
Arrhythmic Burden in Cardiac Amyloidosis: What We Know and What We Do Not
 , , ,
, , ,
Abstract
:1. Introduction
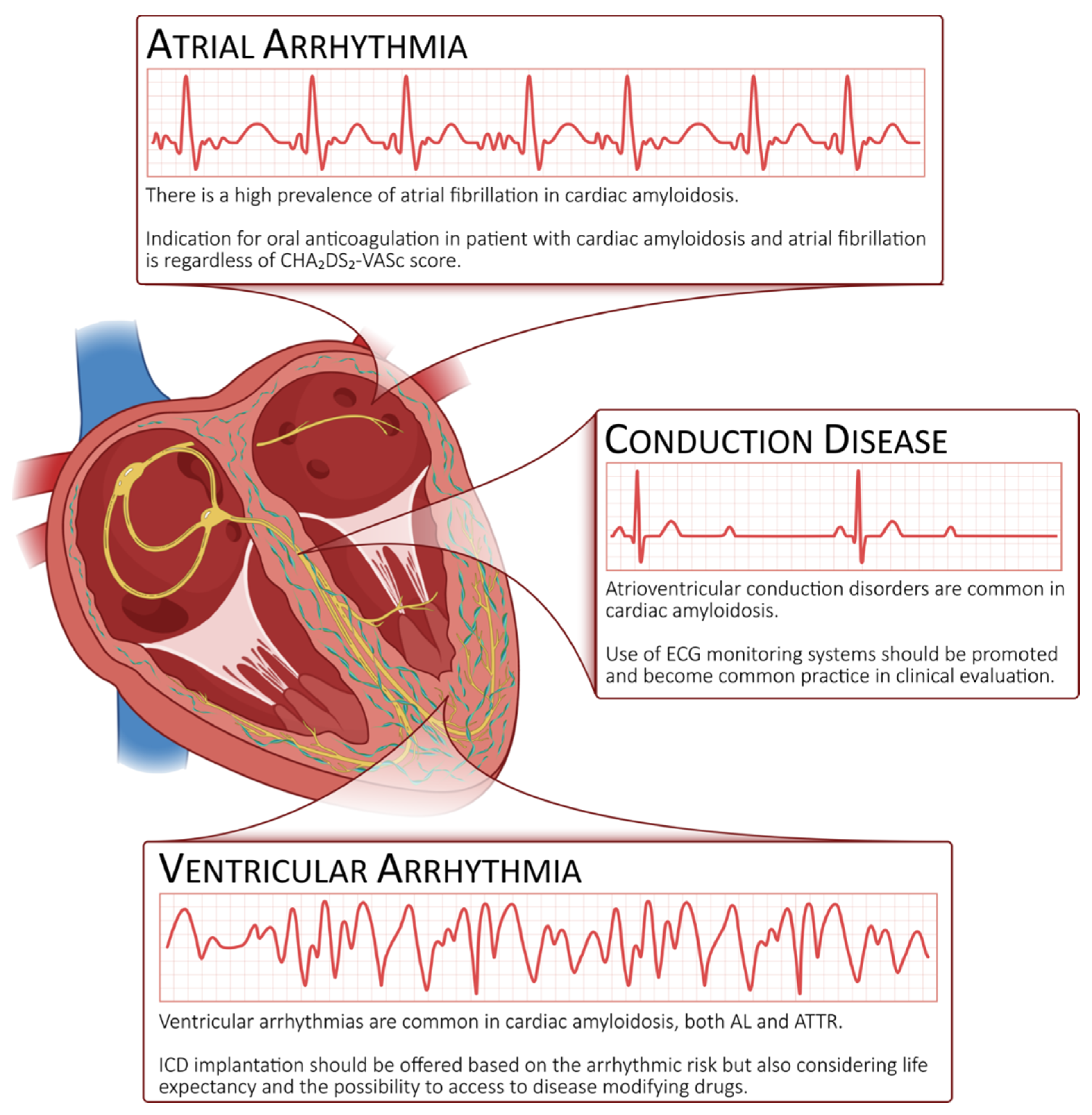
2. Atrial Arrhythmias
2.1. Prevalence
2.2. Pathogenesis
2.3. Arrhythmia Detection
2.4. Prognostic Implications
2.5. Stroke Risk and Anticoagulation
2.6. Our Point of View
2.7. Rate Control
2.8. Rhythm Control
2.9. Atrial Fibrillation in Heart Failure with Preserved Ejection Fraction and Cardiac Amyloidosis
3. Atrioventricular Conduction Diseases
3.1. Pacemaker and Loop Recorder
3.2. Resynchronization Therapy
4. Ventricular Arrhythmias
4.1. Prevalence
4.2. Pathogenesis
4.3. Prognostic Implications
4.4. Sudden Cardiac Death, Pharmacological Treatment and ICD
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- González-López, E.; Gallego-Delgado, M.; Guzzo-Merello, G.; de Haro-Del Moral, F.J.; Cobo-Marcos, M.; Robles, C.; Bornstein, B.; Salas, C.; Lara-Pezzi, E.; Alonso-Pulpon, L.; et al. Wild-type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction. Eur. Heart J. 2015, 36, 2585–2594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chacko, L.; Martone, R.; Bandera, F.; Lane, T.; Martinez-Naharro, A.; Boldrini, M.; Rezk, T.; Whelan, C.; Quarta, C.; Rowczenio, D.; et al. Echocardiographic phenotype and prognosis in transthyretin cardiac amyloidosis. Eur. Heart J. 2020, 41, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Baggiano, A.; Boldrini, M.; Martinez-Naharro, A.; Kotecha, T.; Petrie, A.; Rezk, T.; Gritti, M.; Quarta, C.; Knight, D.S.; Wechalekar, A.D.; et al. Noncontrast Magnetic Resonance for the Diagnosis of Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2020, 13, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Griffin, J.M.; Rosenblum, H.; Maurer, M.S. Pathophysiology and Therapeutic Approaches to Cardiac Amyloidosis. Circ. Res. 2021, 128, 1554–1575. [Google Scholar] [CrossRef] [PubMed]
- Mints, Y.Y.; Doros, G.; Berk, J.L.; Connors, L.; Ruberg, F.L. Features of atrial fibrillation in wild-type transthyretin cardiac amyloidosis: A systematic review and clinical experience. ESC Heart Fail. 2018, 5, 772–779. [Google Scholar] [CrossRef]
- Zampieri, M.; Allinovi, M.; Olivotto, I.; Antonioli, E.; Gabriele, M.; Argirò, A.; Fumagalli, C.; Nardi, G.; Di Mario, C.; Vannucchi, A.M.; et al. Ventricular tachyarrhythmias and sudden cardiac death in light-chain amyloidosis: A clash of cardio-toxicities? Br. J. Haematol. 2021, 193, e27–e31. [Google Scholar] [CrossRef]
- Rapezzi, C.; Merlini, G.; Quarta, C.C.; Riva, L.; Longhi, S.; Leone, O.; Salvi, F.; Ciliberti, P.; Pastorelli, F.; Biagini, E.; et al. Systemic cardiac amyloidoses: Disease profiles and clinical courses of the 3 main types. Circulation 2009, 120, 1203–1212. [Google Scholar] [CrossRef] [Green Version]
- Plehn, J.F.; Southworth, J.; Cornwell, G.G. Brief report: Atrial systolic failure in primary amyloidosis. N. Engl. J. Med. 1992, 327, 1570–1573. [Google Scholar] [CrossRef]
- Bandera, F.; Martone, R.; Chacko, L.; Ganesananthan, S.; Gilbertson, J.A.; Ponticos, M.; Lane, T.; Martinez-Naharro, A.; Whelan, C.; Quarta, C.; et al. Clinical Importance of Left Atrial Infiltration in Cardiac Transthyretin Amyloidosis. JACC Cardiovasc. Imaging 2021, 15, 17–29. [Google Scholar] [CrossRef]
- Sanchis, K.; Cariou, E.; Colombat, M.; Ribes, D.; Huart, A.; Cintas, P.; Fournier, P.; Rollin, A.; Carrié, D.; Galinier, M.; et al. Atrial fibrillation and subtype of atrial fibrillation in cardiac amyloidosis: Clinical and echocardiographic features, impact on mortality. Amyloid 2019, 26, 128–138. [Google Scholar] [CrossRef]
- Papathanasiou, M.; Jakstaite, A.; Oubari, S.; Siebermair, J.; Wakili, R.; Hoffmann, J.; Carpinteiro, A.; Hagenacker, T.; Thimm, A.; Rischpler, C.; et al. Clinical features and predictors of atrial fibrillation in patients with light-chain or transthyretin cardiac amyloidosis. ESC Heart Fail. 2022, 9, 1740–1748. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Bhaskaran, A. Atrial Fibrillation in Transthyretin Cardiac Amyloidosis: The Growing Need to Look Forward. JACC Clin. Electrophysiol. 2020, 6, 1128–1130. [Google Scholar] [CrossRef] [PubMed]
- Barbhaiya, C.R.; Kumar, S.; Baldinger, S.; Michaud, G.F.; Stevenson, W.G.; Falk, R.; John, R.M. Electrophysiologic assessment of conduction abnormalities and atrial arrhythmias associated with amyloid cardiomyopathy. Heart Rhythm 2016, 13, 383–390. [Google Scholar] [CrossRef]
- Sukhacheva, T.V.; Nizyaeva, N.V.; Samsonova, M.V.; Cherniaev, A.L.; Burov, A.A.; Iurova, M.V.; Shchegolev, A.I.; Serov, R.A.; Sukhikh, G.T. Morpho-functional changes of cardiac telocytes in isolated atrial amyloidosis in patients with atrial fibrillation. Sci. Rep. 2021, 11, 3563. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.A.; Jain, M.; Pimentel, D.R.; Wang, B.; Connors, L.H.; Skinner, M.; Apstein, C.S.; Liao, R. Human Amyloidogenic Light Chains Directly Impair Cardiomyocyte Function Through an Increase in Cellular Oxidant Stress. Circ. Res. 2004, 94, 1008–1010. [Google Scholar] [CrossRef] [Green Version]
- Dorbala, S.; Vangala, D.; Bruyere, J.; Quarta, C.; Kruger, J.; Padera, R.; Foster, C.; Hanley, M.; Di Carli, M.F.; Falk, R. Coronary Microvascular Dysfunction Is Related to Abnormalities in Myocardial Structure and Function in Cardiac Amyloidosis. JACC Heart Fail. 2014, 2, 358–367. [Google Scholar] [CrossRef]
- Donnellan, E.; Wazni, O.M.; Hanna, M.; Elshazly, M.B.; Puri, R.; Saliba, W.; Kanj, M.; Vakamudi, S.; Patel, D.R.; Baranowski, B.; et al. Atrial Fibrillation in Transthyretin Cardiac Amyloidosis. JACC Clin. Electrophysiol. 2020, 6, 1118–1127. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.P.; Damy, T.; Eriksson, U.; et al. Diagnosis and treatment of cardiac amyloidosis: A position statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2021, 42, 1554–1568. [Google Scholar] [CrossRef]
- Dale, Z.; Chandrashekar, P.; Al-Rashdan, L.; Gill, S.; Elman, M.; Fischer, K.L.; Nazer, B.; Masri, A. Routine ambulatory heart rhythm monitoring for detection of atrial arrhythmias in transthyretin cardiac amyloidosis. Int. J. Cardiol. 2022, 358, 65–71. [Google Scholar] [CrossRef]
- Lohrmann, G.; Patel, M.A.; Brauneis, D.; Sanchorawala, V.; Sarosiek, S.; Vellanki, N.; Siddiqi, O.K.; Ruberg, F.L.; Gopal, D.M. Left Atrial Mechanics Associates with Paroxysmal Atrial Fibrillation in Light-Chain Amyloidosis Following Stem Cell Transplantation. JACC CardioOncology 2020, 2, 721–731. [Google Scholar] [CrossRef]
- Aquaro, G.D.; Morini, S.; Grigoratos, C.; Taborchi, G.; Di Bella, G.; Martone, R.; Vignini, E.; Emdin, M.; Olivotto, I.; Perfetto, F.; et al. Electromechanical dissociation of left atrium in patients with Cardiac Amyloidosis by Magnetic Resonance: Prognostic and clinical correlates. IJC Heart Vasc. 2020, 31, 100633. [Google Scholar] [CrossRef]
- Versteylen, M.O.; Brons, M.; Teske, A.J.; Oerlemans, M.I.F.J. Restrictive Atrial Dysfunction in Cardiac Amyloidosis: Differences between Immunoglobulin Light Chain and Transthyretin Cardiac Amyloidosis Patients. Biomedicines 2022, 10, 1768. [Google Scholar] [CrossRef] [PubMed]
- Minamisawa, M.; Inciardi, R.M.; Claggett, B.; Cuddy, S.A.; Quarta, C.C.; Shah, A.M.; Dorbala, S.; Falk, R.H.; Matsushita, K.; Kitzman, D.W.; et al. Left atrial structure and function of the amyloidogenic V122I transthyretin variant in elderly African Americans. Eur. J. Heart Fail. 2021, 23, 1290–1295. [Google Scholar] [CrossRef] [PubMed]
- Cappelli, F.; Tini, G.; Russo, D.; Emdin, M.; Del Franco, A.; Vergaro, G.; Di Bella, G.; Mazzeo, A.; Canepa, M.; Volpe, M.; et al. Arterial thrombo-embolic events in cardiac amyloidosis: A look beyond atrial fibrillation. Amyloid 2021, 28, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Stables, R.H.; Ormerod, O.J.M. Atrial thrombi occurring during sinus rhythm in cardiac amyloidosis: Evidence for atrial electromechanical dissociation. Heart Br. Card. Soc. 1996, 75, 426. [Google Scholar] [CrossRef] [Green Version]
- Feng, D.; Edwards, W.D.; Oh, J.K.; Chandrasekaran, K.; Grogan, M.; Martinez, M.W.; Syed, I.I.; Hughes, D.A.; Lust, J.A.; Jaffe, A.S.; et al. Intracardiac Thrombosis and Embolism in Patients with Cardiac Amyloidosis. Circulation 2007, 116, 2420–2426. [Google Scholar] [CrossRef] [Green Version]
- Feng, D.; Syed, I.S.; Martinez, M.; Oh, J.K.; Jaffe, A.S.; Grogan, M.; Edwards, W.D.; Gertz, M.A.; Klarich, K.W. Intracardiac Thrombosis and Anticoagulation Therapy in Cardiac Amyloidosis. Circulation 2009, 119, 2490–2497. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Naharro, A.; Gonzalez-Lopez, E.; Corovic, A.; Mirelis, J.G.; Baksi, A.J.; Moon, J.; Garcia-Pavia, P.; Gillmore, J.D.; Hawkins, P.N.; Fontana, M. High Prevalence of Intracardiac Thrombi in Cardiac Amyloidosis. J. Am. Coll. Cardiol. 2019, 73, 1733–1734. [Google Scholar] [CrossRef]
- Dubrey, S.; Pollak, A.; Skinner, M.; Falk, R.H. Atrial thrombi occurring during sinus rhythm in cardiac amyloidosis: Evidence for atrial electromechanical dissociation. Br. Heart J. 1995, 74, 541–544. [Google Scholar] [CrossRef] [Green Version]
- Vilches, S.; Fontana, M.; Gonzalez-Lopez, E.; Mitrani, L.; Saturi, G.; Renju, M.; Griffin, J.M.; Caponetti, A.; Gnanasampanthan, S.; Santos, J.D.L.; et al. Systemic embolism in amyloid transthyretin cardiomyopathy. Eur. J. Heart Fail. 2022, 24, 1387–1396. [Google Scholar] [CrossRef]
- Mitrani, L.R.; Santos, J.D.L.; Driggin, E.; Kogan, R.; Helmke, S.; Goldsmith, J.; Biviano, A.B.; Maurer, M.S. Anticoagulation with warfarin compared to novel oral anticoagulants for atrial fibrillation in adults with transthyretin cardiac amyloidosis: Comparison of thromboembolic events and major bleeding. Amyloid Int. J. Exp. Clin. Investig. Off. J. Int. Soc. Amyloidosis 2021, 28, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Cariou, E.; Sanchis, K.; Rguez, K.; Blanchard, V.; Cazalbou, S.; Fournier, P.; Huart, A.; Roussel, M.; Cintas, P.; Galinier, M.; et al. New Oral Anticoagulants vs. Vitamin K Antagonists Among Patients with Cardiac Amyloidosis: Prognostic Impact. Front. Cardiovasc. Med. 2021, 8, 742428. [Google Scholar] [CrossRef] [PubMed]
- Falk, R.H.; Rubinow, A.; Cohen, A.S. Cardiac arrhythmias in systemic amyloidosis: Correlation with echocardiographic abnormalities. J. Am. Coll. Cardiol. 1984, 3, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Giancaterino, S.; Urey, M.A.; Darden, D.; Hsu, J.C. Management of Arrhythmias in Cardiac Amyloidosis. JACC Clin. Electrophysiol. 2020, 6, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Rubinow, A.; Skinner, M.; Cohen, A.S. Digoxin sensitivity in amyloid cardiomyopathy. Circulation 1981, 63, 1285–1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, J.P.; Sperry, B.W.; Gabrovsek, A.; Ikram, A.; Tang, W.W.; Estep, J.; Hanna, M. Digoxin Use in Cardiac Amyloidosis. Am. J. Cardiol. 2020, 133, 134–138. [Google Scholar] [CrossRef]
- January, C.T. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation 2014, 130, 2071–2104. [Google Scholar] [CrossRef] [Green Version]
- Kristen, A.V.; Dengler, T.J.; Hegenbart, U.; Schönland, S.; Goldschmidt, H.; Sack, F.-U.; Voss, F.; Becker, R.; Katus, H.A.; Bauer, A. Prophylactic implantation of cardioverter-defibrillator in patients with severe cardiac amyloidosis and high risk for sudden cardiac death. Heart Rhythm 2008, 5, 235–240. [Google Scholar] [CrossRef]
- Kim, E.-J.; Holmes, B.B.; Huang, S.; Lugo, R.; Al Aboud, A.; Goodman, S.; Hung, R.R.; Slosky, D.; Stevenson, W.G.; Michaud, G.F.; et al. Outcomes in patients with cardiac amyloidosis and implantable cardioverter-defibrillator. EP Europace 2020, 22, 1216–1223. [Google Scholar] [CrossRef]
- Khanna, S.; Lo, P.; Cho, K.; Subbiah, R. Ventricular Arrhythmias in Cardiac Amyloidosis: A Review of Current Literature. Clin. Med. Insights Cardiol. 2020, 14, 1179546820963055. [Google Scholar] [CrossRef]
- Kocher, F.; Kaser, A.; Escher, F.; Doerler, J.; Zaruba, M.; Messner, M.; Mussner-Seeber, C.; Mayr, A.; Ulmer, H.; Schneiderbauer-Porod, S.; et al. Heart failure from ATTRwt amyloid cardiomyopathy is associated with poor prognosis. ESC HeartFail. 2020, 7, 3919–3928. [Google Scholar] [CrossRef] [PubMed]
- Higgins, A.Y.; Annapureddy, A.R.; Wang, Y.; Minges, K.E.; Lampert, R.; Rosenfeld, L.E.; Jacoby, D.L.; Curtis, J.P.; Miller, E.J.; Freeman, J.V. Survival Following Implantable Cardioverter-Defibrillator Implantation in Patients with Amyloid Cardiomyopathy. J. Am. Heart Assoc. 2020, 9, e016038. [Google Scholar] [CrossRef] [PubMed]
- El-Am, E.A.; Dispenzieri, A.; Melduni, R.M.; Ammash, N.M.; White, R.D.; Hodge, D.O.; Noseworthy, P.A.; Lin, G.; Pislaru, S.V.; Egbe, A.C.; et al. Direct Current Cardioversion of Atrial Arrhythmias in Adults with Cardiac Amyloidosis. J. Am. Coll. Cardiol. 2019, 73, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Tan, N.Y.; Mohsin, Y.; Hodge, D.O.; Lacy, M.Q.; Packer, D.L.; Dispenzieri, A.; Grogan, M.; Asirvatham, S.J.; Madhavan, M.; McLeod, C.J. Catheter Ablation for Atrial Arrhythmias in Patients with Cardiac Amyloidosis. J. Cardiovasc. Electrophysiol. 2016, 27, 1167–1173. [Google Scholar] [CrossRef]
- Donnellan, E.; Wazni, O.; Kanj, M.; Elshazly, M.B.; Hussein, A.; Baranowski, B.; Hanna, M.; Patel, D.; Trulock, K.; Martyn, M.; et al. Atrial fibrillation ablation in patients with transthyretin cardiac amyloidosis. Eur. Pacing Arrhythm. Card. Electrophysiol. J. Work. Groups Card. Pacing Arrhythm. Card. Cell. Electrophysiol. Eur. Soc. Cardiol. 2020, 22, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.B.; Januzzi, J.L.; O’Neill, B.J.; Gundapaneni, B.; Patterson, T.A.; Sultan, M.B.; López-Sendón, J. Causes of Cardiovascular Hospitalization and Death in Patients with Transthyretin Amyloid Cardiomyopathy (from the Tafamidis in Transthyretin Cardiomyopathy Clinical Trial [ATTR-ACT]). Am. J. Cardiol. 2021, 148, 146–150. [Google Scholar] [CrossRef]
- Kotecha, D. Heart Failure with Preserved Ejection Fraction and Atrial Fibrillation: Vicious Twins. J. Am. Coll. Cardiol. 2016, 68, 2217–2228. [Google Scholar] [CrossRef]
- Vermond, R.A.; Geelhoed, B.; Verweij, N.; Tieleman, R.G.; Van der Harst, P.; Hillege, H.L.; Van Gilst, W.H.; Van Gelder, I.C.; Rienstra, M. Incidence of Atrial Fibrillation and Relationship with Cardiovascular Events, Heart Failure, and Mortality. J. Am. Coll. Cardiol. 2015, 66, 1000–1007. [Google Scholar] [CrossRef] [Green Version]
- Zakeri, R.; Chamberlain, A.M.; Roger, V.L.; Redfield, M.M. Temporal relationship and prognostic significance of atrial fibrillation in heart failure patients with preserved ejection fraction: A community-based study. Circulation 2013, 128, 1085–1093. [Google Scholar] [CrossRef] [Green Version]
- Sanders, P.; Morton, J.B.; Davidson, N.C.; Spence, S.J.; Vohra, J.K.; Sparks, P.B.; Kalman, J.M. Electrical remodeling of the atria in congestive heart failure: Electrophysiological and electroanatomic mapping in humans. Circulation 2003, 108, 1461–1468. [Google Scholar] [CrossRef]
- Longhi, S.; Quarta, C.C.; Milandri, A.; Lorenzini, M.; Gagliardi, C.; Manuzzi, L.; Reggiani, M.L.B.; Leone, O.; Ferlini, A.; Russo, A.; et al. Atrial fibrillation in amyloidotic cardiomyopathy: Prevalence, incidence, risk factors and prognostic role. Amyloid Int. J. Exp. Clin. Investig. Off. J. Int. Soc. Amyloidosis 2015, 22, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.S.P.; Rienstra, M.; Tay, W.T.; Liu, L.C.; Hummel, Y.M.; van der Meer, P.; de Boer, R.A.; Van Gelder, I.C.; van Veldhuisen, D.J.; Voors, A.A.; et al. Atrial Fibrillation in Heart Failure with Preserved Ejection Fraction: Association with Exercise Capacity, Left Ventricular Filling Pressures, Natriuretic Peptides, and Left Atrial Volume. JACC Heart Fail. 2017, 5, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Porcari, A.; Rossi, M.; Cappelli, F.; Canepa, M.; Musumeci, B.; Cipriani, A.; Tini, G.; Barbati, G.; Varrà, G.G.; Morelli, C.; et al. Incidence and risk factors for pacemaker implantation in light-chain and transthyretin cardiac amyloidosis. Eur. J. Heart Fail. 2022, 24, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Cappelli, F.; Vignini, E.; Martone, R.; Perlini, S.; Mussinelli, R.; Sabena, A.; Morini, S.; Gabriele, M.; Taborchi, G.; Bartolini, S.; et al. Baseline ECG Features and Arrhythmic Profile in Transthyretin Versus Light Chain Cardiac Amyloidosis. Circ. Heart Fail. 2020, 13, e006619. [Google Scholar] [CrossRef] [PubMed]
- Falk, R.H. Diagnosis and Management of the Cardiac Amyloidoses. Circulation 2005, 112, 2047–2060. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M.; Banypersad, S.M.; Treibel, T.; Abdel-Gadir, A.; Maestrini, V.; Lane, T.; Gilbertson, J.A.; Hutt, D.F.; Lachmann, H.; Whelan, C.J.; et al. Differential Myocyte Responses in Patients with Cardiac Transthyretin Amyloidosis and Light-Chain Amyloidosis: A Cardiac MR Imaging Study. Radiology 2015, 277, 388–397. [Google Scholar] [CrossRef]
- Frustaci, A.; Letizia, C.; Adamo, F.; Grande, C.; Verardo, R.; Chimenti, C. A-V block as presentation of cardiac amyloid: Prominent infiltration of conduction tissue revealed by endomyocardial biopsy. Amyloid Int. J. Exp. Clin. Investig. Off. J. Int. Soc. Amyloidosis 2017, 24, 131–132. [Google Scholar] [CrossRef]
- Kotecha, T.; Martinez-Naharro, A.; Treibel, T.A.; Francis, R.; Nordin, S.; Abdel-Gadir, A.; Knight, D.S.; Zumbo, G.; Rosmini, S.; Maestrini, V.; et al. Myocardial Edema and Prognosis in Amyloidosis. J. Am. Coll. Cardiol. 2018, 71, 2919–2931. [Google Scholar] [CrossRef]
- Mishra, S.; Guan, J.; Plovie, E.; Seldin, D.C.; Connors, L.H.; Merlini, G.; Falk, R.H.; MacRae, C.A.; Liao, R. Human amyloidogenic light chain proteins result in cardiac dysfunction, cell death, and early mortality in zebrafish. Am. J. Physiol. Circ. Physiol. 2013, 305, H95–H103. [Google Scholar] [CrossRef] [Green Version]
- Morimoto, S.-I.; Kato, S.; Hiramitsu, S.; Uemura, A.; Ohtsuki, M.; Kato, Y.; Sugiura, A.; Miyagishima, K.; Yoshida, Y.; Hishida, H. Role of myocardial interstitial edema in conduction disturbances in acute myocarditis. Heart Vessel. 2006, 21, 356–360. [Google Scholar] [CrossRef]
- Rehorn, M.R.; Loungani, R.S.; Black-Maier, E.; Coniglio, A.C.; Karra, R.; Pokorney, S.D.; Khouri, M.G. Cardiac Implantable Electronic Devices: A Window into the Evolution of Conduction Disease in Cardiac Amyloidosis. JACC Clin. Electrophysiol. 2020, 6, 1144–1154. [Google Scholar] [CrossRef] [PubMed]
- Sayed, R.H.; Rogers, D.; Khan, F.; Wechalekar, A.D.; Lachmann, H.J.; Fontana, M.; Mahmood, S.; Sachchithanantham, S.; Patel, K.; Hawkins, P.N.; et al. A study of implanted cardiac rhythm recorders in advanced cardiac AL amyloidosis. Eur. Heart J. 2015, 36, 1098–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Algalarrondo, V.; Dinanian, S.; Juin, C.; Chemla, D.; Bennani, S.L.; Sebag, C.; Planté, V.; Le Guludec, D.; Samuel, D.; Adams, D.; et al. Prophylactic pacemaker implantation in familial amyloid polyneuropathy. Heart Rhythm 2012, 9, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Donnellan, E.; Wazni, O.M.; Saliba, W.I.; Hanna, M.; Kanj, M.; Patel, D.R.; Wilner, B.; Kochar, A.; Jaber, W.A. Prevalence, Incidence, and Impact on Mortality of Conduction System Disease in Transthyretin Cardiac Amyloidosis. Am. J. Cardiol. 2020, 128, 140–146. [Google Scholar] [CrossRef]
- Donnellan, E.; Wazni, O.M.; Saliba, W.I.; Baranowski, B.; Hanna, M.; Martyn, M.; Patel, D.; Trulock, K.; Menon, V.; Hussein, A.; et al. Cardiac devices in patients with transthyretin amyloidosis: Impact on functional class, left ventricular function, mitral regurgitation, and mortality. J. Cardiovasc. Electrophysiol. 2019, 30, 2427–2432. [Google Scholar] [CrossRef]
- Cappelli, F.; Cipriani, A.; Russo, D.; Tini, G.; Zampieri, M.; Zocchi, C.; Sinigiani, G.; Tassetti, L.; Licchelli, L.; Perfetto, F.; et al. Prevalence and prognostic role of nonsustained ventricular tachycardia in cardiac amyloidosis. Amyloid 2022, 29, 1–2. [Google Scholar] [CrossRef]
- Hörnsten, R.; Wiklund, U.; Olofsson, B.-O.; Jensen, S.M.; Suhr, O.B. Liver Transplantation Does Not Prevent the Development of Life-Threatening Arrhythmia in Familial Amyloidotic Polyneuropathy, Portuguese-Type (ATTR Val30Met) Patients. Transplantation 2004, 78, 112–116. [Google Scholar] [CrossRef]
- Palladini, G.; Malamani, G.; Co, F.; Pistorio, A.; Recusani, F.; Anesi, E.; Garini, P.; Merlini, G. Holter Monitoring in AL Amyloidosis: Prognostic Implications. Pacing Clin. Electrophysiol. PACE 2001, 24, 1228–1233. [Google Scholar] [CrossRef]
- Goldsmith, Y.B.; Liu, J.; Chou, J.; Hoffman, J.; Comenzo, R.L.; Steingart, R.M. Frequencies and Types of Arrhythmias in Patients with Systemic Light-Chain Amyloidosis With Cardiac Involvement Undergoing Stem Cell Transplantation on Telemetry Monitoring. Am. J. Cardiol. 2009, 104, 990–994. [Google Scholar] [CrossRef]
- Varr, B.C.; Zarafshar, S.; Coakley, T.; Liedtke, M.; Lafayette, R.A.; Arai, S.; Schrier, S.L.; Witteles, R.M. Implantable cardioverter-defibrillator placement in patients with cardiac amyloidosis. Heart Rhythm 2014, 11, 158–162. [Google Scholar] [CrossRef]
- Hartnett, J. Electrophysiological Manifestations of Cardiac Amyloidosis: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncology 2021, 3, 506–515. [Google Scholar] [CrossRef] [PubMed]
- John, R. Arrhythmias in Cardiac Amyloidosis. J. Innov. Card. Rhythm Manag. 2018, 9, 3051–3057. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Li, X.; Feng, J.; Shen, K.-N.; Tian, Z.; Sun, J.; Mao, Y.-Y.; Cao, J.; Jin, Z.-Y.; Li, J.; et al. The prognostic value of T1 mapping and late gadolinium enhancement cardiovascular magnetic resonance imaging in patients with light chain amyloidosis. J. Cardiovasc. Magn. Reson. 2018, 20, 2. [Google Scholar] [CrossRef] [PubMed]
- Fontana, M.; Pica, S.; Reant, P.; Abdel-Gadir, A.; Treibel, T.A.; Banypersad, S.M.; Maestrini, V.; Barcella, W.; Rosmini, S.; Bulluck, H.; et al. Prognostic Value of Late Gadolinium Enhancement Cardiovascular Magnetic Resonance in Cardiac Amyloidosis. Circulation 2015, 132, 1570–1579. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.A.; Kerwin, M.J.; Salerno, M. Native T1 Mapping, Extracellular Volume Mapping, and Late Gadolinium Enhancement in Cardiac Amyloidosis: A Meta-Analysis. JACC Cardiovasc. Imaging 2020, 13, 1299–1310. [Google Scholar] [CrossRef]
- Thakkar, S.; Patel, H.P.; Chowdhury, M.; Patel, K.; Kumar, A.; Arora, S.; Zahid, S.; Goel, M.; Barssoum, K.; Jain, V.; et al. Impact of Arrhythmias on Hospitalizations in Patients with Cardiac Amyloidosis. Am. J. Cardiol. 2021, 143, 125–130. [Google Scholar] [CrossRef]
- Escher, F.; Senoner, M.; Doerler, J.; Zaruba, M.M.; Messner, M.; Mussner-Seeber, C.; Ebert, M.; Ensinger, C.; Mair, A.; Kroiss, A.; et al. When and how do patients with cardiac amyloidosis die? Clin. Res. Cardiol. 2020, 109, 78–88. [Google Scholar] [CrossRef] [Green Version]
- Zeppenfeld, K.; Tfelt-Hansen, J.; de Riva, M.; Winkel, B.G.; Behr, E.R.; Blom, N.A.; Charron, P.; Corrado, D.; Dagres, N.; de Chillou, C.; et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur. Heart J. 2022, 43, 3997–4126. [Google Scholar] [CrossRef]
- Brown, M.T.; Yalamanchili, S.; Evans, S.T.; Ram, P.; Blank, E.A.; Lyle, M.A.; Merchant, F.M.; Bhatt, K.N. Ventricular arrhythmia burden and implantable cardioverter-defibrillator outcomes in transthyretin cardiac amyloidosis. Pacing Clin. Electrophysiol. 2022, 45, 443–451. [Google Scholar] [CrossRef]


{kind=link}
| Treatment | Pros | Cons |
|---|---|---|
| Anticoagulation |
|
|
| VKA vs. NOACs |
|
|
| Rate control | ||
| Current cardioversion | ||
| Rhythm control | ||
| ICD implantation |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Argirò, A.; Del Franco, A.; Mazzoni, C.; Allinovi, M.; Tomberli, A.; Tarquini, R.; Di Mario, C.; Perfetto, F.; Cappelli, F.; Zampieri, M. Arrhythmic Burden in Cardiac Amyloidosis: What We Know and What We Do Not. Biomedicines 2022, 10, 2888. https://doi.org/10.3390/biomedicines10112888
Argirò A, Del Franco A, Mazzoni C, Allinovi M, Tomberli A, Tarquini R, Di Mario C, Perfetto F, Cappelli F, Zampieri M. Arrhythmic Burden in Cardiac Amyloidosis: What We Know and What We Do Not. Biomedicines. 2022; 10(11):2888. https://doi.org/10.3390/biomedicines10112888
Chicago/Turabian StyleArgirò, Alessia, Annamaria Del Franco, Carlotta Mazzoni, Marco Allinovi, Alessia Tomberli, Roberto Tarquini, Carlo Di Mario, Federico Perfetto, Francesco Cappelli, and Mattia Zampieri. 2022. "Arrhythmic Burden in Cardiac Amyloidosis: What We Know and What We Do Not" Biomedicines 10, no. 11: 2888. https://doi.org/10.3390/biomedicines10112888