Call Girls In Andheri East Call 9920874524 Book Hot And Sexy Girls
Lecture 5 ( Hyperadrenalism pathology).pdf
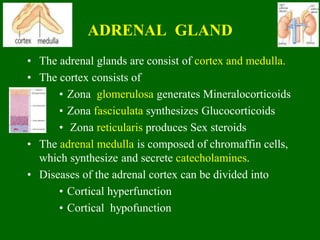
1. ADRENAL GLAND
• The adrenal glands are consist of cortex and medulla.
• The cortex consists of
• Zona glomerulosa generates Mineralocorticoids
• Zona fasciculata synthesizes Glucocorticoids
• Zona reticularis produces Sex steroids
• The adrenal medulla is composed of chromaffin cells,
which synthesize and secrete catecholamines.
• Diseases of the adrenal cortex can be divided into
• Cortical hyperfunction
• Cortical hypofunction
2. ADRENOCORTICAL HYPERFUNCTION
(HYPERADRENALISM)
There are three hyperadrenal clinical
syndromes
• Cushing syndrome (caused by an excess of
cortisol).
• Hyperaldosteronism (caused by an excess
of Aldosterone).
• Adrenogenital or virilizing syndromes
(caused an excess of androgens).
3. Hypercortisolism : Cushing Syndrome
• Hypercortisolism (Cushing syndrome) is caused by elevated
glucocorticoid levels.
• Causes of Cushing syndrome are
• Exogenous glucocorticoids
1. Iatrogenic
• Endogenous
2. Primary hypothalamic - pituitary diseases associated
with hypersecretion of ACTH.
3. The secretion of ectopic ACTH by non-pituitary
neoplasms.
4. Primary adrenocortical neoplasms (adenoma or
carcinoma) and rarely, primary cortical hyperplasia.
4. Iatrogenic Cushing
Syndrome
• Iatrogenic Cushing Syndrome results from
exogenous glucocorticoids.
• This is the most common type of Cushing
Syndrome (among all types)
• This causes suppression of endogenous ACTH
which results in bilateral cortical atrophy (due
to a lack of stimulation of the zona fasciculata
and zona reticularis by ACTH).
5. Primary Hypothalamic - Pituitary Disease
associated with hypersecretion of ACTH
(Pituitary Cushing syndrome – Cushing Disease)
• It is also known as Cushing disease.
• It accounts for approximately 70% of cases of
spontaneous, endogenous Cushing syndrome.
• The prevalence of this disorder is about four times
higher among women than among men.
• It occurs most frequently during young adulthood (the
20s and 30s).
6. Primary Hypothalamic - Pituitary
Disease associated with hypersecretion
of ACTH
• In most of cases, the pituitary gland contains an
ACTH-producing microadenoma.
• In some patients, the anterior pituitary contains areas
of corticotroph cell hyperplasia without a discrete
adenoma.
• The adrenal glands in patients with Cushing disease
are characterized by a variable degree of bilateral
nodular cortical hyperplasia, secondary to the
elevated levels of ACTH (“ACTH-dependent”
Cushing syndrome).
• The cortical hyperplasia is in turn responsible for the
hypercortisolism.
7. Secretion of Ectopic ACTH by
nonpituitary tumors
(Paraneoplastic Cushing Syndrome)
• It accounts for about 10% of cases of Cushing
syndrome.
• The following tumors are associated with this
1. Small cell carcinoma of the lung (most common)
2. Carcinoids
3. Medullary carcinomas of the thyroid
4. PanNETs
• Ectopic ACTH causes hypercortisolism.
• The adrenal glands undergo bilateral cortical
hyperplasia secondary to elevated ACTH.
8. Primary Adrenal Neoplasms
(adrenal Cushing syndrome)
• Adrenal adenoma, carcinoma, and rarely, primary
cortical hyperplasia, are responsible for about 15%
to 20% of cases of endogenous Cushing
syndrome.
• This form of Cushing syndrome is also designated
ACTH-independent Cushing syndrome, or adrenal
Cushing syndrome, because the adrenals function
autonomously.
9. Primary Adrenal Neoplasms
(adrenal Cushing syndrome)
• The biochemical hallmark of adrenal Cushing
syndrome is elevated levels of cortisol with low serum
levels of ACTH.
• In most cases, adrenal Cushing syndrome is caused by
a unilateral adrenocortical neoplasm, which may be
either benign (adenoma) or malignant (carcinoma).
10. Clinical Features
• Early manifestations of Cushing syndrome are
hypertension and weight gain.
• Truncal obesity, moon facies and accumulation of fat in
the posterior neck and back (“buffalo hump”).
• Hypercortisolism causes selective atrophy of fast-twitch
(type II) myofibers, with resultant decreased muscle
mass and proximal limb weakness.
• Glucocorticoids induce gluconeogenesis and inhibit the
uptake of glucose by cells resulting secondary diabetes
( hyperglycemia, glucosuria, and polydipsia).
11. Clinical Features
• Bone resorption results in the development of
osteoporosis, with consequent backache and
increased susceptibility to fractures.
• There is an increased risk of infections because
glucocorticoids suppress the immune response.
• Additional manifestations included Hirsutism and
menstrual abnormalities and psychiatric symptoms
including mood swings, depression, and frank
psychosis.
12. Laboratory Diagnosis of Cushing
Syndrome
It is based on the following:
1. The 24-hour urine free-cortisol concentration,
(which is increased)
2. Loss of normal diurnal pattern of cortisol
secretion.
Determining the cause of Cushing syndrome depends
on the serum ACTH and measurement of urinary
steroid excretion after administration of
dexamethasone (dexamethasone suppression test).
13. Dexamethasone Suppression Test
The results of these tests fall into three general patterns:
1. In pituitary Cushing syndrome
• The ACTH levels are elevated and cannot be
suppressed by the administration of a low dose of
dexamethasone.
• There is no reduction in urinary excretion of 17-
hydroxycorticosteroids.
• After higher doses of injected dexamethasone, the
pituitary responds by reducing ACTH secretion, which
is reflected by suppression of urinary steroid secretion.
14. Dexamethasone Suppression Test
2. Ectopic ACTH secretion
• The level of ACTH is elevated, but its secretion is
completely insensitive to low or high doses of
exogenous dexamethasone.
3. Cushing syndrome caused by an adrenal tumor
• The ACTH level is quite low because of feedback
inhibition of the pituitary. Both low-dose and high-
dose dexamethasone fail to suppress cortisol
excretion.
15. Hyperaldosteronism
• It is characterized by chronic excess aldosterone secretion.
• It may be primary, or secondary to an extraadrenal cause.
• Primary hyperaldosteronism refers to autonomous
overproduction of aldosterone, with resultant suppression
of the renin-angiotensin system and decreased plasma
renin activity.
• The causes of primary hyperaldosteronism are
1. Bilateral idiopathic hyperaldosteronism
2. Adrenocortical neoplasm
3. Familial hyperaldosteronism
16. Causes of Primary Hyperaldosteronism
1. Bilateral idiopathic hyperaldosteronism,
• This is the most common underlying cause of
primary hyperaldosteronism (about 60%of
cases).
• It is characterized by bilateral nodular
hyperplasia of the adrenal glands.
17. Causes of Primary
Hyperaldosteronism
2. Adrenocortical neoplasm
• An aldosterone-producing adenoma (the most common
cause) or, rarely, an adrenocortical carcinoma.
• In approximately 35% of cases, primary
hyperaldosteronism is caused by a solitary aldosterone-
secreting adenoma, a condition referred to as Conn
syndrome.
3. Familial hyperaldosteronism
• It may result from a genetic defect that leads to over
activity of the aldosterone synthase gene (CYP11B2)
18. Secondary Hyperaldosteronism
• In secondary hyperaldosteronism, aldosterone release
occurs in response to activation of the renin-angiotensin
system. This condition is characterized by increased
levels of plasma renin.
• Causes of secondary hyperaldosteronism are
1. Decreased renal perfusion (arteriolar
nephrosclerosis, renal artery stenosis).
2. Arterial hypovolemia and edema (congestive
heart failure, cirrhosis, nephrotic syndrome).
3. Pregnancy (caused by estrogen-induced increases
in plasma renin substrate).
19. CLINICAL FEATURES
• The clinical hallmark of hyperaldosteronism is
hypertension.
• The long-term effects of hyperaldosteronism
induced hypertension are cardiovascular
compromise (e.g., left ventricular hypertrophy )
and an increase in the prevalence of stroke and
myocardial infarction.
• Hypokalemia results from renal potassium wasting
and it can cause a variety of neuromuscular
manifestations, including weakness and
paresthesias.
20. Adrenogenital Syndromes
• This syndrome is due to excess of androgens
which may be caused by primary gonadal
disorders or primary adrenal disorders.
• Adrenal androgen formation is regulated by
ACTH.
• The excessive secretion can present as an
isolated syndrome or in combination with
features of Cushing disease.
21. Adrenogenital Syndromes
• The adrenal causes of androgen excess include
1. Adrenocortical neoplasms
2. An uncommon group of disorders collectively
designated congenital adrenal hyperplasia
(CAH).
• Adrenocortical neoplasms associated with
symptoms of androgen excess (virilization) are more
likely to be carcinomas than adenomas.
22. Congenital Adrenal Hyperplasia (CAH)
• CAH represents a group of autosomal recessive disorders,
each characterized by a hereditary defect in an enzyme
involved in adrenal steroid biosynthesis, particularly cortisol.
• In these conditions, decreased cortisol production results in a
compensatory increase in ACTH secretion due to absence of
feedback inhibition.
• The resultant adrenal hyperplasia causes increased production
of cortisol precursor steroids, which are then channeled into
synthesis of androgens with virilizing activity.
• The most common enzymatic defect in CAH is 21-
hydroxylase deficiency, which accounts for more than 90%
of cases.
23. CLINICAL FEATURES
• Excessive androgenic activity causes signs of
masculinization in females, ranging from clitoral
hypertrophy and pseudohermaphroditism in
infants to oligomenorrhea, hirsutism, and acne in
postpubertal girls.
• CAH should be suspected in any neonate with
ambiguous genitalia.
• In males, androgen excess is associated with
enlargement of the external genitalia and other
evidence of precocious puberty in prepubertal
patients.