CrossRef]
- Nylund, Karen L., Tihomir Asparouhov, and Bengt O. Muthén. 2007. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Structural Equation Modeling: A Multidisciplinary Journal 14: 535–69. [Google Scholar] [CrossRef]
- O’Connor, Michael. 2002. Spiritual dark night and psychological depression: Some comparisons and considerations. Counseling and Values 46: 137–48. [Google Scholar] [CrossRef]
- Otis, L. 1973. The psychobiology of meditation: Some psychological changes. Paper presented at APA Convention, Montreal, CA, Canada, August. [Google Scholar]
- Paolacci, Gabriele, and Chandler Jesse. 2014. Inside the turk understanding mechanical turk as a participant pool. Current Directions in Psychological Science 23: 184–88. [Google Scholar] [CrossRef] [Green Version]
- Pariante, Carmine M., and Stafford L. Lightman. 2008. The HPA axis in major depression: Classical theories and new developments. Trends in Neurosciences 31: 464–68. [Google Scholar] [CrossRef] [PubMed]
- Park, Nan Sook, Beom S. Lee, Fei Sun, David L. Klemmack, Lucinda L. Roff, and Harold G. Koenig. 2013. Typologies of religiousness/spirituality: Implications for health and well-being. Journal of Religion and Health 52: 828–39. [Google Scholar] [CrossRef]
- Perry, Ralph Barton. 1935. The Thought and Character of William James: As Revealed in Unpublished Correspondence and Notes, Together with His Published Writings. Vol. 1, Inheritance and Vocation; Vol. 2, Philosophy and Psychology. Boston: Little, Brown & Co. [Google Scholar]
- Phongsuphap, Sukanya, Yongyuth Pongsupap, Pakorn Chandanamattha, and Chidchanok Lursinsap. 2008. Changes in heart rate variability during concentration meditation. International Journal of Cardiology 130: 481–84. [Google Scholar] [CrossRef]
- Piedmont, Ralph L. 1999. Does spirituality represent the sixth factor of personality? Spiritual transcendence and the five-factor model. Journal of Personality 67: 985–1013. [Google Scholar] [CrossRef]
- Poll, Justin B., and Timothy B. Smith. 2003. The spiritual self: Toward a conceptualization of spiritual identity development. Journal of Psychology and Theology 31: 129–42. [Google Scholar] [CrossRef]
- Post, Stephen G. 2005. Altruism, happiness, and health: It’s good to be good. International Journal of Behavioral Medicine 12: 2–77. [Google Scholar] [CrossRef] [PubMed]
- Prevatt, J., and R. Park. 1989. The spiritual emergence network (SEN). In Spiritual Emergency: When Personal Transformation Becomes a Crisis. Edited by Stanislav Grof and Christina Grof. New York: TarcherPerigee, pp. 225–32. [Google Scholar]
- Rasic, Daniel, Jennifer A. Robinson, James Bolton, O. Joseph Bienvenu, and Jitender Sareen. 2011. Longitudinal relationships of religious worship attendance and spirituality with major depression, anxiety disorders, and suicidal ideation and attempts: Findings from the Baltimore epidemiologic catchment area study. Journal of Psychiatric Research 45: 848–54. [Google Scholar] [CrossRef]
- Rican, Pavel, and Pavlina Janosova. 2010. Spirituality as a basic aspect of personality: A cross-cultural verification of Piedmont’s model. The International Journal for the Psychology of Religion 20: 2–13. [Google Scholar] [CrossRef]
- Roh, Soonhee, Yeon-Shim Lee, Jae Hoon Lee, and James I. Martin. 2014. Typology of religiosity/spirituality in relation to perceived health, depression, and life satisfaction among older Korean immigrants. Aging & Mental Health 18: 444–53. [Google Scholar]
- Ryff, Carol D. 2014. Psychological well-being revisited: Advances in the science and practice of eudaimonia. Psychotherapy and Psychosomatics 83: 10–28. [Google Scholar] [CrossRef]
- Schwartz, Carolyn, Meisenhelder Janice Bell, Ma Yunsheng, and George Reed. 2003. Altruistic social interest behaviors are associated with better mental health. Psychosomatic Medicine 65: 778–85. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, Gideon. 1978. Estimating the dimension of a model. The Annals of Statistics 6: 461–64. [Google Scholar] [CrossRef]
- Seeman, Teresa E., Linda Fagan Dubin, and Melvin Seeman. 2003. Religiosity/spirituality and health: A critical review of the evidence for biological pathways. American Psychologist 58: 53–63. [Google Scholar] [CrossRef]
- Seidlitz, Larry, Alexis D. Abernethy, Paul R. Duberstein, James S. Evinger, Theresa H. Chang, and Bar’bara L. Lewis. 2002. Development of the spiritual transcendence index. Journal for the Scientific Study of Religion 41: 439–53. [Google Scholar] [CrossRef]
- Seligman, Martin E., Tayyab Rashid, and Acacia C. Parks. 2006. Positive psychotherapy. American Psychologist 61: 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiota, Michelle N., Dacher Keltner, and Oliver P. John. 2006. Positive emotion dispositions differentially associated with Big Five personality and attachment style. The Journal of Positive Psychology 1: 61–71. [Google Scholar] [CrossRef]
- Siegrist, Johannes, Dagmar Starke, Tarani Chandola, Isabelle Godin, Michael Marmot, Isabelle Niedhammer, and Richard Peter. 2004. The measurement of effort–reward imbalance at work: European comparisons. Social Science & Medicine 58: 1483–99. [Google Scholar]
- Sinclair, Shane, Reanne Booker, Tak Fung, Shelley Raffin-Boucha, Bert Enns, Kate Beamer, and Naree Ager. 2016. Factors associated with post-traumatic growth, quality of life, and spiritual well-being in outpatients undergoing bone marrow transplantation: A pilot study. Oncology Nursing Forum 43: 772–80. [Google Scholar] [CrossRef]
- Spitzer, Robert L., Kurt Kroenke, Janet B. W. Williams, and Bernd Löwe. 2006. A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine 166: 1092–97. [Google Scholar] [CrossRef] [Green Version]
- SPSS I. 2011. IBM SPSS Statistics for Windows. Version 20.0. New York: IBM Corp. [Google Scholar]
- Squires, Allison, Linda H. Aiken, Koen Van den Heede, Walter Sermeus, Luk Bruyneel, Rikard Lindqvist, Anneli Ensio, Mayte Moreno-Casbas, Anne Marie Rafferty, Maria Schubert, and et al. 2013. A systematic survey instrument translation process for multi-country, comparative health workforce studies. International Journal of Nursing Studies 50: 264–73. [Google Scholar] [CrossRef] [Green Version]
- Starr, Mirabai. 2003. Dark Night of the Soul: St. John of the Cross. Trans. and Intra. New York: Riverhead. [Google Scholar]
- Sutcliffe, Steven J., and Ingvild S. Gilhus. 2014. New Age Spirituality: Rethinking Religion. Abingdon: Routledge. [Google Scholar]
- Suzuki, Daisetz Teitaro. 2012. Manual of Zen Buddhism, annotated ed. Altenmünster: Jazzybee Verlag. [Google Scholar]
- Tacey, David. 2003. The Spirituality Revolution. Sydney: Harper Collins. [Google Scholar]
- Tang, Yi-Yuan, Yinghua Ma, Yaxin Fan, Hongbo Feng, Junhong Wang, Shigang Feng, Qilin Lu, Bing Hu, Yao Lin, Jian Li, and et al. 2009. Central and autonomic nervous system interaction is altered by short-term meditation. Proceedings of the national Academy of Sciences 106: 8865–70. [Google Scholar] [CrossRef] [Green Version]
- Thayer, Julian F., and Richard D. Lane. 2007. The role of vagal function in the risk for cardiovascular disease and mortality. Biological Psychology 74: 224–42. [Google Scholar] [CrossRef]
- Thoresen, Carl E. 1999. Spirituality and health: Is there a relationship? Journal of Health Psychology 4: 291–300. [Google Scholar] [CrossRef]
- Tofighi, Davood, and Craig K. Enders. 2006. Identifying the correct number of components in a finite mixture model. Computational Statistics 9: 65–78. [Google Scholar]
- Tofighi, Davood, and Craig K. Enders. 2008. Identifying the correct number of classes in growth mixture models. Advances in Latent Variable Mixture Models 2007: 317–41. [Google Scholar]
- Traupmann, Jane, and Elaine Hatfield. 1981. Love and its effect on mental and physical health. In Aging: Stability and Change in the Family. New York: Academic Press, pp. 253–74. [Google Scholar]
- Tuward, Matthew. 2016. Buddha Quotes: Wisdoms for a Better Life. Morrisville: Lulu.com. [Google Scholar]
- Vaughan, Frances. 2002. What is spiritual intelligence? Journal of Humanistic Psychology 42: 2–33. [Google Scholar] [CrossRef]
- Veith, Richard C., Nancy Lewis, Oscar A. Linares, Robert F. Barnes, Murray A. Raskind, Enrique C. Villacres, M. Michele Murburg, E. Alexandra Ashleigh, Sonia Castillo, Elaine R. Peskind, and et al. 1994. Sympathetic nervous system activity in major depression: Basal and desipramine-induced alterations in plasma norepinephrine kinetics. Archives of General Psychiatry 51: 411–22. [Google Scholar] [CrossRef] [PubMed]
- West, Thomas G., and Platon. 1979. Plato’s Apology of Socrates: An Interpretation, with a New Translation. Ithaca: Cornell University Press, p. 66. [Google Scholar]
- Westgate, Charlene E. 1996. Spiritual wellness and depression. Journal of Counseling & Development 75: 26–35. [Google Scholar]
- Wilson, Adam D., Adrian J. Bravo, Matthew R. Pearson, and Katie Witkiewitz. 2016. Finding success in failure: Using latent profile analysis to examine heterogeneity in psychosocial functioning among heavy drinkers following treatment. Addiction 111: 2145–54. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. 2009. Process of Translation and Adaptation of Instruments. Available online: http://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 12 June 2020).
- World Health Organization. 2017. Depression and Other Common Mental Disorders: Global Health Estimates. Geneva: World Health Organization. [Google Scholar]
- Yang, Chih Chien. 1998. Finite Mixture Model Selection with Psychometrics Applications. Ph.D. dissertation, University of California, Los Angeles, CA, USA. [Google Scholar]
- Yang, Chih Chien. 2006. Evaluating latent class analysis models in qualitative phenotype identification. Computational Statistics & Data Analysis 50: 1090–104. [Google Scholar]
- Yonker, Julie E., Chelsea A. Schnabelrauch, and Laura G. DeHaan. 2012. The relationship between spirituality and religiosity on psychological outcomes in adolescents and emerging adults: A meta-analytic review. Journal of Adolescence 35: 299–314. [Google Scholar] [CrossRef]
- Zhang, Jieting, Minqiang Zhang, Wenyi Zhang, and Can Jiao. 2014. Model selection for complex multilevel latent class model. Communications in Statistics-Simulation and Computation 43: 838–50. [Google Scholar] [CrossRef]
Figure 1.
This figure shows the overall Latent Profile Analysis model.

Figure 2.
This figure shows the graphical representation of the profiles. The x-axis represents the indicator variables, and the y-axis represents variance from the mean.
Figure 2.
This figure shows the graphical representation of the profiles. The x-axis represents the indicator variables, and the y-axis represents variance from the mean.

Figure 3.
This figure shows the graphical representation and short description of the virtuous humanist profile.
Figure 3.
This figure shows the graphical representation and short description of the virtuous humanist profile.

Figure 4.
This figure shows the graphical representation and short description of the spiritual emergence profile.
Figure 4.
This figure shows the graphical representation and short description of the spiritual emergence profile.

Figure 5.
This figure shows the graphical representation and short description of the socially disconnected profile.
Figure 5.
This figure shows the graphical representation and short description of the socially disconnected profile.

Figure 6.
This figure shows the graphical representation and short description of the spiritually integrated profile.
Figure 6.
This figure shows the graphical representation and short description of the spiritually integrated profile.

Figure 7.
This figure shows the graphical representation and short description of the non-seeking profile.
Figure 7.
This figure shows the graphical representation and short description of the non-seeking profile.

Figure 8.
This figure displays a simplified diagram depicting how the profiles differ in rates of depression, anxiety, and positive psychology from least to most.
Figure 8.
This figure displays a simplified diagram depicting how the profiles differ in rates of depression, anxiety, and positive psychology from least to most.

Figure 9.
This figure shows a summary of each of the profiles.


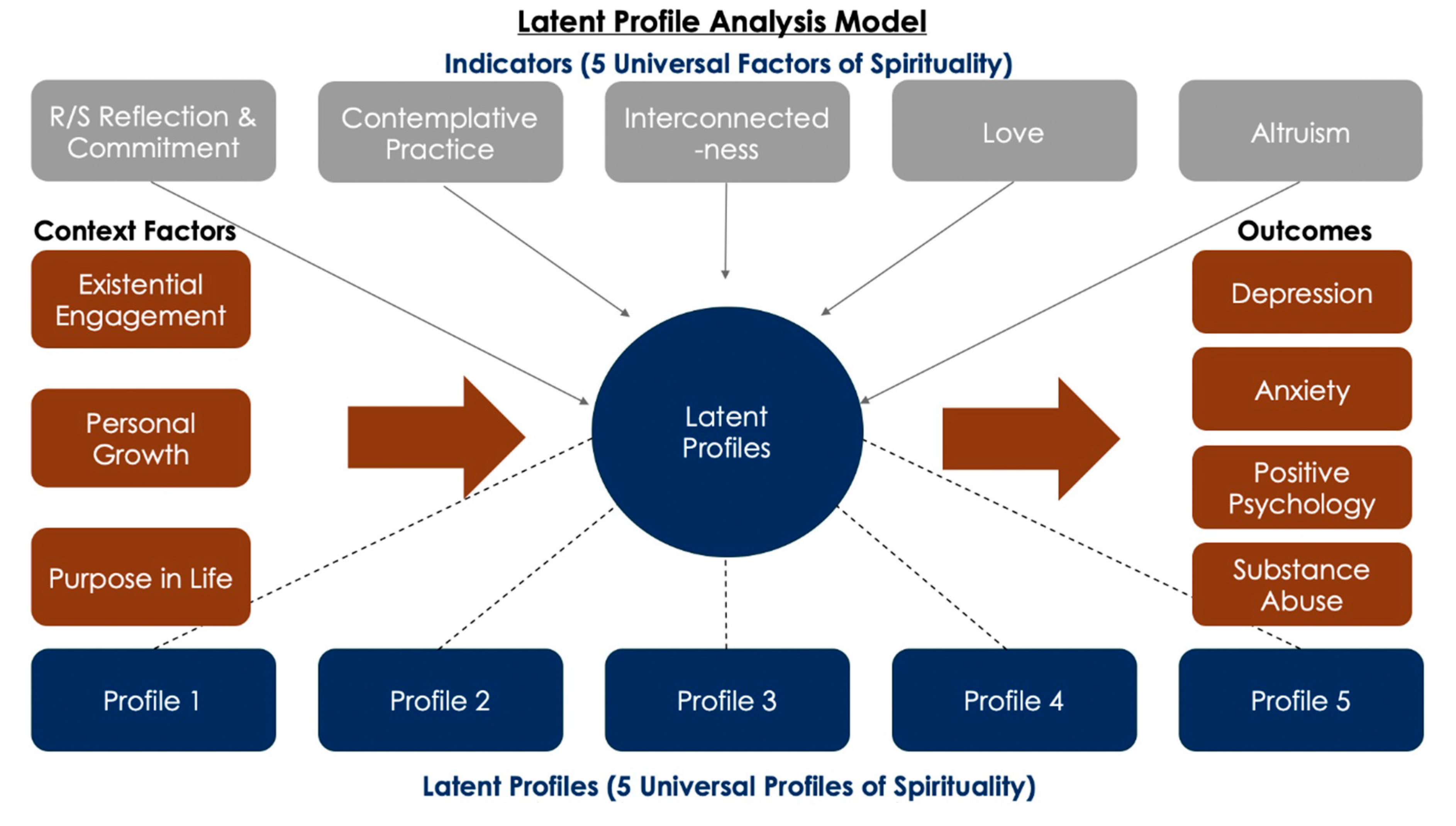{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
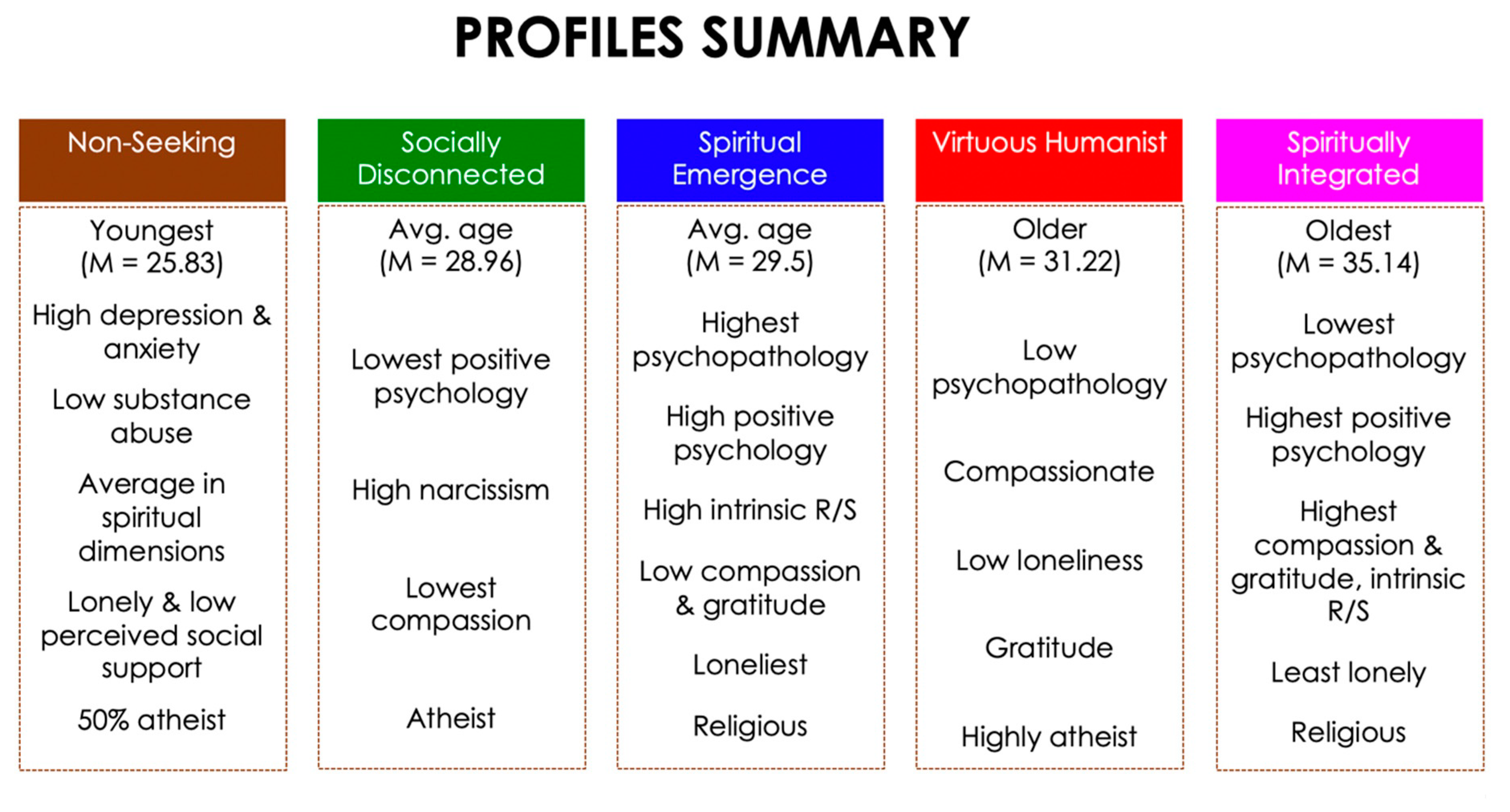{kind=link}
Table 1.
This table shows the sociodemographic characteristics for the overall sample and the sample by country.
Table 1.
This table shows the sociodemographic characteristics for the overall sample and the sample by country.
| Sociodemographic Characteristics of Community Samples in China, India, and the United States | ||||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | Country | Overall Sample | ||||||
| China (N = 3150) | India (N = 863) | United States (N = 1499) | ||||||
| Variable | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| Age | 25.2 | 5.0 | 31.8 | 9.3 | 34.9 | 10.9 | 29.0 | 9.0 |
| N | % | N | % | N | % | N | % | |
| Sex | ||||||||
| Female | 1175 | 37.4 | 328 | 38.0 | 771 | 55.4 | 2274 | 41.3 |
| Male | 1968 | 62.6 | 535 | 62.0 | 728 | 48.6 | 3231 | 58.7 |
| Education level | ||||||||
| Graduate degree | 173 | 5.5 | 302 | 36.5 | 146 | 10.0 | 621 | 11.4 |
| Undergraduate degree | 2011 | 64.1 | 420 | 50.7 | 666 | 45.5 | 3097 | 57.0 |
| Some undergraduate | 611 | 19.5 | 74 | 8.9 | 433 | 29.6 | 1118 | 20.3 |
| High school degree or some high school | 342 | 10.9 | 31 | 3.8 | 220 | 15.0 | 593 | 10.9 |
| Religious affiliation | ||||||||
| Buddhism | 1053 | 33.7 | 1 | <1.0 | 36 | 2.4 | 1090 | 19.9 |
| Christianity | 272 | 8.7 | 145 | 17.0 | 727 | 48.8 | 1144 | 20.9 |
| Hinduism | 4 | <1.0 | 602 | 70.7 | 7 | <1.0 | 613 | 11.2 |
| Islam | 15 | <1.0 | 75 | 8.8 | 13 | <1.0 | 103 | 1.9 |
| Judaism | 11 | <1.0 | 1 | <1.0 | 20 | 1.3 | 32 | <1.0 |
| Other | 366 | 11.7 | 6 | <1.0 | 100 | 6.7 | 472 | 8.6 |
| Non-religious | 1406 | 45 | 21 | 2.5 | 587 | 39.4 | 1406 | 25.7 |
Table 2.
This table displays the latent profile analysis model fit indicators. The bolded row represents the model selected.
Table 2.
This table displays the latent profile analysis model fit indicators. The bolded row represents the model selected.
| Number of Profiles | Logliklihood | AIC | BIC | SABIC | Lo-Mendell-Rubin (k − 1) | p | Entropy | BLRT | p |
|---|---|---|---|---|---|---|---|---|---|
| 1 | −31,712.32 | 63,458.64 | 63,571.09 | 63,517.07 | |||||
| 2 | −30,798.78 | 61,649.55 | 61,821.54 | 61,738.92 | 1803.82 | 0.00 | 0.95 | 1827.09 | 0.00 |
| 3 | −29,811.51 | 59,693.01 | 59,924.52 | 59,813.31 | 1951.89 | 0.00 | 0.80 | 1974.54 | 0.00 |
| 4 | −29,461.52 | 59,011.05 | 59,302.09 | 59,162.28 | 691.05 | 0.00 | 0.76 | 699.96 | 0.00 |
| 5 | −29,128.26 | 58,362.52 | 58,713.10 | 58,544.68 | 658.04 | 0.00 | 0.78 | 666.53 | 0.00 |
| 6 | −28,837.29 | 57,798.58 | 58,208.69 | 58,011.68 | 574.53 | 0.15 | 0.76 | 581.94 | 0.00 |
| 7 | −28,695.31 | 57,532.63 | 58,002.27 | 57,776.65 | 280.34 | 0.05 | 0.77 | 283.96 | 0.00 |
| 8 | −28,535.39 | 57,230.78 | 57,759.95 | 57,505.74 | 315.78 | 0.17 | 0.78 | 319.85 | 0.00 |
| 9 | −28,388.18 | 56,954.36 | 57,543.07 | 57,260.25 | 290.67 | 0.10 | 0.78 | 294.42 | 0.00 |
| 10 | −28,256.76 | 56,709.52 | 57,357.76 | 57,046.34 | 259.50 | 0.02 | 0.79 | 262.84 | 0.00 |
| 11 | −28,158.18 | 56,530.36 | 57,238.13 | 56,898.12 | 209.59 | 0.34 | 0.80 | 212.03 | 0.00 |
| 12 | −28,055.69 | 56,343.39 | 57,110.69 | 56,742.08 | 282.75 | 0.02 | 0.80 | 285.73 | 0.00 |
| 13 | −27,931.05 | 56,112.10 | 56,938.94 | 56,541.73 | 164.80 | 0.50 | 0.81 | 166.71 | 0.00 |
| 14 | −27,844.66 | 55,957.32 | 56,843.69 | 56,417.88 | 277.04 | 0.39 | 0.81 | 280.26 | 0.00 |
| 15 | −27,747.56 | 55,781.11 | 56,727.01 | 56,272.60 | 155.45 | 0.15 | 0.81 | 156.95 | 0.00 |
| 16 | −27,688.37 | 55,680.74 | 56,686.17 | 56,203.16 | 114.27 | 0.23 | 0.82 | 115.47 | 0.00 |
| 17 | −27,637.16 | 55,596.32 | 56,661.28 | 56,149.67 | 250.57 | 0.24 | 0.83 | 252.65 | 0.00 |
| 18 | −27,591.27 | 55,522.54 | 56,647.03 | 56,106.83 | 272.32 | 0.24 | 0.83 | 274.30 | 0.00 |
| 19 | −27,511.46 | 55,380.92 | 56,564.94 | 55,996.14 | 161.12 | 0.13 | 0.83 | 162.37 | 0.00 |
| 20 | −27,463.81 | 55,303.62 | 56,547.18 | 55,949.77 | 110.51 | 0.24 | 0.83 | 111.26 | 0.00 |
| 21 | −27,423.36 | 55,240.73 | 56,543.82 | 55,917.81 | 88.41 | 0.24 | 0.82 | 89.01 | 0.00 |
| 22 | −27,357.97 | 55,127.93 | 56,490.56 | 55,835.96 | 582.28 | 0.36 | 0.81 | 144.60 | 0.36 |
| 23 | −27,313.72 | 55,057.44 | 56,479.60 | 55,796.40 | 92.69 | 0.29 | 0.82 | 93.36 | 0.00 |
Table 3.
This table shows the results of the one-way ANOVA Fisher’s LSD post hoc tests with age as the dependent variable and profiles as the independent variable.
Table 3.
This table shows the results of the one-way ANOVA Fisher’s LSD post hoc tests with age as the dependent variable and profiles as the independent variable.
| One-way ANOVA Fisher’s LSD Post Hoc Tests | ||||
|---|---|---|---|---|
| Reference Profile (I) | Comparison Profile (J) | Mean Difference (I−J) | Std. Error | p |
| 1 | 2 | 1.72 | 0.40 | 0.000 |
| 3 | 2.25 | 0.52 | 0.000 | |
| 4 | −3.92 | 0.41 | 0.000 | |
| 5 | 5.39 | 0.35 | 0.000 | |
| 2 | 1 | −1.72 | 0.40 | 0.000 |
| 3 | 0.53 | 0.50 | 0.283 | |
| 4 | −5.63 | 0.39 | 0.000 | |
| 5 | 3.67 | 0.31 | 0.000 | |
| 3 | 1 | −2.25 | 0.52 | 0.000 |
| 2 | −0.53 | 0.50 | 0.283 | |
| 4 | −6.17 | 0.51 | 0.000 | |
| 5 | 3.14 | 0.45 | 0.000 | |
| 4 | 1 | 3.92 | 0.41 | 0.000 |
| 2 | 5.63 | 0.39 | 0.000 | |
| 3 | 6.17 | 0.51 | 0.000 | |
| 5 | 9.31 | 0.33 | 0.000 | |
| 5 | 1 | −5.39 | 0.35 | 0.000 |
| 2 | −3.67 | 0.31 | 0.000 | |
| 3 | −3.14 | 0.45 | 0.000 | |
| 4 | −9.31 | 0.33 | 0.000 | |
Table 4.
This table shows the results of multinomial logistic regression analyses of covariates—existential engagement, personal growth, and purpose in life.
Table 4.
This table shows the results of multinomial logistic regression analyses of covariates—existential engagement, personal growth, and purpose in life.
| Multinomial Logistic Regression Analyses with Covariates | ||||
|---|---|---|---|---|
| Existential Engagement | ||||
| Profile (vs. 2) | B | Std Error | Exp (B) | p |
| 1 | −0.34 | 0.02 | 0.72 | 0.000 |
| 3 | −0.21 | 0.02 | 0.81 | 0.000 |
| 4 | −0.07 | 0.01 | 0.94 | 0.000 |
| 5 | −0.16 | 0.01 | 0.85 | 0.000 |
| Personal Growth | ||||
| Profile (vs. 2) | B | Std Error | Exp (B) | p |
| 1 | 0.13 | 0.02 | 1.14 | 0.000 |
| 3 | 0.03 | 0.02 | 1.04 | 0.069 |
| 4 | 0.17 | 0.02 | 1.18 | 0.000 |
| 5 | 0.13 | 0.01 | 1.13 | 0.000 |
| Purpose in Life | ||||
| Profile (vs. 2) | B | Std Error | Exp (B) | p |
| 1 | 0.12 | 0.02 | 1.13 | 0.000 |
| 3 | 0.04 | 0.02 | 1.04 | 0.027 |
| 4 | 0.18 | 0.02 | 1.19 | 0.000 |
| 5 | 0.11 | 0.01 | 1.11 | 0.000 |
Table 5.
This table shows the results of binary logistic regression analyses of distal outcomes—depression, anxiety, positive psychology, alcohol dependence, and cannabis dependence.
Table 5.
This table shows the results of binary logistic regression analyses of distal outcomes—depression, anxiety, positive psychology, alcohol dependence, and cannabis dependence.
| Binary Logistic Regression Analyses with Distal Outcomes | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Depression | Anxiety | ||||||||
| Profile (vs. 4) | B | Std Error | Exp (B) | p | Profile (vs. 4) | B | Std Error | Exp (B) | p |
| 1 | 0.14 | 0.13 | 1.16 | 0.274 | 1 | −0.16 | 0.16 | 0.86 | 0.321 |
| 2 | 1.43 | 0.13 | 4.18 | 0.000 | 2 | 1.10 | 0.14 | 3.00 | 0.000 |
| 3 | 0.69 | 0.16 | 1.99 | 0.000 | 3 | 0.13 | 0.19 | 1.14 | 0.485 |
| 5 | 0.61 | 0.11 | 1.84 | 0.000 | 5 | 0.09 | 0.13 | 1.09 | 0.496 |
| Positive Psychology | Alcohol Dependence | ||||||||
| Profile (vs. 4) | B | Std Error | Exp (B) | p | Profile (vs. 4) | B | Std Error | Exp (B) | p |
| 1 | −1.13 | 0.13 | 0.32 | 0.000 | 1 | 1.03 | 0.30 | 2.80 | 0.001 |
| 2 | −0.62 | 0.13 | 0.54 | 0.000 | 2 | 2.66 | 0.33 | 14.35 | 0.000 |
| 3 | −1.94 | 0.19 | 0.14 | 0.000 | 3 | 1.33 | 0.35 | 3.79 | 0.000 |
| 5 | −1.93 | 0.11 | 0.15 | 0.000 | 5 | 0.43 | 0.35 | 1.54 | 0.211 |
| Cannabis Dependence | |||||||||
| Profile (vs. 4) | B | Std Error | Exp (B) | p | |||||
| 1 | 1.38 | 0.29 | 3.97 | 0.000 | |||||
| 2 | 2.99 | 0.34 | 19.82 | 0.000 | |||||
| 3 | 0.35 | 0.35 | 4.36 | 0.000 | |||||
| 5 | 0.76 | 0.36 | 2.13 | 0.035 | |||||
Table 6.
This table shows the results of linear regression analyses of distal outcomes—depression, anxiety, and positive psychology.
Table 6.
This table shows the results of linear regression analyses of distal outcomes—depression, anxiety, and positive psychology.
| Linear Regression Analyses with Distal Outcomes | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Depression (linear regression) | Anxiety (linear regression) | ||||||||
| Profile (vs. 4) | B | Std Error | t | p | Profile (vs. 4) | B | Std Error | t | p |
| 1 | 0.86 | 0.31 | 2.74 | 0.006 | 1 | 0.16 | 0.26 | 0.62 | 0.535 |
| 2 | 3.38 | 0.37 | 9.24 | 0.000 | 2 | 2.35 | 0.31 | 7.65 | 0.000 |
| 3 | 2.41 | 0.42 | 5.73 | 0.000 | 3 | 1.16 | 0.36 | 3.26 | 0.001 |
| 5 | 2.16 | 0.29 | 7.48 | 0.000 | 5 | 1.47 | 0.30 | 4.85 | 0.000 |
| India | India | 0.59 | 0.24 | 2.43 | 0.015 | ||||
| China | China | 0.71 | 0.21 | 3.34 | 0.001 | ||||
| R2 = 0.08 | R2 = 0.04 | ||||||||
| Positive Psychology (linear regression) | |||||||||
| Profile (vs. 4) | B | Std Error | t | p | |||||
| 1 | −0.99 | 0.10 | −10.32 | 0.000 | |||||
| 2 | −0.36 | 0.11 | −3.17 | 0.002 | |||||
| 3 | −1.49 | 0.13 | −11.70 | 0.000 | |||||
| 5 | −0.84 | 0.11 | −7.65 | 0.000 | |||||
| India | 0.39 | 0.09 | 4.37 | 0.000 | |||||
| China | −0.23 | 0.08 | −3.03 | 0.002 | |||||
| R2 = 0.09 | |||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Choi, S.H.; McClintock, C.H.-Y.; Lau, E.; Miller, L. The Dynamic Universal Profiles of Spiritual Awareness: A Latent Profile Analysis. Religions 2020, 11, 288. https://doi.org/10.3390/rel11060288
AMA Style
Choi SH, McClintock CH-Y, Lau E, Miller L. The Dynamic Universal Profiles of Spiritual Awareness: A Latent Profile Analysis. Religions. 2020; 11(6):288. https://doi.org/10.3390/rel11060288
Chicago/Turabian StyleChoi, Simon Hanseung, Clayton Hoi-Yun McClintock, Elsa Lau, and Lisa Miller. 2020. "The Dynamic Universal Profiles of Spiritual Awareness: A Latent Profile Analysis" Religions 11, no. 6: 288. https://doi.org/10.3390/rel11060288
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.